Download as pdf or txt
You might also like
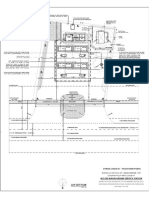
- Preliminary Plans Major Site Plan Application: Sheet List TableDocument31 pagesPreliminary Plans Major Site Plan Application: Sheet List TableJoey Klender100% (2)
- TEMA 28 23 Junio 2016Document5 pagesTEMA 28 23 Junio 2016ElenaSilvaNo ratings yet
- EndocrownDocument10 pagesEndocrowndhillaNo ratings yet
- 1 s2.0 S0300571222002780 MainDocument9 pages1 s2.0 S0300571222002780 Mainhermesugalde70No ratings yet
- Endocrown 2021Document19 pagesEndocrown 2021Valentina SilvaNo ratings yet
- Rocca, Rizcalla Krejci 2012Document7 pagesRocca, Rizcalla Krejci 2012Pablo BenitezNo ratings yet
- The Endocrown - A Different Type of All-Ceramic Reconstruction For Molars - JCDA - Essential Dental KnowledgeDocument8 pagesThe Endocrown - A Different Type of All-Ceramic Reconstruction For Molars - JCDA - Essential Dental KnowledgeJoel AlejandroNo ratings yet
- The Endocrown - A Different Type of All-Ceramic Reconstruction For Molars - JcdaDocument10 pagesThe Endocrown - A Different Type of All-Ceramic Reconstruction For Molars - Jcdaabcder1234No ratings yet
- Endo Crown: An Approach For Restoring Endodontically Treated Right Mandibular First Molars With Large Coronal Destruction - A Case ReportDocument7 pagesEndo Crown: An Approach For Restoring Endodontically Treated Right Mandibular First Molars With Large Coronal Destruction - A Case ReportIJAR JOURNALNo ratings yet
- Fracture Resistance and Failure Mode of Layered Translucent Zirconia With Different Crown DesignsDocument6 pagesFracture Resistance and Failure Mode of Layered Translucent Zirconia With Different Crown DesignsYrene Betancourt GarridoNo ratings yet
- Endocrown (DR - Roja)Document5 pagesEndocrown (DR - Roja)Shubham KingraNo ratings yet
- Ultrasonic Periodontal DebridementDocument9 pagesUltrasonic Periodontal DebridementAsus AsusNo ratings yet
- 1 s2.0 S168785741300005X MainDocument9 pages1 s2.0 S168785741300005X MainJose Luis MejiaNo ratings yet
- Etched Cast RestorationsDocument41 pagesEtched Cast Restorationssharanya chekkarrajNo ratings yet
- 1Document9 pages1Lakshmi PriyaNo ratings yet
- EPR2Document7 pagesEPR2RazvanAngheleNo ratings yet
- The Endocrown: An Alternative Approach For Restoring Extensively Damaged MolarsDocument8 pagesThe Endocrown: An Alternative Approach For Restoring Extensively Damaged MolarsHoàng Đình PhúcNo ratings yet
- Aboutara 2011Document4 pagesAboutara 2011Alejandra LorancaNo ratings yet
- Fracture Resistant Monolithic Dental CrownsDocument27 pagesFracture Resistant Monolithic Dental Crownscele22abNo ratings yet
- Zirconia CrownsDocument8 pagesZirconia CrownsClaudia Lizeth Ibarra DomínguezNo ratings yet
- Inlay Retained FPDDocument35 pagesInlay Retained FPDNikita AggarwalNo ratings yet
- Case Report: Restoration of Endodontically Treated Molars Using All Ceramic EndocrownsDocument6 pagesCase Report: Restoration of Endodontically Treated Molars Using All Ceramic EndocrownsTaufiqurrahman Abdul DjabbarNo ratings yet
- Fracture Resistance and Microleakage of Endocrowns Utilizing Three CAD-CAM BlocksDocument10 pagesFracture Resistance and Microleakage of Endocrowns Utilizing Three CAD-CAM BlocksZen AhmadNo ratings yet
- JResDent23144-4459922 122319 PDFDocument5 pagesJResDent23144-4459922 122319 PDFcindyannisamelatiNo ratings yet
- Lost Salt TechDocument4 pagesLost Salt TechNajeeb UllahNo ratings yet
- Adhesion 2Document6 pagesAdhesion 2Deisy Angarita FlorezNo ratings yet
- Case Report: Inlay-Retained Fixed Dental Prosthesis: A Clinical Option Using Monolithic ZirconiaDocument8 pagesCase Report: Inlay-Retained Fixed Dental Prosthesis: A Clinical Option Using Monolithic ZirconiaPoojitha ApvNo ratings yet
- ZirconiaDocument8 pagesZirconiaAmitNo ratings yet
- Articol L.O.C.Document0 pagesArticol L.O.C.Anda TarasciucNo ratings yet
- Microleakage of Restorative Materials: An in Vitro Study: M P., D S., S ADocument4 pagesMicroleakage of Restorative Materials: An in Vitro Study: M P., D S., S Apreethi.badamNo ratings yet
- Fernandesdacunha 2017Document7 pagesFernandesdacunha 2017Mauricio Hernández ValdezNo ratings yet
