Download as docx, pdf, or txt
You might also like
- Light: The Medicine of The FutureDocument287 pagesLight: The Medicine of The FutureJekyllll100% (8)
- Fatigue NCPDocument2 pagesFatigue NCPclydell joyce masiar100% (6)
- Myocarditis NCP 2Document8 pagesMyocarditis NCP 2astro_aaron117375% (4)
- Nursing Care Plan PDFDocument6 pagesNursing Care Plan PDFEngely MercaderNo ratings yet
- Formulating A Nursing Care Plan: S++aint Paul University PhilippinesDocument7 pagesFormulating A Nursing Care Plan: S++aint Paul University Philippinesninafatima allamNo ratings yet
- Revised Kanda NCPDocument3 pagesRevised Kanda NCPhaxa yzaNo ratings yet
- Nursing Care Plan: Nikolai P. Funcion, FSUU-SNDocument5 pagesNursing Care Plan: Nikolai P. Funcion, FSUU-SNNikolai FuncionNo ratings yet
- Viii. Nursing Management Nursing Care Plan # 1 Assessment Diagnosis Planning Implementation Rationale EvaluationDocument6 pagesViii. Nursing Management Nursing Care Plan # 1 Assessment Diagnosis Planning Implementation Rationale EvaluationStar AlvarezNo ratings yet
- Acute ConDocument2 pagesAcute ConSharmaine MaNo ratings yet
- Dementia NCPDocument2 pagesDementia NCPkaloydiaz09No ratings yet
- NCP Scenario 1 FinalsDocument9 pagesNCP Scenario 1 FinalsAndrei Mackenzie AdapNo ratings yet
- Nursing Care PlanDocument6 pagesNursing Care PlanperezNo ratings yet
- NCP (Alparo, Arnold)Document3 pagesNCP (Alparo, Arnold)Shane InfanteNo ratings yet
- Yori Nicole Martine T. Cuyos: Care-Deficit-Nursing-Diagnosis-Care-PlanDocument4 pagesYori Nicole Martine T. Cuyos: Care-Deficit-Nursing-Diagnosis-Care-PlanYori Nicole Martine CuyosNo ratings yet
- NCPDocument7 pagesNCPBesael BaccolNo ratings yet
- Pioquinto (Rot 2 NCP)Document4 pagesPioquinto (Rot 2 NCP)Ghianx Carlox PioquintoxNo ratings yet
- Nursing Care Plan. CabgDocument4 pagesNursing Care Plan. CabgCecil MonteroNo ratings yet
- Assessment Nursing Diagnosis Planning Intervention Rationale EvaluationDocument5 pagesAssessment Nursing Diagnosis Planning Intervention Rationale EvaluationgianinaemilleNo ratings yet
- NoskhaDocument4 pagesNoskhanoranhassanshams0No ratings yet
- NCP For BipolarDocument11 pagesNCP For BipolarFatima Medriza DuranNo ratings yet
- NCP Template 11Document8 pagesNCP Template 11Carey Jamille YadanNo ratings yet
- Nursing Care Plan: Subjective: "I Drink Alcohol and General: Independent: Independent: Goals Met GenreralDocument3 pagesNursing Care Plan: Subjective: "I Drink Alcohol and General: Independent: Independent: Goals Met GenreralRomzy BasañesNo ratings yet
- 3 Nursing Care PlanDocument6 pages3 Nursing Care PlanJeyser T. GamutiaNo ratings yet
- Actual Nursing Care PlanDocument3 pagesActual Nursing Care PlanJinky Nacar DomingoNo ratings yet
- NURSING CARE PLAN - SuicidalactDocument4 pagesNURSING CARE PLAN - SuicidalactJennifer ArdeNo ratings yet
- Assessment Nursing Diagnosis Outcome Identification Planning Nursing Intervention Evaluation IndependentDocument7 pagesAssessment Nursing Diagnosis Outcome Identification Planning Nursing Intervention Evaluation IndependentQueenie Silva100% (1)
- NCP PsychDocument2 pagesNCP PsychMhariel Macalindong100% (1)
- NCP Group 4Document9 pagesNCP Group 4Kyle FernandezNo ratings yet
