Download as pdf or txt
You might also like
- Kenneth Clark PDFDocument12 pagesKenneth Clark PDFsuryanandiniNo ratings yet
- Diagnosis of Osteoporosis and Assessment of Fracture Risk John A Kanis 2002Document8 pagesDiagnosis of Osteoporosis and Assessment of Fracture Risk John A Kanis 2002Jossie AcuñaNo ratings yet
- Jonathan M. Lacombe, Randall J. Roper T: Review ArticleDocument9 pagesJonathan M. Lacombe, Randall J. Roper T: Review ArticleMaría Paula Caballero BarbosaNo ratings yet
- BMD AssignmentDocument21 pagesBMD Assignment00074216No ratings yet
- Overview of DEXA - UpToDateDocument20 pagesOverview of DEXA - UpToDatemartinus putra muliaNo ratings yet
- Osteoporosis: A Review: June 2016Document8 pagesOsteoporosis: A Review: June 2016Yolan TiaraNo ratings yet
- Osteoporosis A ReviewDocument8 pagesOsteoporosis A ReviewIga AmanyzNo ratings yet
- OsteoporosisDocument8 pagesOsteoporosisSoraya FadhilahNo ratings yet
- (1479683X - European Journal of Endocrinology) The Bone Mass Concept - Problems in Short StatureDocument5 pages(1479683X - European Journal of Endocrinology) The Bone Mass Concept - Problems in Short StatureDeyan SyambasNo ratings yet
- The Effect of Icariin On Bone Metabolism and Its Potential Clinical ApplicationDocument12 pagesThe Effect of Icariin On Bone Metabolism and Its Potential Clinical ApplicationBrenda MartinsNo ratings yet
- Osteoporosis A ReviewDocument8 pagesOsteoporosis A ReviewAliza MustafaNo ratings yet
- A Summary of Advancements in Osteoporosis ManagementDocument4 pagesA Summary of Advancements in Osteoporosis ManagementHerald Scholarly Open AccessNo ratings yet
- Overview of Osteoporosis: Why Be Concerned About Osteoporosis?Document22 pagesOverview of Osteoporosis: Why Be Concerned About Osteoporosis?Gabriela MelinteNo ratings yet
- SCI135 Research Project - EditedDocument4 pagesSCI135 Research Project - EditedRachael KaburuNo ratings yet
- Bone Mineral Density (BMD) : February 2017Document3 pagesBone Mineral Density (BMD) : February 2017Ersa Aqilla HayaNo ratings yet
- Prof. Dr. Hazem Abd El-Azeem Professor of Orthopaedic Surgery Cairo UniversityDocument47 pagesProf. Dr. Hazem Abd El-Azeem Professor of Orthopaedic Surgery Cairo UniversitytarikeopsNo ratings yet
- E-1-Osteoporosis and Periodontitis 2016Document14 pagesE-1-Osteoporosis and Periodontitis 2016Yessid Baltazar Arango100% (1)
- Pathophysiology of Bone MetastasesDocument5 pagesPathophysiology of Bone MetastasesdyahNo ratings yet
- JCM 11 00699Document20 pagesJCM 11 00699OstazNo ratings yet
- Didier Hans, Nicole Barthe, Stephanie Boutroy, Laurent Pothuaud, Renaud Winzenrieth and Marc-Antoine KriegDocument11 pagesDidier Hans, Nicole Barthe, Stephanie Boutroy, Laurent Pothuaud, Renaud Winzenrieth and Marc-Antoine KriegkwafqjwqnyNo ratings yet
- Metabolic Bone DiseaseDocument6 pagesMetabolic Bone Diseasekartini ciatawiNo ratings yet
- Osteoporosis: Best PracticeDocument7 pagesOsteoporosis: Best PracticePerez Wahyu PurnasariNo ratings yet
- Relationship Between Osteoporosis and Periodontal Disease: Review of The LiteratureDocument9 pagesRelationship Between Osteoporosis and Periodontal Disease: Review of The Literatureaakanksha bhardwajNo ratings yet
