Download as pdf or txt
You might also like
- Spinal Cord Lesions 1Document43 pagesSpinal Cord Lesions 1Worthless Boys100% (4)
- Design of Air Conditioning and Ventilation System For A Multi Storey Office BuildingDocument5 pagesDesign of Air Conditioning and Ventilation System For A Multi Storey Office BuildingIppiNo ratings yet
- Folk Violin SongbookDocument19 pagesFolk Violin SongbookTyler Swinn100% (1)
- Spinal Cord TumoursDocument15 pagesSpinal Cord TumoursSakshi NegiNo ratings yet
- CA Spinal CordDocument14 pagesCA Spinal CordMalsawmdawngkimi HmarNo ratings yet
- Intramedullary Spinal Cord TumorsDocument7 pagesIntramedullary Spinal Cord TumorsmutalimNo ratings yet
- Spinal Cord Injury (SCI)Document14 pagesSpinal Cord Injury (SCI)Joanna TaylanNo ratings yet
- Spinal Cord Injury: Presented By: Feliciano, Jenard R. Flores, Arliah Q. Gaspar, Danica VDocument79 pagesSpinal Cord Injury: Presented By: Feliciano, Jenard R. Flores, Arliah Q. Gaspar, Danica VPam RomeroNo ratings yet
- Seminar On Brain TumorDocument26 pagesSeminar On Brain TumorawasthiphothocopyNo ratings yet
- Slkdmsalkdmla Sa NlasDocument12 pagesSlkdmsalkdmla Sa NlasjdjhdNo ratings yet
- Spine and Spinal TraumaDocument47 pagesSpine and Spinal TraumaAde Zulfiah100% (1)
- Structural Disorders of The SpineDocument6 pagesStructural Disorders of The SpineRod Reynon BorceNo ratings yet
- Acute Spinal Cord CompressionDocument13 pagesAcute Spinal Cord CompressionWhoNo ratings yet
- Spinal Cord InjuryDocument13 pagesSpinal Cord Injurypaul_allan17No ratings yet
- Spinal Cord InjuryDocument16 pagesSpinal Cord Injuryjohnlester_jlf100% (2)
- Vertebral Column and DiscDocument5 pagesVertebral Column and Discawais mpNo ratings yet
- Spinal Cord InjuryDocument25 pagesSpinal Cord InjurySolsona Natl HS Maananteng100% (2)
- Tema 1. - Neurotrauma Aproximación Genral y Estrategias de ResuscitaciónDocument17 pagesTema 1. - Neurotrauma Aproximación Genral y Estrategias de ResuscitaciónaniadNo ratings yet
- Spinal cord lesion (Transverse myelitis) د.رشاد عبدالغنيDocument33 pagesSpinal cord lesion (Transverse myelitis) د.رشاد عبدالغنيMohammad BelbahaithNo ratings yet
- Tumors of The Nervous SystemDocument6 pagesTumors of The Nervous SystemRituNo ratings yet
- Meningomyelocele (Spina Bifida) : Bony Neural Arch Not Completely ClosedDocument33 pagesMeningomyelocele (Spina Bifida) : Bony Neural Arch Not Completely Closedlindelle elijahNo ratings yet
- Spine and Spinalcord TraumaDocument21 pagesSpine and Spinalcord TraumaadnanreshunNo ratings yet
- Spinal Meningioma: DR Frank Gaillard View Revision HistoryDocument3 pagesSpinal Meningioma: DR Frank Gaillard View Revision HistoryRia SulistianaNo ratings yet
- CNS PBL 2Document6 pagesCNS PBL 2Hugh JacobsNo ratings yet
- 2 5291964174748882717Document11 pages2 5291964174748882717نشط عقلكNo ratings yet
- Lesion Del Tracto Cortico - Espinal InglesDocument14 pagesLesion Del Tracto Cortico - Espinal InglesCarolina Andrea Daza CharrisNo ratings yet
- SDL 8 Intracranial Space Occupying LesionDocument5 pagesSDL 8 Intracranial Space Occupying LesionJonathan YeohNo ratings yet
- Spinal Cord Tumors: By: Divine Incillo Shiela Marie LaraDocument27 pagesSpinal Cord Tumors: By: Divine Incillo Shiela Marie LaraDivine IncilloNo ratings yet
- Brain Tumor ICP Head and Neck CA TracheostomyDocument11 pagesBrain Tumor ICP Head and Neck CA TracheostomyWincy Faith SalazarNo ratings yet
- Spinal Cord Tumors: Mahmoud Wahdan Benha UniversityDocument61 pagesSpinal Cord Tumors: Mahmoud Wahdan Benha Universitybasmarizk deabsNo ratings yet
- Intradural Spinal Tumors in Adults - Update On Management and OutcomeDocument18 pagesIntradural Spinal Tumors in Adults - Update On Management and OutcomeSuciatije PenelitianNo ratings yet
