
(PERSONALIDADE) Childhood Maltreatment Increases Risk For Personality Disorders During Early Adulthood (JAMA 1999)
(PERSONALIDADE) Childhood Maltreatment Increases Risk For Personality Disorders During Early Adulthood (JAMA 1999)
You might also like
- Mscaa Practice Paper 1 Dec2017 1 1Document29 pagesMscaa Practice Paper 1 Dec2017 1 1Helen VlotomasNo ratings yet
- Child Maltreatment and Mental Health Problems in Adulthood Birth Cohort StudyDocument6 pagesChild Maltreatment and Mental Health Problems in Adulthood Birth Cohort Studyfotosiphone 8No ratings yet
- 3 PDFDocument7 pages3 PDFAltin CeveliNo ratings yet
- Reported Pathological ChildhoodDocument7 pagesReported Pathological ChildhoodMartha Lucía Triviño LuengasNo ratings yet
- Pedi 2019 33 425Document8 pagesPedi 2019 33 425Adisty DokiNo ratings yet
- Very Early Predictors of Adolescent Depression and Suicide Attempts in Children With Attention-Deficit/Hyperactivity DisorderDocument12 pagesVery Early Predictors of Adolescent Depression and Suicide Attempts in Children With Attention-Deficit/Hyperactivity DisorderhimeNo ratings yet
- The Role of Childhood Traumatization in The Development of Borderline Personality Disorder in HungaryDocument14 pagesThe Role of Childhood Traumatization in The Development of Borderline Personality Disorder in HungaryrahafNo ratings yet
- Mental HealthDocument7 pagesMental Healthcooperpaige34No ratings yet
- Prevalence and Correlate - PreadolescenceDocument10 pagesPrevalence and Correlate - PreadolescenceFlóra FarkasNo ratings yet
- BulliedDocument13 pagesBulliedBarry BurijonNo ratings yet
- Childhood Trauma and Children's Emerging Psychotic Symptoms: A Genetically Sensitive Longitudinal Cohort StudyDocument8 pagesChildhood Trauma and Children's Emerging Psychotic Symptoms: A Genetically Sensitive Longitudinal Cohort StudyVikramjit KhangooraNo ratings yet
- HodginsDocument6 pagesHodginsFrixos StephanidesNo ratings yet
- NIH Public Access: Author ManuscriptDocument18 pagesNIH Public Access: Author ManuscriptKc RiveraNo ratings yet
- Psychotic-Like Experiences in Offspring of Parents With Bipolar Disorder and Community ControlsDocument37 pagesPsychotic-Like Experiences in Offspring of Parents With Bipolar Disorder and Community ControlsandindlNo ratings yet
- Halusi JurnalDocument16 pagesHalusi JurnalVitta ChusmeywatiNo ratings yet
- NIH Public AccessDocument13 pagesNIH Public AccessJuan Alberto GonzálezNo ratings yet
- Pedophilia JAMA 2002 Review TherapyDocument8 pagesPedophilia JAMA 2002 Review TherapyW Andrés S MedinaNo ratings yet
- AlcoooDocument8 pagesAlcooofilimon ioanaNo ratings yet
- Pediatic Acuired Immunodeficiency SyndromeDocument6 pagesPediatic Acuired Immunodeficiency Syndromeahmad iffa maududyNo ratings yet
- Body Image and Risk Behaviors in Youth With HIVDocument6 pagesBody Image and Risk Behaviors in Youth With HIVMorrison Omokiniovo Jessa SnrNo ratings yet
- Child and Adolescent Maltreatment Patterns and Risk of Eating Disorder Behaviors Developing in Young AdulthoodDocument9 pagesChild and Adolescent Maltreatment Patterns and Risk of Eating Disorder Behaviors Developing in Young AdulthoodVivian BandeiraNo ratings yet
