Download as pdf or txt
You might also like
- Sync2 Specific Competences Tests LRW EOT1Document8 pagesSync2 Specific Competences Tests LRW EOT1mfrancodlrubiaNo ratings yet
- LPC Skills For LawyersDocument226 pagesLPC Skills For LawyersViệt MeoNo ratings yet
- L5 - Control & Adjustment of RespirationDocument24 pagesL5 - Control & Adjustment of Respirationzaini nieNo ratings yet
- Respiratory Diseases Chapter From Nelson Textbook of PediatricsDocument312 pagesRespiratory Diseases Chapter From Nelson Textbook of PediatricsMilan Andrejevic100% (1)
- Alphabet and Teaching Hebrew DecodingDocument11 pagesAlphabet and Teaching Hebrew DecodingLee Robin100% (1)
- Example A Small Signal Analysis of A BJT AmpDocument10 pagesExample A Small Signal Analysis of A BJT AmpFilipe da Silveira100% (1)
- Central Regulation of RespirationDocument54 pagesCentral Regulation of RespirationsamNo ratings yet
- Organization of The Respiratory Control System 2007Document53 pagesOrganization of The Respiratory Control System 2007Vincent VicuñaNo ratings yet
- LIGHT Pulmo Ventilation Sleep Apnea DR ConstantinoDocument6 pagesLIGHT Pulmo Ventilation Sleep Apnea DR ConstantinoMiguel Cuevas DolotNo ratings yet
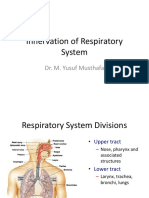
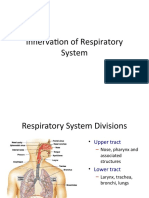
- Innervation of Respiratory SystemDocument21 pagesInnervation of Respiratory SystemYusuf MusthafaNo ratings yet
- (06!03!05) - Lower Brainstem Functions (Compatibility Mode) - 1ppDocument21 pages(06!03!05) - Lower Brainstem Functions (Compatibility Mode) - 1ppjNo ratings yet
- Innervation of Respiratory SystemDocument21 pagesInnervation of Respiratory SystemYusuf MusthafaNo ratings yet
- Regulation of RespirationDocument48 pagesRegulation of Respirationabdullah amirNo ratings yet
- Neural Regulation of RespirationDocument22 pagesNeural Regulation of RespirationDhanush SatheeshNo ratings yet
- RS 1st PartDocument12 pagesRS 1st Parthpcdhp4wkmNo ratings yet
- RegulationofrespirationDocument30 pagesRegulationofrespirationDev SaiNo ratings yet
- Control of Ventilation: Lectures On Respiratory PhysiologyDocument52 pagesControl of Ventilation: Lectures On Respiratory PhysiologyNagib HadianNo ratings yet
- Respiratory Physiology IVDocument52 pagesRespiratory Physiology IVDeea LobonțiuNo ratings yet
- University of LahoreDocument8 pagesUniversity of LahoreAhmad BajwaNo ratings yet
- Respirasi ControlDocument50 pagesRespirasi Controlrinaldy IX9No ratings yet
- Neural Regulation of RespirationDocument56 pagesNeural Regulation of RespirationNishtha GuptaNo ratings yet
- Control of BreathingDocument24 pagesControl of BreathingradicallarryNo ratings yet
- Respiratory System: DR Archna Ghildiyal Associate ProfessorDocument35 pagesRespiratory System: DR Archna Ghildiyal Associate ProfessorFRANCEEN LEANNA KATIGBAKNo ratings yet
- Respiratory System: DR Archna Ghildiyal Associate ProfessorDocument35 pagesRespiratory System: DR Archna Ghildiyal Associate ProfessorFRANCEEN LEANNA KATIGBAKNo ratings yet
- Respiration 3Document23 pagesRespiration 3api-19916399100% (1)
- Respiration - Imp Topics-1Document14 pagesRespiration - Imp Topics-1SHAHSINANo ratings yet
- RespirationDocument10 pagesRespirationADWAIT LALUNo ratings yet
- Egulation of Espiration: Espiratory EntreDocument2 pagesEgulation of Espiration: Espiratory Entrearnav15magicNo ratings yet
- Controlul RespirațieiDocument5 pagesControlul RespirațieiAurelia AlexandraNo ratings yet
- Mbbscbmeph-1 No023525Document40 pagesMbbscbmeph-1 No023525Aritro RoyNo ratings yet
