Download as pdf or txt
You might also like
- Giles Set A1 PDFDocument46 pagesGiles Set A1 PDFPrinting CoNo ratings yet
- Kanabur2017nail and Locking Plate For Periprosthetic FracturesDocument7 pagesKanabur2017nail and Locking Plate For Periprosthetic FracturesLenin EstrellaNo ratings yet
- FX of Distal HumerusDocument76 pagesFX of Distal HumerusGrace NazarenoNo ratings yet
- DHS Screw Position JEDocument8 pagesDHS Screw Position JEDan IonescuNo ratings yet
- High Tibial OsteotomiesDocument24 pagesHigh Tibial OsteotomiesMuhamad Izwan Bin HanafiNo ratings yet
- U05-Distal Humerus FracturesDocument84 pagesU05-Distal Humerus FracturesAmina BentratNo ratings yet
- Complications and Outcomes of The Transfibular Approach For Posterolateral Fractures of The Tibial Plateau PDFDocument19 pagesComplications and Outcomes of The Transfibular Approach For Posterolateral Fractures of The Tibial Plateau PDFSergio Tomas Cortés MoralesNo ratings yet
- Surgeons - Total Acetabular Allografts ( (Dagger) ) Instructional Course Lectures, The American Academy of OrthopaedicDocument13 pagesSurgeons - Total Acetabular Allografts ( (Dagger) ) Instructional Course Lectures, The American Academy of OrthopaedicYariel AraujoNo ratings yet
- Managementofdistal Femurfracturesinadults: An Overview of OptionsDocument12 pagesManagementofdistal Femurfracturesinadults: An Overview of OptionsDoctor's BettaNo ratings yet
- Fai 2007 0529Document7 pagesFai 2007 0529milenabogojevskaNo ratings yet
- 018 Scorpio TS Single Axis Revision Knee System Surgical ProtocolDocument19 pages018 Scorpio TS Single Axis Revision Knee System Surgical ProtocolDinis RegoNo ratings yet
- Thesis PresentationDocument44 pagesThesis Presentationberhe59076362No ratings yet
- New Principles in Pilon Fractres ManagementDocument17 pagesNew Principles in Pilon Fractres ManagementCamila FontechaNo ratings yet
- Primary Total Knee Arthroplasty For Acute Fracture Around The KneeDocument10 pagesPrimary Total Knee Arthroplasty For Acute Fracture Around The KneesaraNo ratings yet
- Implant Selection in Revision Total Knee ArthroplastyDocument10 pagesImplant Selection in Revision Total Knee ArthroplastyAndrés KnubelNo ratings yet
- FR Distal HumerusDocument55 pagesFR Distal Humerusiisscribd100% (1)
- Intertrochanteric MEDSCAPEDocument5 pagesIntertrochanteric MEDSCAPESpica AdharaNo ratings yet
- Ankle FracturesDocument133 pagesAnkle FracturesAtiekPalludaNo ratings yet
- Optimizing Stability in Distal Humeral Fracture Fixation: Historical PerspectiveDocument9 pagesOptimizing Stability in Distal Humeral Fracture Fixation: Historical PerspectiveNazir KhanNo ratings yet
- Compression FractureDocument4 pagesCompression FracturepuchioNo ratings yet
- Basic Arthroplasty - Unit 4 - Bone Loss BacksteinDocument9 pagesBasic Arthroplasty - Unit 4 - Bone Loss BacksteinShu Yang HuNo ratings yet
- Whatistheroleandlimitof Calcanealosteotomyinthe Cavovarusfoot?Document18 pagesWhatistheroleandlimitof Calcanealosteotomyinthe Cavovarusfoot?Anonymous kdBDppigENo ratings yet
- Neglected Femoral Neck Fractures in AdultsDocument21 pagesNeglected Femoral Neck Fractures in AdultsJauharil Wafi MuhammadNo ratings yet
- Intertrochanteric Hip Fractures PDFDocument9 pagesIntertrochanteric Hip Fractures PDFSivaneasan KandiahNo ratings yet
- Clavicle AC SC JointsDocument97 pagesClavicle AC SC Jointsdr.maulanahutabaratNo ratings yet
- Injury: Jian Zou, Wei Zhang, Chang-Qing ZhangDocument5 pagesInjury: Jian Zou, Wei Zhang, Chang-Qing Zhangfebyan yohanesNo ratings yet
- Intertrochanteric FractureDocument9 pagesIntertrochanteric FractureYovita Devi Kornelin100% (1)
- Artigo ClamshellDocument15 pagesArtigo ClamshellbritocirurgiadamaoNo ratings yet
- Jurnal Medikal PDFDocument9 pagesJurnal Medikal PDFAgus SetiawanNo ratings yet
- Presentation 1Document16 pagesPresentation 1Moiz AliNo ratings yet