- Early Childhood Predictors of Boys' Antisocial and Violent Behavior in Early AdulthoodDocument15 pagesEarly Childhood Predictors of Boys' Antisocial and Violent Behavior in Early AdulthoodVictoria ZorzopulosNo ratings yet
- Bourget 2007Document9 pagesBourget 2007Kiara DattaNo ratings yet
- Paranoia RolDocument1 pageParanoia RolV.pavithraNo ratings yet
- Links Between Childhood Experiences andDocument16 pagesLinks Between Childhood Experiences andgica.bucicNo ratings yet
- Development of Bipolar Disorder and Other Comorbilities en TDAHDocument7 pagesDevelopment of Bipolar Disorder and Other Comorbilities en TDAHCarla NapoliNo ratings yet
- Poorer Subjective Mental Health Among Girls: Artefact or Real? Examining Whether Interpretations of What Shapes Mental Health Vary by SexDocument14 pagesPoorer Subjective Mental Health Among Girls: Artefact or Real? Examining Whether Interpretations of What Shapes Mental Health Vary by Sexsherifgamea911No ratings yet
- (2013) - ExnerDocument10 pages(2013) - Exnerbeatriz.l.oliveira.2300No ratings yet
- Marital Status Childhood Maltreatment Family DysfunctionDocument5 pagesMarital Status Childhood Maltreatment Family DysfunctionMaria Gracia AbadNo ratings yet
- Family Rejection As A Predictor of Negative Health Outcomes in White and Latino Lesbian, Gay, and Bisexual Young AdultsDocument9 pagesFamily Rejection As A Predictor of Negative Health Outcomes in White and Latino Lesbian, Gay, and Bisexual Young AdultsMuhammad Naufal FirdausNo ratings yet
- Childhood Bulling Involvement Predicts Low Grade Systemic InflammationDocument6 pagesChildhood Bulling Involvement Predicts Low Grade Systemic InflammationCristiana ComanNo ratings yet
- Running Head: MENTAL DISORDERS 1Document12 pagesRunning Head: MENTAL DISORDERS 1api-532509198No ratings yet
- Child and Adolescent Abuse and Neglect ResearchDocument9 pagesChild and Adolescent Abuse and Neglect ResearchKübraNo ratings yet
- Fruzzetti 2005 OptionalDocument24 pagesFruzzetti 2005 OptionalMacovei Anca0% (1)
- Infant Behavioral Inhibition Predicts Personality and Social Outcomes Three Decades LaterDocument8 pagesInfant Behavioral Inhibition Predicts Personality and Social Outcomes Three Decades LaterTaakeNo ratings yet
- Kendler-Childhood Parental Loss.1992Document8 pagesKendler-Childhood Parental Loss.1992Zsófia OtolticsNo ratings yet
- Family Characteristics and Behavior Problems of Suicidal and Non-Suicidal Children and AdolescentsDocument14 pagesFamily Characteristics and Behavior Problems of Suicidal and Non-Suicidal Children and AdolescentssaNo ratings yet
- 122 Full PDFDocument8 pages122 Full PDFcassieNo ratings yet
- Wood 1976Document8 pagesWood 1976Arif Erdem KöroğluNo ratings yet
- Duffy2013 PDFDocument8 pagesDuffy2013 PDFFelipe VergaraNo ratings yet
- Childhood Abuse, Neglect, and Household Dysfunction and The Risk ofDocument11 pagesChildhood Abuse, Neglect, and Household Dysfunction and The Risk ofDianaBNo ratings yet
- The Behavior of Anxious Parents Examining Mechanisms of Transmission of Anxiety From Parent To ChildDocument12 pagesThe Behavior of Anxious Parents Examining Mechanisms of Transmission of Anxiety From Parent To Child方科惠No ratings yet
