Download as pdf or txt
You might also like
- Key Points/: Study GuideDocument48 pagesKey Points/: Study Guidedanni100% (1)
- Chapter 17 INTERPRETING ELECROCARDIOGRAMDocument7 pagesChapter 17 INTERPRETING ELECROCARDIOGRAMZahra Margrette SchuckNo ratings yet
- ECG/EKG Interpretation: An Easy Approach to Read a 12-Lead ECG and How to Diagnose and Treat ArrhythmiasFrom EverandECG/EKG Interpretation: An Easy Approach to Read a 12-Lead ECG and How to Diagnose and Treat ArrhythmiasRating: 5 out of 5 stars5/5 (2)
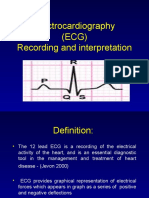
- Electrocardiography (ECG) Recording and InterpretationDocument59 pagesElectrocardiography (ECG) Recording and Interpretationkhushsandhu0% (1)
- Cardiovascular Assessment ChecklistDocument2 pagesCardiovascular Assessment Checklistvishnu100% (3)
- Soap For Atrial FibrillationDocument6 pagesSoap For Atrial FibrillationSombolayuk PriskaNo ratings yet
- Basic Ecg Interpretation and Arrhythmia Recognition By: Ma. Victoria E. Martinez Er - RNDocument34 pagesBasic Ecg Interpretation and Arrhythmia Recognition By: Ma. Victoria E. Martinez Er - RNMavic Martinez BuntalesNo ratings yet
- Electrocardiography: DR Uwanuruochi KelechukwuDocument50 pagesElectrocardiography: DR Uwanuruochi KelechukwuJake MillerNo ratings yet
- How Procedure Is Performed: ElectrocardiogramDocument10 pagesHow Procedure Is Performed: ElectrocardiogramJonathan AlvarezNo ratings yet
- Electrophysiology of The HeartDocument27 pagesElectrophysiology of The HeartTsegaye HailuNo ratings yet
- Ecg Treadmill and Holter TestDocument77 pagesEcg Treadmill and Holter TestRiteka Singh100% (1)
- Electrocardiogram (ECG) : This Is The Lecture No. 4Document51 pagesElectrocardiogram (ECG) : This Is The Lecture No. 4Aboodsha ShNo ratings yet
- ECG InterpretationDocument73 pagesECG Interpretationsultan khabeebNo ratings yet
- ECGs The Basics (Part 1) LectureDocument32 pagesECGs The Basics (Part 1) Lectureliudmyla zakordonetsNo ratings yet
- Electrical Activity of The HeartDocument156 pagesElectrical Activity of The HeartNIRANJANA SHALININo ratings yet
- Electrical Impulse Viewed: Interpretation of The ElectrocardiogramDocument41 pagesElectrical Impulse Viewed: Interpretation of The ElectrocardiogramNesru Ahmed AkkichuNo ratings yet
- EcgDocument29 pagesEcgSouvikDattaNo ratings yet
- Electrocardiography: An Introduction To The ECGDocument76 pagesElectrocardiography: An Introduction To The ECGInnocent Clifford MaranduNo ratings yet
- How To Read An EcgDocument86 pagesHow To Read An EcgmajdNo ratings yet
- ECG1Document67 pagesECG1Farhan RosliNo ratings yet
- Santosh DevDocument45 pagesSantosh Devdevdsantosh100% (1)
- Ecg 1Document198 pagesEcg 1hibaNo ratings yet
- ECGs The Basics (Part 1) LectureDocument33 pagesECGs The Basics (Part 1) Lectureliudmyla zakordonetsNo ratings yet
- Base of The ElectrocardiogramDocument15 pagesBase of The ElectrocardiogramPutri AfisiaNo ratings yet
- Unit-2 ECG LNRDocument29 pagesUnit-2 ECG LNRNagarajan LNo ratings yet
- Electrocardiogram: Edit By: Pea Vuthy Edited From: CMMC/JHDocument42 pagesElectrocardiogram: Edit By: Pea Vuthy Edited From: CMMC/JHNorPhea - នភាNo ratings yet
- Cardiac Arrhythmia & Basics ECGDocument79 pagesCardiac Arrhythmia & Basics ECGMazhar UllahNo ratings yet
- Normal Sinus RhythmDocument48 pagesNormal Sinus RhythmStella mNo ratings yet
- The Wiring Diagram of The HeartDocument4 pagesThe Wiring Diagram of The Heartgurneet kourNo ratings yet