- m4 Lecture 1 Ortho IntroDocument72 pagesm4 Lecture 1 Ortho IntroAqeel RehmanNo ratings yet
- FracturesDocument26 pagesFracturesMelinda MelinNo ratings yet
- Trochanteric #Document20 pagesTrochanteric #Prakash AyyaduraiNo ratings yet
- Basti As 2020Document17 pagesBasti As 2020Martin MoranNo ratings yet
- Seminar 13Document60 pagesSeminar 13radhikamiNo ratings yet
- Management of Bone Defects in Primary Knee Arthroplasty: A Case ReportDocument4 pagesManagement of Bone Defects in Primary Knee Arthroplasty: A Case ReportInternational Journal of Recent Innovations in Academic ResearchNo ratings yet
- Pre-Operative Conference: Trauma 4 Service Jafer Terrence Lim, M.DDocument22 pagesPre-Operative Conference: Trauma 4 Service Jafer Terrence Lim, M.DjcreynesNo ratings yet
- Sakurakichi 2008Document3 pagesSakurakichi 2008dr.aseemb4uNo ratings yet
- TotalHip PDFDocument11 pagesTotalHip PDFLoredanaNovacNo ratings yet
- Bonegrafting 180324163620Document105 pagesBonegrafting 180324163620Ankit Damor100% (1)
- Masquelet TechniqueDocument40 pagesMasquelet TechniqueasioquaNo ratings yet
- Cu Adric Ep Last I Are Vista RobinsonDocument8 pagesCu Adric Ep Last I Are Vista RobinsontomimacagnoNo ratings yet
- U04 Fxs of Humeral ShaftDocument88 pagesU04 Fxs of Humeral Shaftadrian_mogosNo ratings yet
- Proximal Femoral NewDocument34 pagesProximal Femoral NewHimanshu HemantNo ratings yet
- Surgical Challenges in Complex Primary Total Hip ADocument9 pagesSurgical Challenges in Complex Primary Total Hip Aehabede6445No ratings yet
- S-Malunion - Principals and ManagementDocument45 pagesS-Malunion - Principals and ManagementshahnazroeentanmailNo ratings yet
- Manejo de Fracturas Mediales de Cadera 2015 Femoral Neck Fractures - Current ManagementDocument9 pagesManejo de Fracturas Mediales de Cadera 2015 Femoral Neck Fractures - Current ManagementSergio Tomas Cortés MoralesNo ratings yet
- Osteoporotic Vertebral Compression Fracture - TreaDocument4 pagesOsteoporotic Vertebral Compression Fracture - TreaChristopherLawrenceNo ratings yet
- 10 1016@j Jos 2016 04 015Document7 pages10 1016@j Jos 2016 04 015osmann52No ratings yet
- Distal Humerus FXDocument37 pagesDistal Humerus FXjomari dvNo ratings yet
- How To Read A Postoperative Knee Replacement RadiographDocument9 pagesHow To Read A Postoperative Knee Replacement RadiographNegru TeodorNo ratings yet
- Orthopedic Essentials in Emergency MedicineDocument35 pagesOrthopedic Essentials in Emergency MedicineMohd Tarmizi100% (1)
- Trauma OITE - 2012 2013 2014Document543 pagesTrauma OITE - 2012 2013 2014ICH KhuyNo ratings yet
- Hume Ro Prox SutDocument15 pagesHume Ro Prox Sutbenife8420No ratings yet
- Retrieve 5Document12 pagesRetrieve 5Muhammad Iqbal FadillahNo ratings yet
- Tibial Plateau Fractures: Yasser AlwabliDocument35 pagesTibial Plateau Fractures: Yasser AlwabliPin Han NaNo ratings yet
- Use of Iliac Crest Bone Graft in Neglected Neck of Femur FractureDocument126 pagesUse of Iliac Crest Bone Graft in Neglected Neck of Femur Fracturetatha.bajjioNo ratings yet
- S g18 Malunions 161225224920Document53 pagesS g18 Malunions 161225224920shahnazroeentanmailNo ratings yet
- Orthopaedic Surgery - 2014 - Wang - Biomechanical Analysis of Four Types of Internal Fixation in Subtrochanteric FractureDocument9 pagesOrthopaedic Surgery - 2014 - Wang - Biomechanical Analysis of Four Types of Internal Fixation in Subtrochanteric FracturePradeepa GNo ratings yet
- Short ImplantsFrom EverandShort ImplantsBoyd J. TomasettiNo ratings yet
- Advances in Knee Ligament and Knee Preservation SurgeryFrom EverandAdvances in Knee Ligament and Knee Preservation SurgeryNorimasa NakamuraNo ratings yet
- Chatziagorou2019surgical Treatment of Vancouver Type BDocument12 pagesChatziagorou2019surgical Treatment of Vancouver Type BLenin EstrellaNo ratings yet