- US National Longitudinal Lesbian Family Study: Psychological Adjustment of 17-Year-Old AdolescentsDocument11 pagesUS National Longitudinal Lesbian Family Study: Psychological Adjustment of 17-Year-Old AdolescentsGloria StahlNo ratings yet
- The Legacy of Child Maltreatment: Long-Term Health Consequences For WomenDocument6 pagesThe Legacy of Child Maltreatment: Long-Term Health Consequences For WomenRavennaNo ratings yet
- Young Children: Preventing Physical Abuse and Corporal Punishment (2014)Document7 pagesYoung Children: Preventing Physical Abuse and Corporal Punishment (2014)Children's InstituteNo ratings yet
- Adolescent DepressionDocument14 pagesAdolescent DepressionEduardo CañedoNo ratings yet
- Rates of Nonsuicidal Self-Injury in YouthDocument9 pagesRates of Nonsuicidal Self-Injury in YouthWilson Javier Dominguez PerezNo ratings yet
- Bullying Behaviors Among US Youth: Prevalence and Association With Psychosocial AdjustmentDocument13 pagesBullying Behaviors Among US Youth: Prevalence and Association With Psychosocial AdjustmentAna FerreiraNo ratings yet
- Quantitativo Bullying Maip PDFDocument13 pagesQuantitativo Bullying Maip PDFAna FerreiraNo ratings yet
- (696557968) Sifra JurnalDocument9 pages(696557968) Sifra JurnalSifra Turu AlloNo ratings yet
- Pedophilia and DSM-5: The Importance of Clearly Defining The Nature of A Pedophilic DisorderDocument4 pagesPedophilia and DSM-5: The Importance of Clearly Defining The Nature of A Pedophilic DisorderEmy Noviana SandyNo ratings yet
- Gri Zenko 1994Document11 pagesGri Zenko 1994Alex BoncuNo ratings yet
- Sills 2007Document10 pagesSills 2007hotorunNo ratings yet
- Risk of Mental Illness in Offspring of Parents With Schizophrenia, BipolarDocument11 pagesRisk of Mental Illness in Offspring of Parents With Schizophrenia, BipolarOkta BarraNo ratings yet
- Associations Between Four Types of Childhood Neglect and Personality Disorder Symptoms During Adolescence and Early Adulthood: Findings of A Community-Based Longitudinal StudyDocument17 pagesAssociations Between Four Types of Childhood Neglect and Personality Disorder Symptoms During Adolescence and Early Adulthood: Findings of A Community-Based Longitudinal StudyUmer FarooqNo ratings yet
- AmericanDocument13 pagesAmericanDavid QatamadzeNo ratings yet
- Lister, 2015Document7 pagesLister, 2015Bianca HlepcoNo ratings yet
- NIH Public Access: Author ManuscriptDocument15 pagesNIH Public Access: Author Manuscriptyeremias setyawanNo ratings yet
- Risk Factors in Early Life For Developmental Coordination Disorder: A Scoping ReviewDocument9 pagesRisk Factors in Early Life For Developmental Coordination Disorder: A Scoping ReviewLaura RodriguezNo ratings yet
- Danckaerts2000 Article ANaturalHistoryOfHyperactivityDocument13 pagesDanckaerts2000 Article ANaturalHistoryOfHyperactivitymaksim6098No ratings yet
- Behind the Mask: Revealing the Risk Factors of Psychopathy in Children and AdolescentsFrom EverandBehind the Mask: Revealing the Risk Factors of Psychopathy in Children and AdolescentsNo ratings yet
- PharmacologyDocument141 pagesPharmacologyOmowunmi KadriNo ratings yet
- Endocrine Function Report Ncm114Document91 pagesEndocrine Function Report Ncm114abcde pwnjabiNo ratings yet
