Download as docx, pdf, or txt
You might also like
- Practice Bulletin: Management of Preterm LaborDocument10 pagesPractice Bulletin: Management of Preterm LaborXimena OrtegaNo ratings yet
- IOSA ManualDocument702 pagesIOSA ManualManisha YuukiNo ratings yet
- Partus Immaturus, Prematurus, Serotinus.: Dr. Fery Kusnadi, SpogDocument60 pagesPartus Immaturus, Prematurus, Serotinus.: Dr. Fery Kusnadi, SpogArtika MayandaNo ratings yet
- Criminal Law Essay FinalDocument15 pagesCriminal Law Essay FinalAlexander PletschNo ratings yet
- Pre and Post PregnancyDocument23 pagesPre and Post PregnancyJitendra ChaudharyNo ratings yet
- Tocolytics (Also Called Anti-Contraction Medications or Labor Represents) AreDocument2 pagesTocolytics (Also Called Anti-Contraction Medications or Labor Represents) AreEric RothNo ratings yet
- Early Pregnancy Complications (Abortion & Ectopic Pregnancy)Document61 pagesEarly Pregnancy Complications (Abortion & Ectopic Pregnancy)በአምላክ ጋሻዬ በዛNo ratings yet
- FetalDocument2 pagesFetalHay PeeNo ratings yet
- Lecture IV IIIDocument32 pagesLecture IV IIIMohamad Alsayed AlasaasNo ratings yet
- 55 Lecture Abnormal Labor and Delivery, PeurperiumDocument62 pages55 Lecture Abnormal Labor and Delivery, PeurperiumTarek TarekNo ratings yet
- Ch. 21+22Document11 pagesCh. 21+22Gailstar GutierrezNo ratings yet
- 03.partus Immaturus, Prematurus, SerotinusDocument60 pages03.partus Immaturus, Prematurus, SerotinusSuci Rahayu Evasha100% (2)
- Preterm LaborDocument33 pagesPreterm LaborChristian MolinaNo ratings yet
- Premature LabourDocument3 pagesPremature LabourAnonymous Q236bSNo ratings yet
- Miscarriage 120812055232 Phpapp02Document79 pagesMiscarriage 120812055232 Phpapp02Feroz Haniff AzmaiNo ratings yet
- "Prevention of Preterm Parturition": Journal ReadingDocument23 pages"Prevention of Preterm Parturition": Journal ReadingRettyNo ratings yet
- Preterm and Posterm Birth: Oleh: DR Adi Setyawan Prianto SP - OG (K)Document31 pagesPreterm and Posterm Birth: Oleh: DR Adi Setyawan Prianto SP - OG (K)ATIKAH NUR HAFIZHAHNo ratings yet
- Miscarriage (Abortion) : (Adhesions Inside The Uterine Cavity)Document10 pagesMiscarriage (Abortion) : (Adhesions Inside The Uterine Cavity)Rashed Shatnawi100% (1)
- High Yield Obs & GynaeDocument84 pagesHigh Yield Obs & GynaeDrive RashNo ratings yet
- PRETERM DELIVERY With NARRATIONDocument23 pagesPRETERM DELIVERY With NARRATIONamanda deonananNo ratings yet
- Topics Today: Normal Puerperium Diseases of Puerperium Ectopic Pregnancy AbortionDocument52 pagesTopics Today: Normal Puerperium Diseases of Puerperium Ectopic Pregnancy AbortionBitto_Singh_5952No ratings yet
- Preterm LaborDocument41 pagesPreterm LaborAdistri Kim100% (3)
- Seminar G2 (Early Trimester Pregnancy Vaginal Bleeding)Document47 pagesSeminar G2 (Early Trimester Pregnancy Vaginal Bleeding)Chalie MequanentNo ratings yet
- Early Pregnancy Bleeding: 1. Abortion 2. Ectopic Pregnancy 3. GTDDocument48 pagesEarly Pregnancy Bleeding: 1. Abortion 2. Ectopic Pregnancy 3. GTDGebremichael Reta100% (2)
- Premature BirthsDocument3 pagesPremature BirthsZeynep YılmaztürkNo ratings yet
- Acute Abdomen in Pregnancy 2Document54 pagesAcute Abdomen in Pregnancy 2jhobarryNo ratings yet
- Dr. Deviana S. Riu, SpogDocument19 pagesDr. Deviana S. Riu, SpogmasyfuqNo ratings yet
- Postterm Pregnancy - UpToDateDocument17 pagesPostterm Pregnancy - UpToDateJosé Abraham Amaya DuarteNo ratings yet
- Antenatal AssessmentDocument40 pagesAntenatal AssessmentKailash NagarNo ratings yet
- Post Term Pregnancy: Dr. M.C.BansalDocument31 pagesPost Term Pregnancy: Dr. M.C.BansalAnonymous ON3Qpn9ZNo ratings yet