- 4.control of VentilationDocument40 pages4.control of VentilationEbin EbenezerNo ratings yet
- Respiratory ReflexesDocument8 pagesRespiratory ReflexesgokulkrishnayadhavNo ratings yet
- Respiratory Physiology and Anaesthesia: Gary H Mills Bmedsci MBCHB FrcaDocument5 pagesRespiratory Physiology and Anaesthesia: Gary H Mills Bmedsci MBCHB FrcahfjdghjgNo ratings yet
- 1 - Pathophisiology of CoughDocument14 pages1 - Pathophisiology of CoughAqilah MazayaNo ratings yet
- RESPI (PBL1) - Mohamad Arbian Karim - FMUI20Document7 pagesRESPI (PBL1) - Mohamad Arbian Karim - FMUI20Mohamad Arbian KarimNo ratings yet
- Physio Report ShelaDocument20 pagesPhysio Report ShelaSheila HoraNo ratings yet
- Regulation of Respiration: DR Mohamed HassanDocument27 pagesRegulation of Respiration: DR Mohamed HassanSAKARIYE MAXAMEDNo ratings yet
- Regulation of Respiration - 093327Document19 pagesRegulation of Respiration - 093327manahilkhan3103No ratings yet
- Artigo Respirar ImportaDocument17 pagesArtigo Respirar ImportaLuana SteffenNo ratings yet
- Breathing Rhythms and EmotionsDocument11 pagesBreathing Rhythms and EmotionsurweiserNo ratings yet
- Breathing Affects Our Thoughts and EmotionsDocument127 pagesBreathing Affects Our Thoughts and EmotionsarbetaNo ratings yet
- Nocera Lecture36ControlofRespiration-4Document29 pagesNocera Lecture36ControlofRespiration-4Chuk-U MogọNo ratings yet
- Slow Deep BreathingDocument17 pagesSlow Deep BreathingpluigiaNo ratings yet
- Sleepandbreathing: Kelly Newton,, Vipin Malik,, Teofilo Lee-ChiongDocument6 pagesSleepandbreathing: Kelly Newton,, Vipin Malik,, Teofilo Lee-ChiongVijay KumarNo ratings yet
- Regulation of RespirationDocument63 pagesRegulation of RespirationSanya KhoslaNo ratings yet
- Respiratory System - Charts and Graphs 2023Document16 pagesRespiratory System - Charts and Graphs 2023MamathaNo ratings yet
- Neuroanatomy - Answers and ExplanationsDocument6 pagesNeuroanatomy - Answers and ExplanationsshengziyanNo ratings yet
- Pengaturan Sistem RespirasiDocument18 pagesPengaturan Sistem RespirasiMaulidya MagfirahNo ratings yet
- Neural Control of Respiration: A. Medullary SystemsDocument7 pagesNeural Control of Respiration: A. Medullary SystemsKhant Si ThuNo ratings yet
- 25) Regulation of RespirationDocument61 pages25) Regulation of Respirationdr_mksinhaNo ratings yet
- Arduino Uno Based Obstructive Sleep Apnea Detection Using Respiratory SignalDocument5 pagesArduino Uno Based Obstructive Sleep Apnea Detection Using Respiratory SignalbengheniaNo ratings yet
- VentilationDocument6 pagesVentilationLouise FinniganNo ratings yet
- Unit 5.3 Control of RespirationDocument24 pagesUnit 5.3 Control of Respirationjnjjcw68yhNo ratings yet
- Respiration: Control of Ventilation: Learning ObjectivesDocument4 pagesRespiration: Control of Ventilation: Learning Objectiveshuldani-1No ratings yet
- Located Bilaterally in The Medulla Oblongata and Pons of The Brain Stem. Three Major Collections of NeuronsDocument10 pagesLocated Bilaterally in The Medulla Oblongata and Pons of The Brain Stem. Three Major Collections of NeuronsEdzraffel MidtimbangNo ratings yet
- Patterns of RespirationDocument67 pagesPatterns of Respirationsteven hkNo ratings yet
- Neural Regulation of RespirationDocument19 pagesNeural Regulation of RespirationAbeer SallamNo ratings yet
- Control of RespirationDocument33 pagesControl of RespirationJuan Carlos Camacho SuarezNo ratings yet