- Spinal Tumors - A Brief OverviewDocument38 pagesSpinal Tumors - A Brief OverviewRAVIRAJ GHORPADE BELGAUM ADVANCED NEUROSURGERYNo ratings yet
- LP SpinalDocument11 pagesLP SpinalHimaniNo ratings yet
- Magnetic Resonance Imaging of Meningiomas: A Pictorial ReviewDocument10 pagesMagnetic Resonance Imaging of Meningiomas: A Pictorial ReviewKevin EdroNo ratings yet
- Brain & S. C. Tumors, Aneurysm, AVM, Trigeminal Neuralgia, Bell's PalsyDocument15 pagesBrain & S. C. Tumors, Aneurysm, AVM, Trigeminal Neuralgia, Bell's PalsypertinenteNo ratings yet
- Spinal Cord InjuryDocument24 pagesSpinal Cord InjurySteph VistalNo ratings yet
- Spinal Cord TumorDocument3 pagesSpinal Cord TumorRaifian FauziNo ratings yet
- Intramedullary Spinal Cord Tumors: Part I - Epidemiology, Pathophysiology, and DiagnosisDocument11 pagesIntramedullary Spinal Cord Tumors: Part I - Epidemiology, Pathophysiology, and DiagnosiszixzaxoffNo ratings yet
- Spinal Cord InjuryDocument18 pagesSpinal Cord Injuryfaye kimNo ratings yet
- NeoplasiaDocument109 pagesNeoplasiaGEDION ZERIHUNNo ratings yet
- Spinal Injuries: DR Abdelmoniem SaeedDocument44 pagesSpinal Injuries: DR Abdelmoniem SaeedYousef Al-AmeenNo ratings yet
- Definition/Description: Types of SyringomyeliaDocument8 pagesDefinition/Description: Types of SyringomyeliaNurfadiyah YasinNo ratings yet
- Spinal Tumors ArticleDocument5 pagesSpinal Tumors ArticleNouman Safdar AliNo ratings yet
- Spinal Tumors ArticleDocument5 pagesSpinal Tumors ArticleMariaLakhaniNo ratings yet
- Seizure, Headaches, and Right Hemiparesis: R M. B Iii, MDDocument2 pagesSeizure, Headaches, and Right Hemiparesis: R M. B Iii, MDcazecageNo ratings yet
- Legal Med. Report-QueenDocument61 pagesLegal Med. Report-QueenQuinnee VallejosNo ratings yet
- The Radiology Assistant Brain Tumor - Systematic Approach PDFDocument29 pagesThe Radiology Assistant Brain Tumor - Systematic Approach PDFMichael DeanNo ratings yet
- 10 1016@j Amjmed 2018 03 009Document17 pages10 1016@j Amjmed 2018 03 009pedoNo ratings yet
- Brain Tumors: Primary BTDocument5 pagesBrain Tumors: Primary BTMohamed Al-zichrawyNo ratings yet
- Spinal Cord Injury and CompressionDocument10 pagesSpinal Cord Injury and CompressionAdeputhNo ratings yet
- Cerebellopontine Angle TumoursDocument11 pagesCerebellopontine Angle TumoursIsmail Sholeh Bahrun MakkaratteNo ratings yet
- Neck Trauma, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsFrom EverandNeck Trauma, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsNo ratings yet
- Spinal Cord Injury: C M, S - P J - LDocument99 pagesSpinal Cord Injury: C M, S - P J - Lsheel1No ratings yet
- Spinal Tumor: Zelin Sun MD, PH.DDocument28 pagesSpinal Tumor: Zelin Sun MD, PH.DMargaret ThatcherNo ratings yet
- Cervical InjuryDocument9 pagesCervical Injurypmahi8854No ratings yet
- Soul Free - Spinal Cord Injury Knowledge Packet 29. 09. 2013Document6 pagesSoul Free - Spinal Cord Injury Knowledge Packet 29. 09. 2013Maddala NagendrakumarNo ratings yet
- Intramedullary Spinal Cord Tumors: Clinical PresentationDocument15 pagesIntramedullary Spinal Cord Tumors: Clinical Presentationmetasoniko81No ratings yet
- Diagnosis and Treatment of Brain TumorDocument9 pagesDiagnosis and Treatment of Brain TumorCharan TejaNo ratings yet
- Spinal Cord Injury - CompleteDocument88 pagesSpinal Cord Injury - CompleteJen Passilan100% (10)
- 1spinal Cord InjuryDocument8 pages1spinal Cord Injurysunny_jr_No ratings yet
- Transverse Myelitis, A Simple Guide To The Condition, Treatment And Related DiseasesFrom EverandTransverse Myelitis, A Simple Guide To The Condition, Treatment And Related DiseasesRating: 5 out of 5 stars5/5 (1)
