
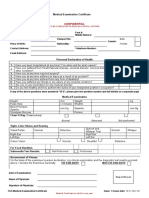
Medical Check Up Form
Medical Check Up Form
You might also like
- Pre Employment Medical Test FormDocument1 pagePre Employment Medical Test FormSreedhar Raja100% (16)
- Pre-Employment Medical Examination FormDocument2 pagesPre-Employment Medical Examination FormAnandababu70% (10)
- New Teacher Induction ProgramDocument6 pagesNew Teacher Induction Programapi-458881694No ratings yet
- Laboratory Request FormDocument1 pageLaboratory Request FormEric Nagum100% (2)
- Pre Employment Medical Examination Form - RS - pt.FIDocument3 pagesPre Employment Medical Examination Form - RS - pt.FINooB GAMING100% (1)
- Fuzail Ayaz Gamca ReportDocument1 pageFuzail Ayaz Gamca ReportFuzail AyazNo ratings yet
- GCC Medical FormDocument1 pageGCC Medical Formதஞ்சை செல்வம்100% (2)
- Scientific Principles of Strength TrainingDocument38 pagesScientific Principles of Strength Trainingarkko5585% (13)
- Nationwide Health Systems Baguio, Inc: Please Fill Up Dotted Boxed Area OnlyDocument1 pageNationwide Health Systems Baguio, Inc: Please Fill Up Dotted Boxed Area OnlyNorma Arquillo100% (1)
- Medical Examination Certificate: ConfidentialDocument2 pagesMedical Examination Certificate: ConfidentialVioleta100% (1)
- Medical Report 1Document1 pageMedical Report 1Ravi Nagar 47No ratings yet
- Vision Report SchaefflerDocument1 pageVision Report SchaefflerMarketingNo ratings yet
- Bản sao của Form thực hành nhập môn KXNK 2Document2 pagesBản sao của Form thực hành nhập môn KXNK 2YouTube GoogleNo ratings yet
- Nhsbi FormDocument1 pageNhsbi FormBudong BernalNo ratings yet
- Annexure-3 (Medical Certificate)Document1 pageAnnexure-3 (Medical Certificate)Kirti SainiNo ratings yet
- Nationwide Health Systems Baguio, Inc: Please Fill Up Dotted Boxed Area OnlyDocument1 pageNationwide Health Systems Baguio, Inc: Please Fill Up Dotted Boxed Area OnlyLennix ValenciaNo ratings yet
- Lto SPDocument3 pagesLto SPKaran ChoNo ratings yet
- Job Hazard Analysis: Iwp Project - Barka PROJ. 135Document12 pagesJob Hazard Analysis: Iwp Project - Barka PROJ. 135Satheesh PurushothamanNo ratings yet
- Cinical Note Sheet: Prsenting ComplaintsDocument2 pagesCinical Note Sheet: Prsenting ComplaintsDhananjay SainiNo ratings yet
- Job Hazard Analysis: JHA By: DateDocument12 pagesJob Hazard Analysis: JHA By: DateSatheesh PurushothamanNo ratings yet
- Nhsbi FormDocument1 pageNhsbi FormClark Jayden JacobNo ratings yet
- Medical Checkup Requirement For Permission Work Visa in Kingdom of BahrainDocument1 pageMedical Checkup Requirement For Permission Work Visa in Kingdom of BahrainAngle_BahNo ratings yet
- Opd Final PDFDocument1 pageOpd Final PDFmadhyabindu municipal hospitalNo ratings yet
- Nationwide Health Systems Baguio, Inc: DateDocument1 pageNationwide Health Systems Baguio, Inc: Datei KordiNo ratings yet
- AMRDocument1 pageAMR87j7qmn5nvNo ratings yet
- IPAMS Healthcare and Medical Services Evaluation FormDocument2 pagesIPAMS Healthcare and Medical Services Evaluation FormManases VelasquezNo ratings yet