- Asupan Mineral, Kadar Kolesterol Total Dan Kepadatan Mineral Tulang Pada LansiaDocument6 pagesAsupan Mineral, Kadar Kolesterol Total Dan Kepadatan Mineral Tulang Pada LansiaLutfia Ardina OFFICIALNo ratings yet
- Os 1 251Document7 pagesOs 1 251mukhlis akmalNo ratings yet
- JCM 11 06434 v2Document17 pagesJCM 11 06434 v2NeelamNo ratings yet
- Tto de La Osteoporosis - 2020Document16 pagesTto de La Osteoporosis - 2020GilbertoNo ratings yet
- Asupan Mineral, Kadar Kolesterol Total Dan Kepadatan Mineral Tulang Pada LansiaDocument6 pagesAsupan Mineral, Kadar Kolesterol Total Dan Kepadatan Mineral Tulang Pada Lansiadwi elma safitriNo ratings yet
- Orthopaedic Surgery - 2019 - Qu - Bone Turnover Markers and Bone Mineral Density To Predict Osteoporotic Fractures in OlderDocument8 pagesOrthopaedic Surgery - 2019 - Qu - Bone Turnover Markers and Bone Mineral Density To Predict Osteoporotic Fractures in OlderAlfred AlfredNo ratings yet
- Osteoporosis: Current Concepts: Ibrahim Akkawi Hassan ZmerlyDocument6 pagesOsteoporosis: Current Concepts: Ibrahim Akkawi Hassan ZmerlyDimas M IlhamNo ratings yet
- A Biomechanical Perspective On Bone QualityDocument18 pagesA Biomechanical Perspective On Bone QualityGustavo Del PinoNo ratings yet
- Porose CKD e Osso - Qualidade Ossea 2017Document7 pagesPorose CKD e Osso - Qualidade Ossea 2017Ben-Hur AlbergariaNo ratings yet
- Lorentz On 2015Document23 pagesLorentz On 2015Sanita AurinNo ratings yet
- Screening For Osteoporosis - UpToDateDocument22 pagesScreening For Osteoporosis - UpToDatesindy suarezNo ratings yet
- High Prevalence of Vitamin D Deficiency and Osteoporosis in Patients With Fragility Fractures of Hip - A Pilot StudyDocument4 pagesHigh Prevalence of Vitamin D Deficiency and Osteoporosis in Patients With Fragility Fractures of Hip - A Pilot StudyDiah Rindayani HasbiNo ratings yet
- Differentiating The Causes of Adynamic Bone in Advanced Chro - 2021 - Kidney IntDocument13 pagesDifferentiating The Causes of Adynamic Bone in Advanced Chro - 2021 - Kidney IntGeorgiana BunghiuzNo ratings yet
- Varianta OriginalaDocument3 pagesVarianta Originalaiahim_ulizamNo ratings yet
- OsteoporosisDocument18 pagesOsteoporosisErica ValladaresNo ratings yet
- Clinical Use Bone DensitometryDocument10 pagesClinical Use Bone Densitometryfildzah amalyaNo ratings yet
- Bone Reports: A A B C C B CDocument9 pagesBone Reports: A A B C C B Caeroforce20No ratings yet
- Monostotic Fibrous Dysplasia of The Mandible: Oral Health and Dental Management June 2014Document5 pagesMonostotic Fibrous Dysplasia of The Mandible: Oral Health and Dental Management June 2014Narito NianNo ratings yet
- Perez Et Al. - 2018 - Tissue Engineering and Cell-Based Therapies For Fractures and Bone DefectsDocument23 pagesPerez Et Al. - 2018 - Tissue Engineering and Cell-Based Therapies For Fractures and Bone DefectsAlif FakhriNo ratings yet
- Osteoporosis in The Aging Male: Treatment Options: BackgroundDocument16 pagesOsteoporosis in The Aging Male: Treatment Options: BackgroundcumbredinNo ratings yet
- 1042 FullDocument9 pages1042 Fulloki harisandiNo ratings yet
- Surgical Treatment of Severe Osteoporosis Includin-DikonversiDocument6 pagesSurgical Treatment of Severe Osteoporosis Includin-DikonversikhairaniNo ratings yet