- 8) PROM - and PTBDocument38 pages8) PROM - and PTBmameekasim75No ratings yet
- Main Areas: Prenatal CareDocument11 pagesMain Areas: Prenatal Caresumit rawatNo ratings yet
- Preterm LaborDocument21 pagesPreterm LaborrranindyaprabasaryNo ratings yet
- Abortion and Postabortal CareDocument38 pagesAbortion and Postabortal Caremugabe Kabingira JrNo ratings yet
- Management Ectopic Pregnancy SLCOGDocument9 pagesManagement Ectopic Pregnancy SLCOGMelissa Aina Mohd YusofNo ratings yet
- NCM 109-Module 1 Lesson 1Document30 pagesNCM 109-Module 1 Lesson 1MARY ROSE DOLOGUINNo ratings yet
- Parto Prematuro ACOGDocument10 pagesParto Prematuro ACOGAngela_Maria_M_7864No ratings yet
- 2.early Pregnancy and BleedingDocument79 pages2.early Pregnancy and BleedingjosephNo ratings yet
- Preterm Labor: Ahmed Barefah Ahmed Al-Ghamdi Mohammed Al-TalhiDocument52 pagesPreterm Labor: Ahmed Barefah Ahmed Al-Ghamdi Mohammed Al-TalhiAdams Westlifer SophianoNo ratings yet
- Preterm Postterm Prom1Document35 pagesPreterm Postterm Prom1api-3856051No ratings yet
- Vaginal Bleeding in Early PregnancyDocument8 pagesVaginal Bleeding in Early PregnancyBal Ri Mekoleu100% (1)
- Prevention of Preterm Parturition: Jay D. Iams, M.DDocument20 pagesPrevention of Preterm Parturition: Jay D. Iams, M.DdiajengrainNo ratings yet
- Post Term Pregnancy: Dr. DR Letta S Lintang, M.Ked (OG), SP - OG (K)Document14 pagesPost Term Pregnancy: Dr. DR Letta S Lintang, M.Ked (OG), SP - OG (K)Paul Behring ManurungNo ratings yet
- Key Points: GuidelinesDocument4 pagesKey Points: GuidelinesJefri EfendiNo ratings yet
- Preterm Labour: Muhammad Hanif Final Year MBBSDocument32 pagesPreterm Labour: Muhammad Hanif Final Year MBBSArslan HassanNo ratings yet
- Abortion: L Sekhavat MD Ob & GynDocument38 pagesAbortion: L Sekhavat MD Ob & GynNurulAqilahZulkifliNo ratings yet
- Vital StatisticsDocument22 pagesVital Statisticssavita hanamsagarNo ratings yet
- The Management of Preterm Labor: Robert L. GoldenbergDocument18 pagesThe Management of Preterm Labor: Robert L. GoldenbergMarjorie Eliana MorejónNo ratings yet
- Preterm Labor and Prelabor Rupture of Membranes (Document35 pagesPreterm Labor and Prelabor Rupture of Membranes (Gendis Giona SudjaNo ratings yet
- Threatened Abortion PDFDocument3 pagesThreatened Abortion PDFAizat KamalNo ratings yet
- Preterm LaborDocument29 pagesPreterm LaborBer AnneNo ratings yet
- Gestational ConditionsDocument148 pagesGestational ConditionsEsvinch EsvinchNo ratings yet
- Preterm BirthDocument11 pagesPreterm Birthmendato marcabanNo ratings yet
- Abortion and Post-Abortion Care Abortion and Post-Abortion CareDocument48 pagesAbortion and Post-Abortion Care Abortion and Post-Abortion CareKerod AbebeNo ratings yet
- High-Risk Labor & Delivery Client & Her FamilyDocument68 pagesHigh-Risk Labor & Delivery Client & Her FamilyJAMES ROD MARINDUQUENo ratings yet
- AbortionDocument35 pagesAbortionZahida Aida Ida Paramore100% (1)
- Abortion TypesDocument19 pagesAbortion TypesFany MaldoNo ratings yet
- Pregnancy-Related Hypertension: Subdept. of Obstetrics & Gynecology Dr. Ramelan Indonesian Naval Hospital SurabayaDocument34 pagesPregnancy-Related Hypertension: Subdept. of Obstetrics & Gynecology Dr. Ramelan Indonesian Naval Hospital SurabayaSonyaSellyHNo ratings yet
- New Born ClassificationDocument47 pagesNew Born ClassificationEyob MizanNo ratings yet
- Getting Pregnant Faster: Step-By-Step Guide To Achieving PregnancyFrom EverandGetting Pregnant Faster: Step-By-Step Guide To Achieving PregnancyNo ratings yet
- Treatment Strategy for Unexplained Infertility and Recurrent MiscarriageFrom EverandTreatment Strategy for Unexplained Infertility and Recurrent MiscarriageKeiji KurodaNo ratings yet