- Our Lady of Perpetual Help: I. Patient'S Personal InformationDocument10 pagesOur Lady of Perpetual Help: I. Patient'S Personal InformationOkram OrlinaNo ratings yet
- Medical Health Check Up FormDocument1 pageMedical Health Check Up FormR Sahadeo ReddyNo ratings yet
- Annex (1) Health Check-Up Form: Detailed Candidate ReportDocument6 pagesAnnex (1) Health Check-Up Form: Detailed Candidate ReportMukesh MistriNo ratings yet
- Medical FormDocument1 pageMedical Formmspplwith bclNo ratings yet
- Bill Cum ReceiptMr. PAT - 000042Document1 pageBill Cum ReceiptMr. PAT - 000042Sidharth WalavalkarNo ratings yet
- Case SheetDocument9 pagesCase SheetmoghkadayanallurNo ratings yet
- Case Sheet L3Document22 pagesCase Sheet L3Gulfeshan ArshiNo ratings yet
- Medical Surveillance GuidelineDocument21 pagesMedical Surveillance GuidelineIdham BaharudinNo ratings yet
- Health FitnessDocument3 pagesHealth FitnessNo oneNo ratings yet
- Medical CertificateDocument1 pageMedical CertificateManvi DuttNo ratings yet
- Ram Neupane Opd TicketDocument1 pageRam Neupane Opd Ticketmadhyabindu municipal hospitalNo ratings yet
- CHO Medical CertificateDocument1 pageCHO Medical Certificategebarita24No ratings yet
- Sample Form - New Pre-Employment - MEDEX 001Document3 pagesSample Form - New Pre-Employment - MEDEX 001Helmi C MahadyNo ratings yet
- MedSurg SBARDocument2 pagesMedSurg SBARduaalipa18No ratings yet
- F7.6 Seafarers Medical Examination-CertificateDocument7 pagesF7.6 Seafarers Medical Examination-CertificateHerbert Maganga100% (1)
- New Health Screening Medical FormDocument4 pagesNew Health Screening Medical Formsalmankhan.484875No ratings yet
- Rules and RegulationsDocument6 pagesRules and RegulationsMukesh MistriNo ratings yet
- Non GAMCA Medical Check Up FormDocument1 pageNon GAMCA Medical Check Up FormNurman Hidayat100% (1)
- Piedmont Authorization Form FIT TestDocument1 pagePiedmont Authorization Form FIT Testodurden02No ratings yet
- Format For Medical CertificateDocument1 pageFormat For Medical Certificatecittu RajputNo ratings yet
- Response To Referral N503846 06 JanDocument4 pagesResponse To Referral N503846 06 Janpratapreddy1258No ratings yet
- Medical Certificate: KEDLU6506206191036Document1 pageMedical Certificate: KEDLU6506206191036Shier LynNo ratings yet
- General Physical Exam FormDocument4 pagesGeneral Physical Exam FormNay LinNo ratings yet
- Format No. 1-2019-PSS-01 Rev.1Document1 pageFormat No. 1-2019-PSS-01 Rev.1nithinNo ratings yet
- Case Investigation Form - Acute Flaccid ParalysisDocument2 pagesCase Investigation Form - Acute Flaccid Paralysisclaverialc10No ratings yet
- PFIZER 5 17 All in 1 FormDocument3 pagesPFIZER 5 17 All in 1 Formrenz jNo ratings yet
- Nhsbi Form To Deepen UnderstandingDocument2 pagesNhsbi Form To Deepen UnderstandingRoselle ManuelNo ratings yet
- HM Medical Checkups at Project Sites Medical CampsDocument2 pagesHM Medical Checkups at Project Sites Medical Campsraj kumariNo ratings yet