- Bone Mineral DensityDocument5 pagesBone Mineral DensityMd Ahsanuzzaman PinkuNo ratings yet
- Management of Osteoporosis in CKD: Pascale Khairallah and Thomas L. NickolasDocument8 pagesManagement of Osteoporosis in CKD: Pascale Khairallah and Thomas L. NickolasSlr RandiNo ratings yet
- Management of Severe OsteoporosisDocument16 pagesManagement of Severe OsteoporosisZendy Nicole Cano SaavedraNo ratings yet
- Edit BMD and Bone QualityDocument74 pagesEdit BMD and Bone QualityBenny Chris TantoNo ratings yet
- C Eller 2020 Q2Document18 pagesC Eller 2020 Q2NasriNo ratings yet
- Jurnal 3 - Osteoarthritis Bone Marrow LesionsDocument7 pagesJurnal 3 - Osteoarthritis Bone Marrow LesionsAndre PratamaNo ratings yet
- Articulo 1 CX DecimoDocument6 pagesArticulo 1 CX Decimodentist booksNo ratings yet
- Osteoporosis 1Document22 pagesOsteoporosis 1Júlia LedesmaNo ratings yet
- Guidelines For Diagnosis and Management of OsteoporosisDocument17 pagesGuidelines For Diagnosis and Management of OsteoporosisVanessaCockerNo ratings yet
- Bone Tumors Differential DiagnosisDocument12 pagesBone Tumors Differential DiagnosisNahuel ColinaNo ratings yet
- Osteoporose Diagnóstico-1Document17 pagesOsteoporose Diagnóstico-1Rayanne SilvaNo ratings yet
- 2020 A Contemporary View of The Definition and Diagnosis of Osteoporosis in Children and AdolescentsDocument10 pages2020 A Contemporary View of The Definition and Diagnosis of Osteoporosis in Children and AdolescentsRaisa SugoroNo ratings yet
- Bone Disease in Chronic Kidney Disease and Kidney TransplantDocument27 pagesBone Disease in Chronic Kidney Disease and Kidney TransplantBhanu KumarNo ratings yet
- The Challenges of Diagnosing Osteoporosis - and The Limitations of Currently Available - ToolsDocument13 pagesThe Challenges of Diagnosing Osteoporosis - and The Limitations of Currently Available - ToolsJevon JavierNo ratings yet
- Osteoporosis The Evolution in DiagnosisDocument12 pagesOsteoporosis The Evolution in DiagnosisPakistan RevolutionNo ratings yet
- Drug-Induced Osteonecrosis of the Jaws: How to Diagnose, Prevent, and Treat ItFrom EverandDrug-Induced Osteonecrosis of the Jaws: How to Diagnose, Prevent, and Treat ItNo ratings yet
- Rules For Subject - Verb Agreement Are As Follows:: Boy BoyDocument37 pagesRules For Subject - Verb Agreement Are As Follows:: Boy BoyKumaresan RamalingamNo ratings yet
- 20120-Article Text-29342-1-10-20200625Document5 pages20120-Article Text-29342-1-10-20200625Min PuNo ratings yet
- 080930-Antarctica TourismDocument15 pages080930-Antarctica TourismVân PhươngNo ratings yet
- Public Space Thesis ArchitectureDocument5 pagesPublic Space Thesis Architecturestephaniejohnsonsyracuse100% (2)
- Business Analytics AssignmentDocument3 pagesBusiness Analytics AssignmentDevansh RaiNo ratings yet
- The Learners Demonstrate An Understanding of The Significance of Studying Culture, Society, and PoliticsDocument2 pagesThe Learners Demonstrate An Understanding of The Significance of Studying Culture, Society, and PoliticsMabelle BagtasosNo ratings yet
- Persuasive Essay Examples College LevelDocument9 pagesPersuasive Essay Examples College Levelafibaixzyhpqmc100% (2)
- MIJIDocument17 pagesMIJIpranilNo ratings yet