- Electrocardiogram (2022) )Document128 pagesElectrocardiogram (2022) )Craft Hachz By dhiyaNo ratings yet
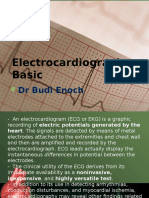
- Electrocardiography Basic: DR Budi EnochDocument49 pagesElectrocardiography Basic: DR Budi EnochYohanes Malindo Wiyaa DBs-uno100% (1)
- MUCLecture 2021 1292271Document34 pagesMUCLecture 2021 1292271Kouka MahfoudiNo ratings yet
- Lecture On Basics of ECG For 1st Year MBBS by Dr. RoomiDocument28 pagesLecture On Basics of ECG For 1st Year MBBS by Dr. RoomiMudassar Roomi100% (3)
- Ecg 2Document46 pagesEcg 2niamh traceyNo ratings yet
- ECG Basics Module-1Document127 pagesECG Basics Module-1manyusinghNo ratings yet
- EcgDocument18 pagesEcgmyla adapNo ratings yet
- Electrocardiography: DR Budi EnochDocument115 pagesElectrocardiography: DR Budi EnochAriyanaNo ratings yet
- ECG EKG: BasicsDocument191 pagesECG EKG: BasicsSabio DenmenNo ratings yet
- The Electrocardiogram: Ecg: by Gaurishi Agarwal, 32Document17 pagesThe Electrocardiogram: Ecg: by Gaurishi Agarwal, 32Gaurishi AgarwalNo ratings yet
- Ecg Physio LectureDocument60 pagesEcg Physio LectureAninze Chidera100% (1)
- Peer 2 Im1Document9 pagesPeer 2 Im1fabrahamNo ratings yet
- Ecg BSTDocument204 pagesEcg BSTAnusha Verghese100% (1)
- Basic EKG InterpretationDocument48 pagesBasic EKG InterpretationAimee Ann Pauco MacaraegNo ratings yet
- 321 Lecture ECGDocument38 pages321 Lecture ECGCea Mikee Mitch BartolomeNo ratings yet
- DrAbnet ECG - BasicsDocument99 pagesDrAbnet ECG - BasicsAbnet WondimuNo ratings yet
- Lectro Ardio Raphy: by Dr. Omprakash Sah Medical Officer NAMS, Bir HospitalDocument162 pagesLectro Ardio Raphy: by Dr. Omprakash Sah Medical Officer NAMS, Bir HospitalAjay SharmaNo ratings yet
- JHGJHGHJDocument112 pagesJHGJHGHJHello VintunnaraNo ratings yet
- Ecg Interpretation: Gowtham Krishna JDocument60 pagesEcg Interpretation: Gowtham Krishna JGowtham KrishnaNo ratings yet
- Electrical TimeDocument14 pagesElectrical TimeNithyaa SathishNo ratings yet
- Lab Exercise 5 PDFDocument50 pagesLab Exercise 5 PDFE1- Villapaz, Aiemarie R. (Aie)No ratings yet
- Electrical Activity of The HeartDocument40 pagesElectrical Activity of The HeartMichael Ajak GhaiNo ratings yet
- ECGDocument62 pagesECGSanju TanwarNo ratings yet
- Electrocardiography: Dr. Anand PatelDocument155 pagesElectrocardiography: Dr. Anand PatelDeepika PatelNo ratings yet
- ECG Made Easy For Allied Health ProfessionalsDocument47 pagesECG Made Easy For Allied Health ProfessionalsDr GowrishankarPotturi PT100% (3)
- Lec7 Sem2 CVSWK3 20140920 PDFDocument12 pagesLec7 Sem2 CVSWK3 20140920 PDFAprina RosyadahNo ratings yet
- Asist. Univ. Dr. Mihaela Popescu Catedra de Cardiologie Spitalul Universitar de Urgenta EliasDocument64 pagesAsist. Univ. Dr. Mihaela Popescu Catedra de Cardiologie Spitalul Universitar de Urgenta EliasAnonymous CQmrhq1O7No ratings yet
- Ecg Interpretation: Presented by:-ROHINI RAI M SC Nursing Part I, C.O.N, N.B.M.C.HDocument69 pagesEcg Interpretation: Presented by:-ROHINI RAI M SC Nursing Part I, C.O.N, N.B.M.C.HRohini RaiNo ratings yet
- Ecg or Electro Cardiogram and ElectrocardiographDocument20 pagesEcg or Electro Cardiogram and ElectrocardiographsureshNo ratings yet
- Basic Principles of ECGDocument53 pagesBasic Principles of ECGSmita Jain100% (1)
- Ecg PresentationDocument27 pagesEcg Presentationanish3189No ratings yet
- ECG PracticalDocument48 pagesECG PracticalbvkjtzrvnyNo ratings yet