- Medical Form For Countries That Did Not Ratified MLCDocument1 pageMedical Form For Countries That Did Not Ratified MLCBranimira Dukic BaracNo ratings yet
- Medical Report FormDocument2 pagesMedical Report FormmakinchNo ratings yet
- Airport Security ForcesDocument1 pageAirport Security Forcesabcdbcd098No ratings yet
- GDOH-LAB-SAF-305 Stool Analysis FormDocument1 pageGDOH-LAB-SAF-305 Stool Analysis FormdrabdulrabbNo ratings yet
- Ape Blank FormDocument1 pageApe Blank FormArlene Bermudez PascualNo ratings yet
- One Step Med: General Medical Information Record Keeping ManualFrom EverandOne Step Med: General Medical Information Record Keeping ManualNo ratings yet
- Govt Polytechnic College UjjainDocument15 pagesGovt Polytechnic College UjjainRavi Nagar 47No ratings yet
- Ee 5 Sem Power Electronics and Application 6241 F 2017Document4 pagesEe 5 Sem Power Electronics and Application 6241 F 2017Ravi Nagar 47No ratings yet
- Hours T: I) Ii) FR - A) Costirg. B) C) Estimate. D) SystemsDocument4 pagesHours T: I) Ii) FR - A) Costirg. B) C) Estimate. D) SystemsRavi Nagar 47No ratings yet
- Minor Project 5th SemDocument19 pagesMinor Project 5th SemRavi Nagar 47No ratings yet
- Resume: Ravi NagarDocument2 pagesResume: Ravi NagarRavi Nagar 47No ratings yet
- Vishwavidyalaya, BHOPAL: ElecdicalDocument9 pagesVishwavidyalaya, BHOPAL: ElecdicalRavi Nagar 47No ratings yet
- Su Jeut: RoladDocument5 pagesSu Jeut: RoladRavi Nagar 47No ratings yet
- Ele ProjDocument34 pagesEle ProjRavi Nagar 47No ratings yet
- 19030e01047 6842 PDFDocument7 pages19030e01047 6842 PDFRavi Nagar 47No ratings yet
- Ravi NagarDocument5 pagesRavi NagarRavi Nagar 47No ratings yet
- Psop Assignment Dec 16, 2021Document8 pagesPsop Assignment Dec 16, 2021Ravi Nagar 47No ratings yet
- G63Oeoiout 25 - 02J2O2: Arebe MebieDocument4 pagesG63Oeoiout 25 - 02J2O2: Arebe MebieRavi Nagar 47No ratings yet
- 19030e01047 6841 PDFDocument4 pages19030e01047 6841 PDFRavi Nagar 47No ratings yet
- Obe Curriculum For The Course: RGPV (Diploma Wing) BhopalDocument6 pagesObe Curriculum For The Course: RGPV (Diploma Wing) BhopalRavi Nagar 47No ratings yet
- Obe Curriculum For The Course: RGPV (Diploma Wing) BhopalDocument6 pagesObe Curriculum For The Course: RGPV (Diploma Wing) BhopalRavi Nagar 47No ratings yet
- Obe Curriculum For The Course: RGPV (Diploma Wing) BhopalDocument6 pagesObe Curriculum For The Course: RGPV (Diploma Wing) BhopalRavi Nagar 47No ratings yet
- Jurnal 1 Risk Factors Female Breast CancerDocument11 pagesJurnal 1 Risk Factors Female Breast CanceriprastiNo ratings yet
- FINAL High Alert Checklist UpdatedDocument5 pagesFINAL High Alert Checklist UpdatedCita BudiartiNo ratings yet
- Eugene Emergency Physicians Community LetterDocument4 pagesEugene Emergency Physicians Community LetterSinclair Broadcast Group - Eugene100% (2)
- The Brazilian Hip and Groin Outcome Score (HAGOS-Br)Document9 pagesThe Brazilian Hip and Groin Outcome Score (HAGOS-Br)Clarice CarvalhoNo ratings yet
- TACFIT - Kettlebell Spetsnaz 101Document10 pagesTACFIT - Kettlebell Spetsnaz 101Fabrizio Mosca100% (1)