- Carpal Tunnel Syndrome, A Simple Guide To The Condition, Treatment And Related ConditionsFrom EverandCarpal Tunnel Syndrome, A Simple Guide To The Condition, Treatment And Related ConditionsRating: 5 out of 5 stars5/5 (1)
- Crane Overhaul ProcedureDocument8 pagesCrane Overhaul ProcedureHưng ĐỗNo ratings yet
- MonotropismQuestionnaire 230510Document5 pagesMonotropismQuestionnaire 230510Javiera AlarconNo ratings yet
- Full Development of Annex A Exercise-J CardenasDocument17 pagesFull Development of Annex A Exercise-J CardenasBruno SamosNo ratings yet
- Instruction Manual: High-Output, Temperature Controlled Soldering StationDocument28 pagesInstruction Manual: High-Output, Temperature Controlled Soldering Stationalexgreen121No ratings yet
- License Exceptions Part 740 - Page 1: 740.1 IntroductionDocument82 pagesLicense Exceptions Part 740 - Page 1: 740.1 Introductiondali layouniNo ratings yet
- Tryptophan 2 PDFDocument9 pagesTryptophan 2 PDFLim Xiu XianNo ratings yet
- RecursionDocument9 pagesRecursionMada BaskoroNo ratings yet
- 2019 Bookmatter AgronomicCropsDocument17 pages2019 Bookmatter AgronomicCropsMunimNo ratings yet
- Iw Tec 200 01Document548 pagesIw Tec 200 01GuilhermeNo ratings yet
- Module 17 TAI - TC.MTO Basic Knowledge Examination Summary DataDocument27 pagesModule 17 TAI - TC.MTO Basic Knowledge Examination Summary DataChatchai PrasertsukNo ratings yet
- AHN Eafit Sarmiento 2011 Llanos Petroleum GeologyDocument177 pagesAHN Eafit Sarmiento 2011 Llanos Petroleum Geology2032086No ratings yet
- Zipatile ManualDocument16 pagesZipatile ManualdacrysNo ratings yet
- Astm Specifications For Concrete Masonry Units: TEK 1-1FDocument4 pagesAstm Specifications For Concrete Masonry Units: TEK 1-1FEric HernándezNo ratings yet
- Toxicon: Tamara Sajevic, Adrijana Leonardi, Igor Kri ZajDocument19 pagesToxicon: Tamara Sajevic, Adrijana Leonardi, Igor Kri Zajaulia rahmahNo ratings yet
- Howlett Paper 09182013Document6 pagesHowlett Paper 09182013FutantxxyzNo ratings yet
- William Stallings Computer Organization and Architecture 9 EditionDocument28 pagesWilliam Stallings Computer Organization and Architecture 9 EditionAnggi Riza Amirullah SidhartaNo ratings yet
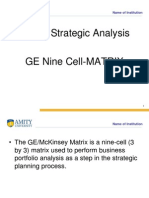
- GE - Nine CellDocument12 pagesGE - Nine CellNikita SangalNo ratings yet
- Dwnload Full Icd 10 CM Pcs Coding Theory and Practice 2016 Edition 1st Edition Lovaasen Test Bank PDFDocument33 pagesDwnload Full Icd 10 CM Pcs Coding Theory and Practice 2016 Edition 1st Edition Lovaasen Test Bank PDFjacobgrahamlet100% (13)
- Periodontal Ligament-SummerDocument24 pagesPeriodontal Ligament-Summerapi-3775747100% (1)
- Inquiry-Based Lesson Plan - HypothesesDocument3 pagesInquiry-Based Lesson Plan - Hypothesesapi-532939717No ratings yet
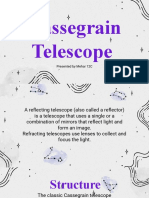
- Cassegrain Telescope: Presented by Mehar 12CDocument10 pagesCassegrain Telescope: Presented by Mehar 12CMehar FathimaNo ratings yet
- Green Light HPS Laser Operator ManualDocument81 pagesGreen Light HPS Laser Operator ManualPhillip V Mitchell0% (1)
- LevellingDocument11 pagesLevellingetikaf50% (2)
- The 73rd Constitutional Amendment ActDocument26 pagesThe 73rd Constitutional Amendment ActYasser ArfatNo ratings yet
- Data SheetDocument48 pagesData SheetLost HumeraNo ratings yet
- AAA EDR Container DescriptionDocument12 pagesAAA EDR Container DescriptionmadhumohanNo ratings yet
- Allison Taylor Dissertation Heinrich SchliemannDocument6 pagesAllison Taylor Dissertation Heinrich SchliemannPaperWritingServiceSuperiorpapersSpringfield100% (1)
- Deyu Cai: General Notes and SpecificationDocument1 pageDeyu Cai: General Notes and SpecificationSKYLERNo ratings yet