- Genetic Mutation and DisorderDocument31 pagesGenetic Mutation and Disorderabrielle dytucoNo ratings yet
- Disfagia Esofágica en Niños. Estado Del Arte y Propuesta para Un Enfoque Diagnóstico Basado en Los Síntomas (2022)Document12 pagesDisfagia Esofágica en Niños. Estado Del Arte y Propuesta para Un Enfoque Diagnóstico Basado en Los Síntomas (2022)7 MNTNo ratings yet
- DebateDocument12 pagesDebate•Kai yiii•No ratings yet
- CSB043 Prostate EBRT 2016 PCDocument53 pagesCSB043 Prostate EBRT 2016 PCPeter CaldwellNo ratings yet
- 3 Interview Transcripts From The Leaky Brain SummitDocument39 pages3 Interview Transcripts From The Leaky Brain SummitJimmy SchibelloNo ratings yet
- Stages of Acute Otitis MediaDocument1 pageStages of Acute Otitis MediaNicole Marie NicolasNo ratings yet
- Cancer WebquestDocument2 pagesCancer WebquestAmaia FiolNo ratings yet
- Overview of Viral MyositisDocument3 pagesOverview of Viral MyositisemirkurtalicNo ratings yet
- Substance-Related Disorders: Professor DR Sirwan K Ali Department of PsychiatryDocument43 pagesSubstance-Related Disorders: Professor DR Sirwan K Ali Department of PsychiatryAlan AhmadNo ratings yet
- Living With AdhdDocument3 pagesLiving With Adhdapi-704337450No ratings yet
- 1 s2.0 S0300289621001745 mmc2Document2 pages1 s2.0 S0300289621001745 mmc2aris dwiprasetyaNo ratings yet
- GREGORY - Demencia Rápidamente ProgresivaDocument47 pagesGREGORY - Demencia Rápidamente ProgresivaUgalde López ReginaNo ratings yet
- ICD 10 CM Coding - DiabetesDocument68 pagesICD 10 CM Coding - Diabeteschaitanya varmaNo ratings yet
- Asco Treatment Summary and Survivorship Care PlanDocument2 pagesAsco Treatment Summary and Survivorship Care PlanFriska Permatasari NababanNo ratings yet
- 05 - 2022 ISI Short Term Application Form - EnglishDocument2 pages05 - 2022 ISI Short Term Application Form - EnglishPapitcha chittipornsanNo ratings yet
- Initation of Insulin - Final 2023Document27 pagesInitation of Insulin - Final 2023DEWI RIZKI AGUSTINANo ratings yet
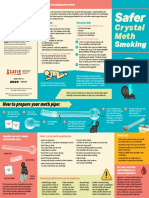
- CATIE SaferSmoking CrystalMeth E 2020 FINAL WEBDocument2 pagesCATIE SaferSmoking CrystalMeth E 2020 FINAL WEBJeff PuglisiNo ratings yet
- The Accuracy of Fibroscan in A Real World StudyDocument2 pagesThe Accuracy of Fibroscan in A Real World StudyRaeni Dwi PutriNo ratings yet
- Juni 23 1Document105 pagesJuni 23 1Isabella MebangNo ratings yet
- Whipple Procedure: Procedure at A GlanceDocument4 pagesWhipple Procedure: Procedure at A GlanceAze Andrea PutraNo ratings yet
- نماذج باثو نظري هيكليDocument2 pagesنماذج باثو نظري هيكليWael EssaNo ratings yet
- OSCE Medicine by DR BilanDocument77 pagesOSCE Medicine by DR BilanBukhaari MohamedNo ratings yet
- M1 Post Task - Caparas-Bsn2a-A2Document2 pagesM1 Post Task - Caparas-Bsn2a-A2Gretta CaparasNo ratings yet
- Tatalaksana Primary Dan Secondary SurveyDocument26 pagesTatalaksana Primary Dan Secondary Surveyakun 31No ratings yet
- BMJ 22-09Document15 pagesBMJ 22-09Kiran ShahNo ratings yet
- DOLOCAN Dolocem CBD Eczema Cream White Paper - 20190917Document1 pageDOLOCAN Dolocem CBD Eczema Cream White Paper - 20190917Petra MitićNo ratings yet