- HealthScouter Pregnancy: Pregnancy Stages and New Mother Self Advocate GuideFrom EverandHealthScouter Pregnancy: Pregnancy Stages and New Mother Self Advocate GuideNo ratings yet
- ELEMAN HSEMS - Safety Management System PDFDocument64 pagesELEMAN HSEMS - Safety Management System PDFZafar SiddiquiNo ratings yet
- Bahasa Inggris Soal LatihanDocument38 pagesBahasa Inggris Soal LatihanIndah PramantiNo ratings yet
- PED 5 Heat ExchangersDocument74 pagesPED 5 Heat ExchangersDiogo EstevesNo ratings yet
- Viruses Wanted PosterDocument2 pagesViruses Wanted Posterapi-318809591No ratings yet
- Erection and Painting of Steel StructureDocument7 pagesErection and Painting of Steel StructureTAHER AMMARNo ratings yet
- 11 JMSCRDocument6 pages11 JMSCRWuppuluri Jayanth Kumar SharmaNo ratings yet
- Igneous RocksDocument7 pagesIgneous RocksHamzaBaigNo ratings yet
- HX400D6R AFJE3E 355CC-125 400-3-50 DatasheetDocument1 pageHX400D6R AFJE3E 355CC-125 400-3-50 DatasheetNduP78No ratings yet
- A Study On Customer Satisfaction Towards Herbal Products Dr. K. S. Kavitha & T. Anish FathimaDocument4 pagesA Study On Customer Satisfaction Towards Herbal Products Dr. K. S. Kavitha & T. Anish Fathimasangeetha0% (1)
- Text WinnicottDocument44 pagesText WinnicottCharlotte Betti100% (1)
- 3 - Trainees Record BookDocument6 pages3 - Trainees Record BookNelgen PiolaNo ratings yet
- Planning Considerations For Ice PlantsDocument5 pagesPlanning Considerations For Ice PlantsribozymesNo ratings yet
- Road Safety Training DocumentsDocument25 pagesRoad Safety Training DocumentsAbdullah Al BakyNo ratings yet
- Effect of Mulch On Soil TemperatureDocument11 pagesEffect of Mulch On Soil TemperatureEzeugo NelsonNo ratings yet
- Feel The Difference Owner'S Handbook: FordrangerDocument156 pagesFeel The Difference Owner'S Handbook: FordrangerGammy ZhammyNo ratings yet
- Central Venous Pressure Monitoring.: DR Jyothsna Chairperson DR Sunil ChhabriaDocument24 pagesCentral Venous Pressure Monitoring.: DR Jyothsna Chairperson DR Sunil ChhabriaPriyanka MaiyaNo ratings yet
- Hazard Assessment Report Legaspi AlbayDocument7 pagesHazard Assessment Report Legaspi AlbayJosh 施志勇 HarderNo ratings yet
- Planificare Engleza 0Document7 pagesPlanificare Engleza 0danielasiposNo ratings yet
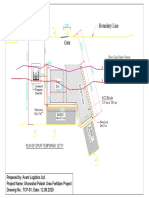
- Boundary Line: Plan of Gpuff Temporary JettyDocument1 pageBoundary Line: Plan of Gpuff Temporary Jettyshafiq_05No ratings yet
- Chapter 16 Amino Acids, Proteins, and EnzymesDocument92 pagesChapter 16 Amino Acids, Proteins, and EnzymesDennis ZhouNo ratings yet
- How To Make Lye For Natural Soap Making From Wood AshDocument7 pagesHow To Make Lye For Natural Soap Making From Wood AshMeim HakkasNo ratings yet
- Ved Vyas FinalDocument20 pagesVed Vyas FinalSunandaNo ratings yet
- Biochemical Biomarkers in Alzheimer's DiseaseDocument150 pagesBiochemical Biomarkers in Alzheimer's DiseaseInternational Medical PublisherNo ratings yet
- MSSL Annual Report 19 20Document427 pagesMSSL Annual Report 19 20gayatri suryakanthanNo ratings yet
- Tipe A - Test Admin Shopee ExpressDocument6 pagesTipe A - Test Admin Shopee ExpressHapsyah MarniNo ratings yet
- Unmsm/Fqiq/Epiq/Daadp/Inglés TÉCNICO/EF5/2020-I: Section V: The Impact of Chemical Engineering Design On SocietyDocument3 pagesUnmsm/Fqiq/Epiq/Daadp/Inglés TÉCNICO/EF5/2020-I: Section V: The Impact of Chemical Engineering Design On SocietyJuanLopezTrujilloNo ratings yet
- ISO 14001-Claus-4.4.1Document2 pagesISO 14001-Claus-4.4.1Navnath TamhaneNo ratings yet
- ERRV Survey Guidelines - Issue 5Document42 pagesERRV Survey Guidelines - Issue 5Hưng Lê TrungNo ratings yet