- Karachi: List of Valid Licence Holder of Banaspati (Ps:221-2003®) July 2014Document76 pagesKarachi: List of Valid Licence Holder of Banaspati (Ps:221-2003®) July 2014Okita MiraningrumNo ratings yet
- Different Modes of Agitations Era of Difference Acts & Pacts - 1st - ChapterDocument7 pagesDifferent Modes of Agitations Era of Difference Acts & Pacts - 1st - Chapterpavithra gurubaranNo ratings yet
- VollyballDocument4 pagesVollyballCristina LataganNo ratings yet
- Victor Manuel Chevere v. Jerry Johnson Stephen Kaiser Rick E. Peters Jim Keith Bob Affolter, 38 F.3d 1220, 10th Cir. (1994)Document4 pagesVictor Manuel Chevere v. Jerry Johnson Stephen Kaiser Rick E. Peters Jim Keith Bob Affolter, 38 F.3d 1220, 10th Cir. (1994)Scribd Government DocsNo ratings yet
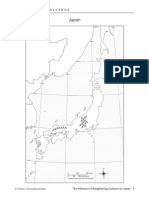
- Influence of Nieghbors On Japan Student NotebookDocument9 pagesInfluence of Nieghbors On Japan Student Notebookapi-233464494No ratings yet
- Your Contacts From TelephoneDocument73 pagesYour Contacts From TelephoneEly IEJINo ratings yet
- Subcontract Agreement (Jenesis) V.1.1Document4 pagesSubcontract Agreement (Jenesis) V.1.1sigit l.prabowoNo ratings yet
- Reasons For Decision-Appeal Judgment-Mandaya Thomas-V - The QueenDocument4 pagesReasons For Decision-Appeal Judgment-Mandaya Thomas-V - The QueenBernewsAdminNo ratings yet
- Ajax Asynchronous Javascript + XML: "A Fundamental Shift in What'S Possible On The Web"Document60 pagesAjax Asynchronous Javascript + XML: "A Fundamental Shift in What'S Possible On The Web"lucasNo ratings yet
- Function of The Criticism by TS EliotDocument18 pagesFunction of The Criticism by TS EliotRISHIKA SINHANo ratings yet
- (Lines - of - Thought - ) Robert - C. - Stalnaker-Our - Knowledge - of - The - Internal - World - (Lines - of - Thought) - Oxford - University - Press, - USA (2008) (1) by Stalnaker PDFDocument20 pages(Lines - of - Thought - ) Robert - C. - Stalnaker-Our - Knowledge - of - The - Internal - World - (Lines - of - Thought) - Oxford - University - Press, - USA (2008) (1) by Stalnaker PDFPriyanka DeNo ratings yet
- Aisc-Asd 89 PDFDocument15 pagesAisc-Asd 89 PDFKang Mas Wiralodra100% (4)
- MyDigital ID Brochure 2024Document6 pagesMyDigital ID Brochure 2024ariff29132776No ratings yet
- Ieep 104Document7 pagesIeep 104Praveen KumarpillaiNo ratings yet
- Tauck Australia Expands: WeeklyDocument3 pagesTauck Australia Expands: WeeklycruiseweeklyNo ratings yet
- Man-In-Simulant Test (MIST) For Protective EnsemblesDocument11 pagesMan-In-Simulant Test (MIST) For Protective EnsemblesAhmad Zubair RasulyNo ratings yet
- (Extra) Questões - Phrasal VerbsDocument6 pages(Extra) Questões - Phrasal VerbsRafael GomesNo ratings yet
- Emcee ScriptDocument6 pagesEmcee ScriptJasper MomoNo ratings yet
- Air Is Allowed To Flow From A Large Reservoir ThroDocument3 pagesAir Is Allowed To Flow From A Large Reservoir Throsid202pkNo ratings yet
- Third Merit List FY BMS 2021-2022 Christian Minority: Form No Denomination Name Gender Stream 12th %Document8 pagesThird Merit List FY BMS 2021-2022 Christian Minority: Form No Denomination Name Gender Stream 12th %Albin JohnNo ratings yet
- 20 Century Cases Where No Finding of Gross Immorality Was MadeDocument6 pages20 Century Cases Where No Finding of Gross Immorality Was MadeLeonel OcanaNo ratings yet