- Basics of ECG: DR Subroto Mandal, MD, DM, DC Associate Professor, CardiologyDocument206 pagesBasics of ECG: DR Subroto Mandal, MD, DM, DC Associate Professor, CardiologyRavi SharmaNo ratings yet
- Introduction To ElectrocardiogramDocument46 pagesIntroduction To ElectrocardiogramEba DadoughNo ratings yet
- Pagewriter Xli Users GuideDocument129 pagesPagewriter Xli Users Guidemebme2022No ratings yet
- Heart Failure Pelatihan Dokter KeluargaDocument55 pagesHeart Failure Pelatihan Dokter KeluargaDelia NingrumNo ratings yet
- Ad 8232Document8 pagesAd 8232umairNo ratings yet
- Ficha 12 - Pulse RateDocument2 pagesFicha 12 - Pulse Ratejorgitoperu2014100% (1)
- Rhythm Summary Review Packet EKG CLassDocument12 pagesRhythm Summary Review Packet EKG CLassmisslhen.rn04No ratings yet
- Systematic Approach To ECGDocument12 pagesSystematic Approach To ECGAmr El TaherNo ratings yet
- Athlete's Heart: Dr. Arzalan BaigDocument59 pagesAthlete's Heart: Dr. Arzalan BaigArzalan BaigNo ratings yet
- OSPE No. 01: Examine Ther Radial Artery Pulse. Step Expected Duration ScoreDocument4 pagesOSPE No. 01: Examine Ther Radial Artery Pulse. Step Expected Duration ScoreKhaled Abdel-saterNo ratings yet
- The Kiss of The Girl From IpanemaDocument4 pagesThe Kiss of The Girl From IpanemaDrMarcus KeyboardNo ratings yet
- CardioDocument48 pagesCardiomalisalukmanNo ratings yet
- Mobile Coronary Care UnitDocument16 pagesMobile Coronary Care UnitArcha100% (2)
- Classification of Sports: Type of Exercise PerformedDocument2 pagesClassification of Sports: Type of Exercise PerformedAnh MinhNo ratings yet
- An Easy Guide To Head To Toe Assessment Vrtis 2011-1 PDFDocument6 pagesAn Easy Guide To Head To Toe Assessment Vrtis 2011-1 PDFkatherine dayagNo ratings yet
- Interpretation: Certificate Courses OnDocument2 pagesInterpretation: Certificate Courses OnKamleshNo ratings yet
- Nursing School EKGDocument43 pagesNursing School EKGRob Dickerson100% (1)
- Drugs Used in Cardiac EmergenciesDocument18 pagesDrugs Used in Cardiac Emergencieshakky gamyNo ratings yet
- The Wiggers DiagramDocument2 pagesThe Wiggers DiagramKuro ShiroNo ratings yet
- AbijitDocument3 pagesAbijitvimalNo ratings yet
- The Pathophysiology of Congestive Heart FailureDocument3 pagesThe Pathophysiology of Congestive Heart FailureDennis KimNo ratings yet
- GREY BOOK August 2022 75th EditionDocument155 pagesGREY BOOK August 2022 75th EditionMohamed AbdelmoniemNo ratings yet
- Hemodynamic Parameters To Guide Fluid Therapy: Review Open AccessDocument9 pagesHemodynamic Parameters To Guide Fluid Therapy: Review Open AccessClaudioValdiviaNo ratings yet
- A Student'S Guide To The Interpretation of Ecgs: by Richard MckearneyDocument12 pagesA Student'S Guide To The Interpretation of Ecgs: by Richard MckearneyEba'a GamilNo ratings yet
- Atrial Fibrillation and Congestive Heart Failure: EditorialDocument3 pagesAtrial Fibrillation and Congestive Heart Failure: EditorialfederikarosilawatiNo ratings yet
- Heart - WikipediaDocument215 pagesHeart - WikipediaUviweNo ratings yet
- Rigel Uni Sim Lite DatasheetDocument5 pagesRigel Uni Sim Lite Datasheetmailalexmd.vrn.ruNo ratings yet
- Day 1 Patient's Name: Mr. X Age: 61 Address: Larap, Jose Panganiban, Camarines Norte Date / Time Focus Data, Action, Response Chest PainDocument4 pagesDay 1 Patient's Name: Mr. X Age: 61 Address: Larap, Jose Panganiban, Camarines Norte Date / Time Focus Data, Action, Response Chest PainJulliza Joy PandiNo ratings yet