- Regulation RespirationDocument34 pagesRegulation Respirationkiedd_04100% (2)
- Pi Is 0960982216310557Document2 pagesPi Is 0960982216310557Ridski D. MiruNo ratings yet
- Evelyn Hone College of Applied Arts and Commerce School of Health and Applied Sciences Pharmacy SectionDocument10 pagesEvelyn Hone College of Applied Arts and Commerce School of Health and Applied Sciences Pharmacy Sectionbill chaiwaNo ratings yet
- NURSING CARE PLAN - JayDocument8 pagesNURSING CARE PLAN - JayJaylord VerazonNo ratings yet
- Shams - Lectures P9, P10 and P11 - Acid and BaseDocument42 pagesShams - Lectures P9, P10 and P11 - Acid and BaseUmerNo ratings yet
- OSPE LatestDocument3 pagesOSPE LatestUmerNo ratings yet
- A12. MediastinumDocument29 pagesA12. MediastinumUmerNo ratings yet
- Muscle IIDocument31 pagesMuscle IIUmerNo ratings yet
- Introduction To Physiology 2023 For MoodleDocument17 pagesIntroduction To Physiology 2023 For MoodleUmerNo ratings yet
- B.Lib SyllabusDocument17 pagesB.Lib SyllabussantoshguptaaNo ratings yet
- Sci-Box: Grade 7Document6 pagesSci-Box: Grade 7Trinity MarieNo ratings yet
- Up Portia SororityDocument11 pagesUp Portia Sororitycmv mendozaNo ratings yet
- Mat Rempit EditedDocument21 pagesMat Rempit Editedadle_267% (3)
- Vocab GamesDocument6 pagesVocab Gamesapi-265791946No ratings yet
- SEXTANTDocument5 pagesSEXTANTEmrah GurelNo ratings yet
- Bipolar Disorder ReportDocument6 pagesBipolar Disorder ReportLecah DevarasNo ratings yet
- (Lecture Notes) Brian Osserman - Math 150C - Algebra, Spring 2015 (2015)Document27 pages(Lecture Notes) Brian Osserman - Math 150C - Algebra, Spring 2015 (2015)klinton tvhNo ratings yet
- Building Biblical Theology - Lesson 4 - TransciptDocument28 pagesBuilding Biblical Theology - Lesson 4 - TransciptThird Millennium MinistriesNo ratings yet
- From The Answers To Bar Examination Ques (Dragged)Document11 pagesFrom The Answers To Bar Examination Ques (Dragged)Carla VirtucioNo ratings yet
- OrdinanceDocument5 pagesOrdinanceRudgia Carme CambalonNo ratings yet
- History of Music TherapyDocument4 pagesHistory of Music TherapyJonathan Malimban PrietoNo ratings yet
- Counseling ProjDocument29 pagesCounseling ProjFatema MoiyadiNo ratings yet
- Hope Narrative ReportDocument3 pagesHope Narrative ReportNicole SalaNo ratings yet
- Poetry Terms ReviewDocument3 pagesPoetry Terms ReviewtmaddenNo ratings yet
- Decision TreeDocument12 pagesDecision TreeshrikrishnaNo ratings yet
- Antenna Theory - Short Dipole - Tutorialspoint PDFDocument3 pagesAntenna Theory - Short Dipole - Tutorialspoint PDFSukhada Deshpande.100% (1)
- Interview Questions - AnswersDocument10 pagesInterview Questions - AnswersFatima BibiNo ratings yet
- Accounting Information System of Akij Food & BeverageDocument15 pagesAccounting Information System of Akij Food & BeverageNasim SharifNo ratings yet
- DepartmentationDocument6 pagesDepartmentationAnirudhKodaliNo ratings yet
- Phil Lit Group 3Document15 pagesPhil Lit Group 3rmbayan5No ratings yet
- 겨울왕국 대본Document53 pages겨울왕국 대본김요한No ratings yet
- Grade 8 MusicDocument2 pagesGrade 8 MusicJeneva Rose PerezNo ratings yet
- Proposal Desi Dwi Part 1 After SeminarDocument35 pagesProposal Desi Dwi Part 1 After SeminarNurul OktavianiNo ratings yet
- Strength Weaknesses: Apple IncorporationDocument4 pagesStrength Weaknesses: Apple IncorporationRica Mae InamargaNo ratings yet
- Competence Test A. Choose The Correct AnswerDocument1 pageCompetence Test A. Choose The Correct AnswerRehana Zema hanifaNo ratings yet