- Mechanical Load Exerted by PET-G Aligners During Mesial and Distal Derotation of A Mandibular CanineDocument9 pagesMechanical Load Exerted by PET-G Aligners During Mesial and Distal Derotation of A Mandibular CanineDavid F. MuñozNo ratings yet
- Icmm Sustainable Development FrameworkDocument5 pagesIcmm Sustainable Development Frameworkfaqih rasyidNo ratings yet
- Curriculum Vitae Eric Kinnosuke Martins Ueda Phar.D., MSC, PHDDocument3 pagesCurriculum Vitae Eric Kinnosuke Martins Ueda Phar.D., MSC, PHDEric Ueda100% (1)
- Constitution of ZimbabweDocument139 pagesConstitution of ZimbabweIdah GoverehNo ratings yet
- Exit InterviewDocument3 pagesExit Interviewgunawan WNo ratings yet
- MRCP (UK) PACES 22-2 Feedback Report For The WebsiteDocument6 pagesMRCP (UK) PACES 22-2 Feedback Report For The WebsiteSmallsNo ratings yet
- Sindi Artika (ENGLISH FOR NURSE 3. Reading)Document3 pagesSindi Artika (ENGLISH FOR NURSE 3. Reading)Artika SindiNo ratings yet
- Mental HelthDocument19 pagesMental Helthjayvee dacubaNo ratings yet
- Epidemiology Course OutlineDocument6 pagesEpidemiology Course OutlineFYMNo ratings yet
- Modul Pembahasn YosiDocument2 pagesModul Pembahasn YosiAnisa Nur AfifahNo ratings yet
- BCCH Diabetic Ketoacidosis Protocol Toolkit: Endocrinology & Diabetes UnitDocument16 pagesBCCH Diabetic Ketoacidosis Protocol Toolkit: Endocrinology & Diabetes UnitaseelNo ratings yet
- Motif Pemerintah Australia Melalui Program Hcpi Terhadap Kaum Gay Dan Waria Di Bali Tahun 2009Document12 pagesMotif Pemerintah Australia Melalui Program Hcpi Terhadap Kaum Gay Dan Waria Di Bali Tahun 2009Rizki NurulhadiNo ratings yet
- Tien Cheu 2021Document11 pagesTien Cheu 2021Ismael Cervantes ChavezNo ratings yet
- Midterm Test Level 4 (50 Points)Document4 pagesMidterm Test Level 4 (50 Points)Valeria Alonso LopezNo ratings yet
- Double ComparisonDocument3 pagesDouble ComparisonMai PhuongNo ratings yet
- 11 Effects of Sleep Deprivation On Your BodyDocument1 page11 Effects of Sleep Deprivation On Your Bodydayna mooreNo ratings yet
- A Descriptive Study To Assess The Level of Knowledge Regarding Burnout Syndromme Among The Staff NursesDocument8 pagesA Descriptive Study To Assess The Level of Knowledge Regarding Burnout Syndromme Among The Staff NursesIJRASETPublicationsNo ratings yet
- Jurnal InternasionalDocument17 pagesJurnal InternasionalindahNo ratings yet
- Buy Adderall 5 MG Online in USDocument11 pagesBuy Adderall 5 MG Online in USmyadderallNo ratings yet
- Assignment 2, Rafia Tanveer, L-21274, Business LawDocument4 pagesAssignment 2, Rafia Tanveer, L-21274, Business LawFaisal NaqviNo ratings yet
- Maa Atta Tho SarasamDocument3 pagesMaa Atta Tho SarasamVidya Sagar NuguriNo ratings yet
- Paper Presentation PDFDocument18 pagesPaper Presentation PDFramneekNo ratings yet
- Module II On PFA: Calming Down and Managing One's Emotions and Thoughts (DAY 2)Document2 pagesModule II On PFA: Calming Down and Managing One's Emotions and Thoughts (DAY 2)Jenny RoseNo ratings yet





































































