- Homeopathic Heritage February Issue 2024Document94 pagesHomeopathic Heritage February Issue 2024Sumanta KamilaNo ratings yet
























































































Download as pdf or txt
You might also like
- Mscaa Practice Paper 1 Dec2017 1 1Document29 pagesMscaa Practice Paper 1 Dec2017 1 1Helen VlotomasNo ratings yet
- Child Maltreatment and Mental Health Problems in Adulthood Birth Cohort StudyDocument6 pagesChild Maltreatment and Mental Health Problems in Adulthood Birth Cohort Studyfotosiphone 8No ratings yet
- 3 PDFDocument7 pages3 PDFAltin CeveliNo ratings yet
- Reported Pathological ChildhoodDocument7 pagesReported Pathological ChildhoodMartha Lucía Triviño LuengasNo ratings yet
- Pedi 2019 33 425Document8 pagesPedi 2019 33 425Adisty DokiNo ratings yet
- Very Early Predictors of Adolescent Depression and Suicide Attempts in Children With Attention-Deficit/Hyperactivity DisorderDocument12 pagesVery Early Predictors of Adolescent Depression and Suicide Attempts in Children With Attention-Deficit/Hyperactivity DisorderhimeNo ratings yet
- The Role of Childhood Traumatization in The Development of Borderline Personality Disorder in HungaryDocument14 pagesThe Role of Childhood Traumatization in The Development of Borderline Personality Disorder in HungaryrahafNo ratings yet
- Mental HealthDocument7 pagesMental Healthcooperpaige34No ratings yet
- Prevalence and Correlate - PreadolescenceDocument10 pagesPrevalence and Correlate - PreadolescenceFlóra FarkasNo ratings yet
- BulliedDocument13 pagesBulliedBarry BurijonNo ratings yet
- Childhood Trauma and Children's Emerging Psychotic Symptoms: A Genetically Sensitive Longitudinal Cohort StudyDocument8 pagesChildhood Trauma and Children's Emerging Psychotic Symptoms: A Genetically Sensitive Longitudinal Cohort StudyVikramjit KhangooraNo ratings yet
- HodginsDocument6 pagesHodginsFrixos StephanidesNo ratings yet
- NIH Public Access: Author ManuscriptDocument18 pagesNIH Public Access: Author ManuscriptKc RiveraNo ratings yet
- Psychotic-Like Experiences in Offspring of Parents With Bipolar Disorder and Community ControlsDocument37 pagesPsychotic-Like Experiences in Offspring of Parents With Bipolar Disorder and Community ControlsandindlNo ratings yet
- Halusi JurnalDocument16 pagesHalusi JurnalVitta ChusmeywatiNo ratings yet
- NIH Public AccessDocument13 pagesNIH Public AccessJuan Alberto GonzálezNo ratings yet
- Pedophilia JAMA 2002 Review TherapyDocument8 pagesPedophilia JAMA 2002 Review TherapyW Andrés S MedinaNo ratings yet
- AlcoooDocument8 pagesAlcooofilimon ioanaNo ratings yet
- Pediatic Acuired Immunodeficiency SyndromeDocument6 pagesPediatic Acuired Immunodeficiency Syndromeahmad iffa maududyNo ratings yet
- Body Image and Risk Behaviors in Youth With HIVDocument6 pagesBody Image and Risk Behaviors in Youth With HIVMorrison Omokiniovo Jessa SnrNo ratings yet
- Child and Adolescent Maltreatment Patterns and Risk of Eating Disorder Behaviors Developing in Young AdulthoodDocument9 pagesChild and Adolescent Maltreatment Patterns and Risk of Eating Disorder Behaviors Developing in Young AdulthoodVivian BandeiraNo ratings yet