- Comparison of Different Restoration Techniques ForDocument7 pagesComparison of Different Restoration Techniques ForDiana Fitri MuslimahNo ratings yet
- Clinical Success of Zirconia in Dental Applications: KeywordsDocument5 pagesClinical Success of Zirconia in Dental Applications: KeywordsJulio TorresNo ratings yet
- Implementing Sandwich Technique With RMGI: (Resin-Modified Glass-Ionomer)Document8 pagesImplementing Sandwich Technique With RMGI: (Resin-Modified Glass-Ionomer)Firma Nurdinia DewiNo ratings yet
- 62 - The Open PDFDocument9 pages62 - The Open PDFSandeep Lal CherukaraNo ratings yet
- Acar 2021Document9 pagesAcar 2021HllerdNo ratings yet
- Zirconia Based CeramicsDocument13 pagesZirconia Based CeramicsJafar SadiqNo ratings yet
- TMP 1 E04Document5 pagesTMP 1 E04FrontiersNo ratings yet
- Hollow Dentures: Treatment Option For Atrophic Ridges. A Clinical ReportDocument21 pagesHollow Dentures: Treatment Option For Atrophic Ridges. A Clinical ReportArchitNo ratings yet
- Fiber-Reinforced Resin Coating For Endocrown Preparations.A Technical Report 12-139-trDocument7 pagesFiber-Reinforced Resin Coating For Endocrown Preparations.A Technical Report 12-139-trDan MPNo ratings yet
- Direct Posterior Composite 1Document33 pagesDirect Posterior Composite 1Rawzh Salih MuhammadNo ratings yet
- Influence of Different Posts and Cores On MarginalDocument10 pagesInfluence of Different Posts and Cores On Marginalfebriani serojaNo ratings yet
- Art of Debonding in OrthodonticsDocument2 pagesArt of Debonding in OrthodonticsmalifaragNo ratings yet
- Assessment of Fracture Resistance of Endocrown Constructed of Two Different Materials Compared To Conventional Post and Core Retained CrownDocument20 pagesAssessment of Fracture Resistance of Endocrown Constructed of Two Different Materials Compared To Conventional Post and Core Retained CrownDr-Ahmed Yahya ElRefaayNo ratings yet
- Effect of Different CAD-CAM Materials On The Marginal and Internal Adaptation of Endocrown Restorations: An in Vitro StudyDocument7 pagesEffect of Different CAD-CAM Materials On The Marginal and Internal Adaptation of Endocrown Restorations: An in Vitro StudyNetra TaleleNo ratings yet
- CAD CAM DigitalImpressionsDocument8 pagesCAD CAM DigitalImpressionsMircea ZaneaNo ratings yet
- The Effect of Finish Line Preparation and Layer Thickness On The Failure@0Document8 pagesThe Effect of Finish Line Preparation and Layer Thickness On The Failure@0Valery MontoyaNo ratings yet
- No Post-No Core Approach To Restore Severely Damaged Posterior Teeth - An Up To 10-Year Retrospective Study of Documented Endocrown CasesDocument7 pagesNo Post-No Core Approach To Restore Severely Damaged Posterior Teeth - An Up To 10-Year Retrospective Study of Documented Endocrown CasesDiana FreireNo ratings yet
- A Technique For Impressing The Severely Resorbed MDocument5 pagesA Technique For Impressing The Severely Resorbed MPradeep Prady100% (1)
- Molnár J - Dent Mater (2022)Document11 pagesMolnár J - Dent Mater (2022)floressam2000No ratings yet
- 01 Mahidol Dental Journal 3 2020Document10 pages01 Mahidol Dental Journal 3 2020shafira zulvaNo ratings yet
- ZIRCOMADocument4 pagesZIRCOMARatih CynthiaNo ratings yet
- Sectional CDDocument35 pagesSectional CDmithileshwaripatilNo ratings yet
- Endocrown Biacchi Basting 2012Document7 pagesEndocrown Biacchi Basting 2012Andre PereiraNo ratings yet
- Dental Research Journal: Marginal Adaptation of Spinell Inceram and Feldspathic Porcelain Laminate VeneersDocument6 pagesDental Research Journal: Marginal Adaptation of Spinell Inceram and Feldspathic Porcelain Laminate VeneersLuis Alberto Carpio MorenoNo ratings yet
- Nghiên Cứu Khả Năng Chống Gãy Của Mão Và Lớp Phủ Lithium Disilicate CADCAM Với Các Phương Pháp Khác (e.max CAD) (CEREC Tessera)Document7 pagesNghiên Cứu Khả Năng Chống Gãy Của Mão Và Lớp Phủ Lithium Disilicate CADCAM Với Các Phương Pháp Khác (e.max CAD) (CEREC Tessera)Nguyễn Đức TuấnNo ratings yet
- Jap 13 269Document12 pagesJap 13 269Sun TerawatNo ratings yet
- Comparision of Chamfer & Deep Chamfer PreparationDocument5 pagesComparision of Chamfer & Deep Chamfer Preparationjinny1_0No ratings yet