Download as pdf or txt
You might also like
- Pre Employment Medical Test FormDocument1 pagePre Employment Medical Test FormSreedhar Raja100% (16)
- Pre-Employment Medical Examination FormDocument2 pagesPre-Employment Medical Examination FormAnandababu70% (10)
- New Teacher Induction ProgramDocument6 pagesNew Teacher Induction Programapi-458881694No ratings yet
- Laboratory Request FormDocument1 pageLaboratory Request FormEric Nagum100% (2)
- Pre Employment Medical Examination Form - RS - pt.FIDocument3 pagesPre Employment Medical Examination Form - RS - pt.FINooB GAMING100% (1)
- Fuzail Ayaz Gamca ReportDocument1 pageFuzail Ayaz Gamca ReportFuzail AyazNo ratings yet
- GCC Medical FormDocument1 pageGCC Medical Formதஞ்சை செல்வம்100% (2)
- Scientific Principles of Strength TrainingDocument38 pagesScientific Principles of Strength Trainingarkko5585% (13)
- Nationwide Health Systems Baguio, Inc: Please Fill Up Dotted Boxed Area OnlyDocument1 pageNationwide Health Systems Baguio, Inc: Please Fill Up Dotted Boxed Area OnlyNorma Arquillo100% (1)
- Medical Examination Certificate: ConfidentialDocument2 pagesMedical Examination Certificate: ConfidentialVioleta100% (1)
- Medical Report 1Document1 pageMedical Report 1Ravi Nagar 47No ratings yet
- Vision Report SchaefflerDocument1 pageVision Report SchaefflerMarketingNo ratings yet
- Bản sao của Form thực hành nhập môn KXNK 2Document2 pagesBản sao của Form thực hành nhập môn KXNK 2YouTube GoogleNo ratings yet
- Nhsbi FormDocument1 pageNhsbi FormBudong BernalNo ratings yet
- Annexure-3 (Medical Certificate)Document1 pageAnnexure-3 (Medical Certificate)Kirti SainiNo ratings yet
- Nationwide Health Systems Baguio, Inc: Please Fill Up Dotted Boxed Area OnlyDocument1 pageNationwide Health Systems Baguio, Inc: Please Fill Up Dotted Boxed Area OnlyLennix ValenciaNo ratings yet
- Lto SPDocument3 pagesLto SPKaran ChoNo ratings yet
- Job Hazard Analysis: Iwp Project - Barka PROJ. 135Document12 pagesJob Hazard Analysis: Iwp Project - Barka PROJ. 135Satheesh PurushothamanNo ratings yet
- Cinical Note Sheet: Prsenting ComplaintsDocument2 pagesCinical Note Sheet: Prsenting ComplaintsDhananjay SainiNo ratings yet
- Job Hazard Analysis: JHA By: DateDocument12 pagesJob Hazard Analysis: JHA By: DateSatheesh PurushothamanNo ratings yet
- Nhsbi FormDocument1 pageNhsbi FormClark Jayden JacobNo ratings yet
- Medical Checkup Requirement For Permission Work Visa in Kingdom of BahrainDocument1 pageMedical Checkup Requirement For Permission Work Visa in Kingdom of BahrainAngle_BahNo ratings yet
- Opd Final PDFDocument1 pageOpd Final PDFmadhyabindu municipal hospitalNo ratings yet
- Nationwide Health Systems Baguio, Inc: DateDocument1 pageNationwide Health Systems Baguio, Inc: Datei KordiNo ratings yet
- AMRDocument1 pageAMR87j7qmn5nvNo ratings yet
- IPAMS Healthcare and Medical Services Evaluation FormDocument2 pagesIPAMS Healthcare and Medical Services Evaluation FormManases VelasquezNo ratings yet