- Early Childhood Predictors of Boys' Antisocial and Violent Behavior in Early AdulthoodDocument15 pagesEarly Childhood Predictors of Boys' Antisocial and Violent Behavior in Early AdulthoodVictoria ZorzopulosNo ratings yet
- Bourget 2007Document9 pagesBourget 2007Kiara DattaNo ratings yet
- Paranoia RolDocument1 pageParanoia RolV.pavithraNo ratings yet
- Links Between Childhood Experiences andDocument16 pagesLinks Between Childhood Experiences andgica.bucicNo ratings yet
- Development of Bipolar Disorder and Other Comorbilities en TDAHDocument7 pagesDevelopment of Bipolar Disorder and Other Comorbilities en TDAHCarla NapoliNo ratings yet
- Poorer Subjective Mental Health Among Girls: Artefact or Real? Examining Whether Interpretations of What Shapes Mental Health Vary by SexDocument14 pagesPoorer Subjective Mental Health Among Girls: Artefact or Real? Examining Whether Interpretations of What Shapes Mental Health Vary by Sexsherifgamea911No ratings yet
- (2013) - ExnerDocument10 pages(2013) - Exnerbeatriz.l.oliveira.2300No ratings yet
- Marital Status Childhood Maltreatment Family DysfunctionDocument5 pagesMarital Status Childhood Maltreatment Family DysfunctionMaria Gracia AbadNo ratings yet
- Family Rejection As A Predictor of Negative Health Outcomes in White and Latino Lesbian, Gay, and Bisexual Young AdultsDocument9 pagesFamily Rejection As A Predictor of Negative Health Outcomes in White and Latino Lesbian, Gay, and Bisexual Young AdultsMuhammad Naufal FirdausNo ratings yet
- Childhood Bulling Involvement Predicts Low Grade Systemic InflammationDocument6 pagesChildhood Bulling Involvement Predicts Low Grade Systemic InflammationCristiana ComanNo ratings yet
- Running Head: MENTAL DISORDERS 1Document12 pagesRunning Head: MENTAL DISORDERS 1api-532509198No ratings yet
- Child and Adolescent Abuse and Neglect ResearchDocument9 pagesChild and Adolescent Abuse and Neglect ResearchKübraNo ratings yet
- Fruzzetti 2005 OptionalDocument24 pagesFruzzetti 2005 OptionalMacovei Anca0% (1)
- Infant Behavioral Inhibition Predicts Personality and Social Outcomes Three Decades LaterDocument8 pagesInfant Behavioral Inhibition Predicts Personality and Social Outcomes Three Decades LaterTaakeNo ratings yet
- Kendler-Childhood Parental Loss.1992Document8 pagesKendler-Childhood Parental Loss.1992Zsófia OtolticsNo ratings yet
- Family Characteristics and Behavior Problems of Suicidal and Non-Suicidal Children and AdolescentsDocument14 pagesFamily Characteristics and Behavior Problems of Suicidal and Non-Suicidal Children and AdolescentssaNo ratings yet
- 122 Full PDFDocument8 pages122 Full PDFcassieNo ratings yet
- Wood 1976Document8 pagesWood 1976Arif Erdem KöroğluNo ratings yet
- Duffy2013 PDFDocument8 pagesDuffy2013 PDFFelipe VergaraNo ratings yet
- Childhood Abuse, Neglect, and Household Dysfunction and The Risk ofDocument11 pagesChildhood Abuse, Neglect, and Household Dysfunction and The Risk ofDianaBNo ratings yet
- The Behavior of Anxious Parents Examining Mechanisms of Transmission of Anxiety From Parent To ChildDocument12 pagesThe Behavior of Anxious Parents Examining Mechanisms of Transmission of Anxiety From Parent To Child方科惠No ratings yet