- Kanabur2017nail and Locking Plate For Periprosthetic FracturesDocument7 pagesKanabur2017nail and Locking Plate For Periprosthetic FracturesLenin EstrellaNo ratings yet
- Briant-Evans2009cement-In-Cement Stem Revision For Vancouver Type B Periprosthetic Femoral Fractures After Total Hip ArthroplastyDocument6 pagesBriant-Evans2009cement-In-Cement Stem Revision For Vancouver Type B Periprosthetic Femoral Fractures After Total Hip ArthroplastyLenin EstrellaNo ratings yet
- Khan 2017 ReviewDocument9 pagesKhan 2017 ReviewLenin EstrellaNo ratings yet
- Biomechanics of The Knee JointDocument31 pagesBiomechanics of The Knee JointnovitaNo ratings yet
- WFSR 44004710107 PDFDocument26 pagesWFSR 44004710107 PDFAyub Anwar M-SalihNo ratings yet
- AnkleDocument13 pagesAnklesadiaNo ratings yet
- Calcaneal SpurDocument19 pagesCalcaneal SpurucssNo ratings yet
- Tratamiento Quirurgico de La SindactiliaDocument13 pagesTratamiento Quirurgico de La SindactiliaJose Alejandro Cobas PazNo ratings yet
- 4.abdomen and Pelvis Gross SpottersDocument122 pages4.abdomen and Pelvis Gross Spottersmatt medmedmedicNo ratings yet
- Tort Law Lecture 5 - Breach of Duty: Ms GallopDocument43 pagesTort Law Lecture 5 - Breach of Duty: Ms GallopABDOULIENo ratings yet
- Definition of Damage Control OrthopaedicsDocument2 pagesDefinition of Damage Control OrthopaedicsHerryanto Agustriadi100% (1)
- Body Movements Class 6 SciDocument2 pagesBody Movements Class 6 SciHardik Pancholi100% (1)
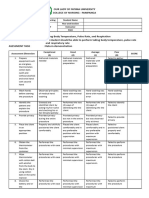
- Health Assessment Rubrics 1Document40 pagesHealth Assessment Rubrics 1bagangsbNo ratings yet
- Self PNF Stretching Calf - Google SearchDocument1 pageSelf PNF Stretching Calf - Google SearchKobe ChungNo ratings yet
- Introduction To Anatomy and Physiology: Unit IDocument55 pagesIntroduction To Anatomy and Physiology: Unit ILara C.No ratings yet
- 90-91-054 Rev A Manual - MEERKATDocument338 pages90-91-054 Rev A Manual - MEERKATbrasgNo ratings yet
- 1-1 Anatomie Des Extenseurs Des Doigts LongsDocument20 pages1-1 Anatomie Des Extenseurs Des Doigts LongsProfesseur Christian DumontierNo ratings yet
- Injury Report Form: Circle and NameDocument1 pageInjury Report Form: Circle and NameNinNo ratings yet
- Contemporary Management Pediatric Craniofacial InjuriesDocument8 pagesContemporary Management Pediatric Craniofacial InjuriesTabishur RahmanNo ratings yet
- Laminectomy Tumor Resection - Case ReportDocument8 pagesLaminectomy Tumor Resection - Case Reportshara rachmawatiNo ratings yet
- Legal Medicine Reviewer (Part 1)Document3 pagesLegal Medicine Reviewer (Part 1)Rey Gabriel ObandoNo ratings yet
- Psychology Essay QuestionsDocument4 pagesPsychology Essay Questionsovexvenbf100% (2)
- Fractures of Clavicle 1Document41 pagesFractures of Clavicle 1Noor Al Zahraa AliNo ratings yet
- Chapter 3. Tissue - RepairDocument55 pagesChapter 3. Tissue - RepairMohamed NourNo ratings yet
- Unit 8 Non - Fatal Offences Against The Person LectureDocument29 pagesUnit 8 Non - Fatal Offences Against The Person LectureElliot Mfune Jr.No ratings yet
- Indicaciones Colgajo Inguinal MusloDocument10 pagesIndicaciones Colgajo Inguinal MusloMATTHEWS1No ratings yet
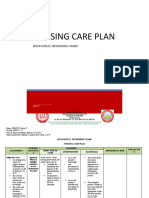
- Nursing Care PlanDocument5 pagesNursing Care PlanColeen PequitNo ratings yet
- Biomechanics PDFDocument55 pagesBiomechanics PDFKinjal SharmaNo ratings yet
- Mapeh 5 ModuleDocument19 pagesMapeh 5 ModuleSharamae CarpioNo ratings yet
- The Major Categories of Wound Previously DescribedDocument40 pagesThe Major Categories of Wound Previously DescribedAri Sri WulandariNo ratings yet
- Amputation Rehabilitation and Prosthetic Restoration. From Surgery To Community ReintegrationDocument7 pagesAmputation Rehabilitation and Prosthetic Restoration. From Surgery To Community ReintegrationGabriela Istrati-StanciugelNo ratings yet
- Musculoskeletal TraumaDocument19 pagesMusculoskeletal Traumamunazzarehman37No ratings yet