- Our Lady of Perpetual Help: I. Patient'S Personal InformationDocument10 pagesOur Lady of Perpetual Help: I. Patient'S Personal InformationOkram OrlinaNo ratings yet
- Medical Health Check Up FormDocument1 pageMedical Health Check Up FormR Sahadeo ReddyNo ratings yet
- Annex (1) Health Check-Up Form: Detailed Candidate ReportDocument6 pagesAnnex (1) Health Check-Up Form: Detailed Candidate ReportMukesh MistriNo ratings yet
- Medical FormDocument1 pageMedical Formmspplwith bclNo ratings yet
- Bill Cum ReceiptMr. PAT - 000042Document1 pageBill Cum ReceiptMr. PAT - 000042Sidharth WalavalkarNo ratings yet
- Case SheetDocument9 pagesCase SheetmoghkadayanallurNo ratings yet
- Case Sheet L3Document22 pagesCase Sheet L3Gulfeshan ArshiNo ratings yet
- Medical Surveillance GuidelineDocument21 pagesMedical Surveillance GuidelineIdham BaharudinNo ratings yet
- Health FitnessDocument3 pagesHealth FitnessNo oneNo ratings yet
- Medical CertificateDocument1 pageMedical CertificateManvi DuttNo ratings yet
- Ram Neupane Opd TicketDocument1 pageRam Neupane Opd Ticketmadhyabindu municipal hospitalNo ratings yet
- CHO Medical CertificateDocument1 pageCHO Medical Certificategebarita24No ratings yet
- Sample Form - New Pre-Employment - MEDEX 001Document3 pagesSample Form - New Pre-Employment - MEDEX 001Helmi C MahadyNo ratings yet
- MedSurg SBARDocument2 pagesMedSurg SBARduaalipa18No ratings yet
- F7.6 Seafarers Medical Examination-CertificateDocument7 pagesF7.6 Seafarers Medical Examination-CertificateHerbert Maganga100% (1)
- New Health Screening Medical FormDocument4 pagesNew Health Screening Medical Formsalmankhan.484875No ratings yet
- Rules and RegulationsDocument6 pagesRules and RegulationsMukesh MistriNo ratings yet
- Non GAMCA Medical Check Up FormDocument1 pageNon GAMCA Medical Check Up FormNurman Hidayat100% (1)
- Piedmont Authorization Form FIT TestDocument1 pagePiedmont Authorization Form FIT Testodurden02No ratings yet
- Format For Medical CertificateDocument1 pageFormat For Medical Certificatecittu RajputNo ratings yet
- Response To Referral N503846 06 JanDocument4 pagesResponse To Referral N503846 06 Janpratapreddy1258No ratings yet
- Medical Certificate: KEDLU6506206191036Document1 pageMedical Certificate: KEDLU6506206191036Shier LynNo ratings yet
- General Physical Exam FormDocument4 pagesGeneral Physical Exam FormNay LinNo ratings yet
- Format No. 1-2019-PSS-01 Rev.1Document1 pageFormat No. 1-2019-PSS-01 Rev.1nithinNo ratings yet
- Case Investigation Form - Acute Flaccid ParalysisDocument2 pagesCase Investigation Form - Acute Flaccid Paralysisclaverialc10No ratings yet
- PFIZER 5 17 All in 1 FormDocument3 pagesPFIZER 5 17 All in 1 Formrenz jNo ratings yet
- Nhsbi Form To Deepen UnderstandingDocument2 pagesNhsbi Form To Deepen UnderstandingRoselle ManuelNo ratings yet
- HM Medical Checkups at Project Sites Medical CampsDocument2 pagesHM Medical Checkups at Project Sites Medical Campsraj kumariNo ratings yet