- The Science of Superhydrophobicity: Enhancing Outdoor Electrical InsulatorsFrom EverandThe Science of Superhydrophobicity: Enhancing Outdoor Electrical InsulatorsNo ratings yet
- OISD-129 GAP AnalysisDocument1 pageOISD-129 GAP AnalysisNayan AhmedNo ratings yet
- Lesson 1 Introduction To Accounting Theory & Overview of Theories in AccountingDocument69 pagesLesson 1 Introduction To Accounting Theory & Overview of Theories in AccountingDerek DadzieNo ratings yet
- GPH-BUET Test ReportDocument24 pagesGPH-BUET Test ReportAtikur RahmanNo ratings yet
- Flexible Budgets and Variance Analysis: © 2007 Pearson Education Canada Slide 12-1Document14 pagesFlexible Budgets and Variance Analysis: © 2007 Pearson Education Canada Slide 12-1nowthisisitkoolNo ratings yet
- 5.2 Production MethodsDocument3 pages5.2 Production MethodsGonzalo PastorNo ratings yet
- Negotiable Instruments Multiple Questions With AnswersDocument8 pagesNegotiable Instruments Multiple Questions With AnswersJust ForNo ratings yet
- Barro Sala-i-Martin - Convergence - 1992Document30 pagesBarro Sala-i-Martin - Convergence - 1992mgrotzNo ratings yet
- Data - Sheet - FP1 - 2102-100 - Active - Digital - 1060 (Refurb or Newer)Document2 pagesData - Sheet - FP1 - 2102-100 - Active - Digital - 1060 (Refurb or Newer)Basil HwangNo ratings yet
- Chain For Wet Scrapper ConveyorDocument18 pagesChain For Wet Scrapper ConveyorHarish AG workNo ratings yet
- Solutions Chapter 10Document7 pagesSolutions Chapter 10Nama SahajaNo ratings yet
- Evelyn Hone College of Applied Arts and Commerce School of Business Studies Human Resource SectionDocument4 pagesEvelyn Hone College of Applied Arts and Commerce School of Business Studies Human Resource SectionMichelo HabulemboNo ratings yet
- Mahalakshmi Service Station - Majjigepura PesoDocument1 pageMahalakshmi Service Station - Majjigepura PesoDileep K MahadevaiahNo ratings yet
- Trading Strategies Involving Options: Fundamentals of Futures and Options Markets, 6Document15 pagesTrading Strategies Involving Options: Fundamentals of Futures and Options Markets, 6rockman911No ratings yet
- DS (Pan Africanism)Document59 pagesDS (Pan Africanism)Eden Alvaro EmilyNo ratings yet
- Starter Activity: Complete The Worksheet Provided by Your Teacher!Document20 pagesStarter Activity: Complete The Worksheet Provided by Your Teacher!Pammi KumariNo ratings yet
- AmigurumiDocument5 pagesAmigurumiFn131No ratings yet
- Lessons4Ielts - Reading (2) - Page 106-113Document8 pagesLessons4Ielts - Reading (2) - Page 106-113Pham VuongNo ratings yet
- Ex. WorksheetDocument3 pagesEx. WorksheetAllysa Kim RubisNo ratings yet
- Portfolio Theory Exam 2020 With SolutionDocument4 pagesPortfolio Theory Exam 2020 With SolutionFARAH BENDALINo ratings yet
- Fakey Trading Strategy (Inside Bar False Break Out)Document8 pagesFakey Trading Strategy (Inside Bar False Break Out)Doug Trudell100% (1)
- Akshaya Nidhi Case SummaryDocument3 pagesAkshaya Nidhi Case SummaryAnanda BudiNo ratings yet
- Ebook Economics A Contemporary Introduction 10Th Edition Mceachern Solutions Manual Full Chapter PDFDocument36 pagesEbook Economics A Contemporary Introduction 10Th Edition Mceachern Solutions Manual Full Chapter PDFpauldiamondwe8100% (13)
- Kadar PB Sebelum Dan Setelah Di Beri Perlakuan: Lampiran 4. Output Hasil Analisis Data Dengan SPSSDocument3 pagesKadar PB Sebelum Dan Setelah Di Beri Perlakuan: Lampiran 4. Output Hasil Analisis Data Dengan SPSSaverinaNo ratings yet
- Cma Final SCM - Vol 1Document405 pagesCma Final SCM - Vol 1Pritam patelNo ratings yet
- Microeconomics An Intuitive Approach With Calculus 2nd Edition Thomas Nechyba Test Bank 1Document7 pagesMicroeconomics An Intuitive Approach With Calculus 2nd Edition Thomas Nechyba Test Bank 1shirley100% (58)
- Cluster Profile Belgaum Foundries: KarnatakaDocument14 pagesCluster Profile Belgaum Foundries: KarnatakaSonal PatelNo ratings yet
- Chapter 3 Appendix ADocument16 pagesChapter 3 Appendix AJingjing ZhuNo ratings yet
- Cheque Requisition Form SampleDocument1 pageCheque Requisition Form SamplehenaediNo ratings yet
- Copyright Bar ExamDocument18 pagesCopyright Bar ExamVance Ceballos100% (1)