- US National Longitudinal Lesbian Family Study: Psychological Adjustment of 17-Year-Old AdolescentsDocument11 pagesUS National Longitudinal Lesbian Family Study: Psychological Adjustment of 17-Year-Old AdolescentsGloria StahlNo ratings yet
- The Legacy of Child Maltreatment: Long-Term Health Consequences For WomenDocument6 pagesThe Legacy of Child Maltreatment: Long-Term Health Consequences For WomenRavennaNo ratings yet
- Young Children: Preventing Physical Abuse and Corporal Punishment (2014)Document7 pagesYoung Children: Preventing Physical Abuse and Corporal Punishment (2014)Children's InstituteNo ratings yet
- Adolescent DepressionDocument14 pagesAdolescent DepressionEduardo CañedoNo ratings yet
- Rates of Nonsuicidal Self-Injury in YouthDocument9 pagesRates of Nonsuicidal Self-Injury in YouthWilson Javier Dominguez PerezNo ratings yet
- Bullying Behaviors Among US Youth: Prevalence and Association With Psychosocial AdjustmentDocument13 pagesBullying Behaviors Among US Youth: Prevalence and Association With Psychosocial AdjustmentAna FerreiraNo ratings yet
- Quantitativo Bullying Maip PDFDocument13 pagesQuantitativo Bullying Maip PDFAna FerreiraNo ratings yet
- (696557968) Sifra JurnalDocument9 pages(696557968) Sifra JurnalSifra Turu AlloNo ratings yet
- Pedophilia and DSM-5: The Importance of Clearly Defining The Nature of A Pedophilic DisorderDocument4 pagesPedophilia and DSM-5: The Importance of Clearly Defining The Nature of A Pedophilic DisorderEmy Noviana SandyNo ratings yet
- Gri Zenko 1994Document11 pagesGri Zenko 1994Alex BoncuNo ratings yet
- Sills 2007Document10 pagesSills 2007hotorunNo ratings yet
- Risk of Mental Illness in Offspring of Parents With Schizophrenia, BipolarDocument11 pagesRisk of Mental Illness in Offspring of Parents With Schizophrenia, BipolarOkta BarraNo ratings yet
- Associations Between Four Types of Childhood Neglect and Personality Disorder Symptoms During Adolescence and Early Adulthood: Findings of A Community-Based Longitudinal StudyDocument17 pagesAssociations Between Four Types of Childhood Neglect and Personality Disorder Symptoms During Adolescence and Early Adulthood: Findings of A Community-Based Longitudinal StudyUmer FarooqNo ratings yet
- AmericanDocument13 pagesAmericanDavid QatamadzeNo ratings yet
- Lister, 2015Document7 pagesLister, 2015Bianca HlepcoNo ratings yet
- NIH Public Access: Author ManuscriptDocument15 pagesNIH Public Access: Author Manuscriptyeremias setyawanNo ratings yet
- Risk Factors in Early Life For Developmental Coordination Disorder: A Scoping ReviewDocument9 pagesRisk Factors in Early Life For Developmental Coordination Disorder: A Scoping ReviewLaura RodriguezNo ratings yet
- Danckaerts2000 Article ANaturalHistoryOfHyperactivityDocument13 pagesDanckaerts2000 Article ANaturalHistoryOfHyperactivitymaksim6098No ratings yet
- Behind the Mask: Revealing the Risk Factors of Psychopathy in Children and AdolescentsFrom EverandBehind the Mask: Revealing the Risk Factors of Psychopathy in Children and AdolescentsNo ratings yet
- PharmacologyDocument141 pagesPharmacologyOmowunmi KadriNo ratings yet
- Endocrine Function Report Ncm114Document91 pagesEndocrine Function Report Ncm114abcde pwnjabiNo ratings yet