- Medical Form For Countries That Did Not Ratified MLCDocument1 pageMedical Form For Countries That Did Not Ratified MLCBranimira Dukic BaracNo ratings yet
- Medical Report FormDocument2 pagesMedical Report FormmakinchNo ratings yet
- Airport Security ForcesDocument1 pageAirport Security Forcesabcdbcd098No ratings yet
- GDOH-LAB-SAF-305 Stool Analysis FormDocument1 pageGDOH-LAB-SAF-305 Stool Analysis FormdrabdulrabbNo ratings yet
- Ape Blank FormDocument1 pageApe Blank FormArlene Bermudez PascualNo ratings yet
- One Step Med: General Medical Information Record Keeping ManualFrom EverandOne Step Med: General Medical Information Record Keeping ManualNo ratings yet
- Govt Polytechnic College UjjainDocument15 pagesGovt Polytechnic College UjjainRavi Nagar 47No ratings yet
- Ee 5 Sem Power Electronics and Application 6241 F 2017Document4 pagesEe 5 Sem Power Electronics and Application 6241 F 2017Ravi Nagar 47No ratings yet
- Hours T: I) Ii) FR - A) Costirg. B) C) Estimate. D) SystemsDocument4 pagesHours T: I) Ii) FR - A) Costirg. B) C) Estimate. D) SystemsRavi Nagar 47No ratings yet
- Minor Project 5th SemDocument19 pagesMinor Project 5th SemRavi Nagar 47No ratings yet
- Resume: Ravi NagarDocument2 pagesResume: Ravi NagarRavi Nagar 47No ratings yet
- Vishwavidyalaya, BHOPAL: ElecdicalDocument9 pagesVishwavidyalaya, BHOPAL: ElecdicalRavi Nagar 47No ratings yet
- Su Jeut: RoladDocument5 pagesSu Jeut: RoladRavi Nagar 47No ratings yet
- Ele ProjDocument34 pagesEle ProjRavi Nagar 47No ratings yet
- 19030e01047 6842 PDFDocument7 pages19030e01047 6842 PDFRavi Nagar 47No ratings yet
- Ravi NagarDocument5 pagesRavi NagarRavi Nagar 47No ratings yet
- Psop Assignment Dec 16, 2021Document8 pagesPsop Assignment Dec 16, 2021Ravi Nagar 47No ratings yet
- G63Oeoiout 25 - 02J2O2: Arebe MebieDocument4 pagesG63Oeoiout 25 - 02J2O2: Arebe MebieRavi Nagar 47No ratings yet
- 19030e01047 6841 PDFDocument4 pages19030e01047 6841 PDFRavi Nagar 47No ratings yet
- Obe Curriculum For The Course: RGPV (Diploma Wing) BhopalDocument6 pagesObe Curriculum For The Course: RGPV (Diploma Wing) BhopalRavi Nagar 47No ratings yet
- Obe Curriculum For The Course: RGPV (Diploma Wing) BhopalDocument6 pagesObe Curriculum For The Course: RGPV (Diploma Wing) BhopalRavi Nagar 47No ratings yet
- Obe Curriculum For The Course: RGPV (Diploma Wing) BhopalDocument6 pagesObe Curriculum For The Course: RGPV (Diploma Wing) BhopalRavi Nagar 47No ratings yet
- Jurnal 1 Risk Factors Female Breast CancerDocument11 pagesJurnal 1 Risk Factors Female Breast CanceriprastiNo ratings yet
- FINAL High Alert Checklist UpdatedDocument5 pagesFINAL High Alert Checklist UpdatedCita BudiartiNo ratings yet
- Eugene Emergency Physicians Community LetterDocument4 pagesEugene Emergency Physicians Community LetterSinclair Broadcast Group - Eugene100% (2)
- The Brazilian Hip and Groin Outcome Score (HAGOS-Br)Document9 pagesThe Brazilian Hip and Groin Outcome Score (HAGOS-Br)Clarice CarvalhoNo ratings yet
- TACFIT - Kettlebell Spetsnaz 101Document10 pagesTACFIT - Kettlebell Spetsnaz 101Fabrizio Mosca100% (1)
- Mechanical Load Exerted by PET-G Aligners During Mesial and Distal Derotation of A Mandibular CanineDocument9 pagesMechanical Load Exerted by PET-G Aligners During Mesial and Distal Derotation of A Mandibular CanineDavid F. MuñozNo ratings yet
- Icmm Sustainable Development FrameworkDocument5 pagesIcmm Sustainable Development Frameworkfaqih rasyidNo ratings yet
- Curriculum Vitae Eric Kinnosuke Martins Ueda Phar.D., MSC, PHDDocument3 pagesCurriculum Vitae Eric Kinnosuke Martins Ueda Phar.D., MSC, PHDEric Ueda100% (1)
- Constitution of ZimbabweDocument139 pagesConstitution of ZimbabweIdah GoverehNo ratings yet
- Exit InterviewDocument3 pagesExit Interviewgunawan WNo ratings yet
- MRCP (UK) PACES 22-2 Feedback Report For The WebsiteDocument6 pagesMRCP (UK) PACES 22-2 Feedback Report For The WebsiteSmallsNo ratings yet
- Sindi Artika (ENGLISH FOR NURSE 3. Reading)Document3 pagesSindi Artika (ENGLISH FOR NURSE 3. Reading)Artika SindiNo ratings yet
- Mental HelthDocument19 pagesMental Helthjayvee dacubaNo ratings yet
- Epidemiology Course OutlineDocument6 pagesEpidemiology Course OutlineFYMNo ratings yet
- Modul Pembahasn YosiDocument2 pagesModul Pembahasn YosiAnisa Nur AfifahNo ratings yet
- BCCH Diabetic Ketoacidosis Protocol Toolkit: Endocrinology & Diabetes UnitDocument16 pagesBCCH Diabetic Ketoacidosis Protocol Toolkit: Endocrinology & Diabetes UnitaseelNo ratings yet
- Motif Pemerintah Australia Melalui Program Hcpi Terhadap Kaum Gay Dan Waria Di Bali Tahun 2009Document12 pagesMotif Pemerintah Australia Melalui Program Hcpi Terhadap Kaum Gay Dan Waria Di Bali Tahun 2009Rizki NurulhadiNo ratings yet
- Tien Cheu 2021Document11 pagesTien Cheu 2021Ismael Cervantes ChavezNo ratings yet
- Midterm Test Level 4 (50 Points)Document4 pagesMidterm Test Level 4 (50 Points)Valeria Alonso LopezNo ratings yet
- Double ComparisonDocument3 pagesDouble ComparisonMai PhuongNo ratings yet
- 11 Effects of Sleep Deprivation On Your BodyDocument1 page11 Effects of Sleep Deprivation On Your Bodydayna mooreNo ratings yet
- A Descriptive Study To Assess The Level of Knowledge Regarding Burnout Syndromme Among The Staff NursesDocument8 pagesA Descriptive Study To Assess The Level of Knowledge Regarding Burnout Syndromme Among The Staff NursesIJRASETPublicationsNo ratings yet
- Jurnal InternasionalDocument17 pagesJurnal InternasionalindahNo ratings yet
- Buy Adderall 5 MG Online in USDocument11 pagesBuy Adderall 5 MG Online in USmyadderallNo ratings yet
- Assignment 2, Rafia Tanveer, L-21274, Business LawDocument4 pagesAssignment 2, Rafia Tanveer, L-21274, Business LawFaisal NaqviNo ratings yet
- Maa Atta Tho SarasamDocument3 pagesMaa Atta Tho SarasamVidya Sagar NuguriNo ratings yet
- Paper Presentation PDFDocument18 pagesPaper Presentation PDFramneekNo ratings yet
- Module II On PFA: Calming Down and Managing One's Emotions and Thoughts (DAY 2)Document2 pagesModule II On PFA: Calming Down and Managing One's Emotions and Thoughts (DAY 2)Jenny RoseNo ratings yet