- Genetic Mutation and DisorderDocument31 pagesGenetic Mutation and Disorderabrielle dytucoNo ratings yet
- Disfagia Esofágica en Niños. Estado Del Arte y Propuesta para Un Enfoque Diagnóstico Basado en Los Síntomas (2022)Document12 pagesDisfagia Esofágica en Niños. Estado Del Arte y Propuesta para Un Enfoque Diagnóstico Basado en Los Síntomas (2022)7 MNTNo ratings yet
- DebateDocument12 pagesDebate•Kai yiii•No ratings yet
- CSB043 Prostate EBRT 2016 PCDocument53 pagesCSB043 Prostate EBRT 2016 PCPeter CaldwellNo ratings yet
- 3 Interview Transcripts From The Leaky Brain SummitDocument39 pages3 Interview Transcripts From The Leaky Brain SummitJimmy SchibelloNo ratings yet
- Stages of Acute Otitis MediaDocument1 pageStages of Acute Otitis MediaNicole Marie NicolasNo ratings yet
- Cancer WebquestDocument2 pagesCancer WebquestAmaia FiolNo ratings yet
- Overview of Viral MyositisDocument3 pagesOverview of Viral MyositisemirkurtalicNo ratings yet
- Substance-Related Disorders: Professor DR Sirwan K Ali Department of PsychiatryDocument43 pagesSubstance-Related Disorders: Professor DR Sirwan K Ali Department of PsychiatryAlan AhmadNo ratings yet
- Living With AdhdDocument3 pagesLiving With Adhdapi-704337450No ratings yet
- 1 s2.0 S0300289621001745 mmc2Document2 pages1 s2.0 S0300289621001745 mmc2aris dwiprasetyaNo ratings yet
- GREGORY - Demencia Rápidamente ProgresivaDocument47 pagesGREGORY - Demencia Rápidamente ProgresivaUgalde López ReginaNo ratings yet
- ICD 10 CM Coding - DiabetesDocument68 pagesICD 10 CM Coding - Diabeteschaitanya varmaNo ratings yet
- Asco Treatment Summary and Survivorship Care PlanDocument2 pagesAsco Treatment Summary and Survivorship Care PlanFriska Permatasari NababanNo ratings yet
- 05 - 2022 ISI Short Term Application Form - EnglishDocument2 pages05 - 2022 ISI Short Term Application Form - EnglishPapitcha chittipornsanNo ratings yet
- Initation of Insulin - Final 2023Document27 pagesInitation of Insulin - Final 2023DEWI RIZKI AGUSTINANo ratings yet
- CATIE SaferSmoking CrystalMeth E 2020 FINAL WEBDocument2 pagesCATIE SaferSmoking CrystalMeth E 2020 FINAL WEBJeff PuglisiNo ratings yet
- The Accuracy of Fibroscan in A Real World StudyDocument2 pagesThe Accuracy of Fibroscan in A Real World StudyRaeni Dwi PutriNo ratings yet
- Juni 23 1Document105 pagesJuni 23 1Isabella MebangNo ratings yet
- Whipple Procedure: Procedure at A GlanceDocument4 pagesWhipple Procedure: Procedure at A GlanceAze Andrea PutraNo ratings yet
- نماذج باثو نظري هيكليDocument2 pagesنماذج باثو نظري هيكليWael EssaNo ratings yet
- OSCE Medicine by DR BilanDocument77 pagesOSCE Medicine by DR BilanBukhaari MohamedNo ratings yet
- M1 Post Task - Caparas-Bsn2a-A2Document2 pagesM1 Post Task - Caparas-Bsn2a-A2Gretta CaparasNo ratings yet
- Tatalaksana Primary Dan Secondary SurveyDocument26 pagesTatalaksana Primary Dan Secondary Surveyakun 31No ratings yet
- BMJ 22-09Document15 pagesBMJ 22-09Kiran ShahNo ratings yet
- DOLOCAN Dolocem CBD Eczema Cream White Paper - 20190917Document1 pageDOLOCAN Dolocem CBD Eczema Cream White Paper - 20190917Petra MitićNo ratings yet
- Homeopathic Heritage February Issue 2024Document94 pagesHomeopathic Heritage February Issue 2024Sumanta KamilaNo ratings yet