- Breast Mass Bilateral To Consider FibroadenomaDocument5 pagesBreast Mass Bilateral To Consider FibroadenomaYum CNo ratings yet
- NCP Disturbed Sleep Pattern and Hypothermia (Care of Older Adult Issues)Document4 pagesNCP Disturbed Sleep Pattern and Hypothermia (Care of Older Adult Issues)Jenny AjocNo ratings yet
- CPH 2ND WK NCPDocument5 pagesCPH 2ND WK NCPAyessa Camelle DumileNo ratings yet
- NURSINGCAREPLANDocument5 pagesNURSINGCAREPLANJulius AtencioNo ratings yet
- NCP (Final) - BipolarDocument6 pagesNCP (Final) - BipolarBel CortezNo ratings yet
- NCP Alzheimers DiseaseDocument2 pagesNCP Alzheimers DiseaseShawn TejanoNo ratings yet
- Assessmen T Diagnosi S Planning Interventions Rationale Evaluatio NDocument10 pagesAssessmen T Diagnosi S Planning Interventions Rationale Evaluatio NStephanie Villanueva AdvinculaNo ratings yet
- Nursing Care Plan For Mother:: Sno Assessment Diagnosis Planning Implementation EvaluationDocument4 pagesNursing Care Plan For Mother:: Sno Assessment Diagnosis Planning Implementation Evaluationmishti100% (1)
- My NoteDocument6 pagesMy NotePrincess Mae SabadoNo ratings yet
- NCP High RiskDocument3 pagesNCP High RiskJanelle Gift SenarloNo ratings yet
- St. Paul University PhilippinesDocument4 pagesSt. Paul University PhilippinesMia Grace GarciaNo ratings yet
- Nursing Care Plan For Patient With Musculoskeletal InjuryDocument2 pagesNursing Care Plan For Patient With Musculoskeletal Injuryoliviapalmer100% (1)
- Nursing Care Plan For Patient With Musculoskeletal InjuryDocument2 pagesNursing Care Plan For Patient With Musculoskeletal InjuryKyla ToledoNo ratings yet
- Nursing Care Plan Assesment Nursing Diagnosis Nursing Goal Nursing Intervention Rationale Actual EvaluationDocument4 pagesNursing Care Plan Assesment Nursing Diagnosis Nursing Goal Nursing Intervention Rationale Actual EvaluationFebee GeeNo ratings yet
- Assessment Diagnosis Planning Intervention Rationale EvaluationDocument4 pagesAssessment Diagnosis Planning Intervention Rationale Evaluationjay5ar5jamorabon5torNo ratings yet
- Self Care DeficitDocument2 pagesSelf Care DeficitCG Patron Bambo0% (1)
- Metch 3C NCPDocument7 pagesMetch 3C NCPEsmareldah Henry SirueNo ratings yet
- Afhto Cbti Presentation July 2021Document56 pagesAfhto Cbti Presentation July 2021tinasunxdNo ratings yet
- Self Care Deficit NCPDocument3 pagesSelf Care Deficit NCPJUSTIN ALZATENo ratings yet
- NCM 101 - Overview of Nursing ProcessDocument3 pagesNCM 101 - Overview of Nursing ProcessJohn Paul MolinaNo ratings yet
- Nursing Care Plan Cues Nursing Diagnosis Scientific Explanation Planning Implementation Scientific Rationale Evaluation Subjective CuesDocument4 pagesNursing Care Plan Cues Nursing Diagnosis Scientific Explanation Planning Implementation Scientific Rationale Evaluation Subjective Cues24 PAULINO ALDRIN MUJARNo ratings yet
- I.E (Adpie)Document4 pagesI.E (Adpie)Jayrelle D. SafranNo ratings yet
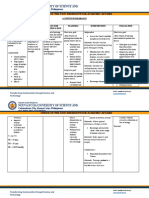
- Nueva Ecija University of Science And: O V A ADocument2 pagesNueva Ecija University of Science And: O V A AVanessa VillanuevaNo ratings yet
- Psych Vignetter VC Group 5Document20 pagesPsych Vignetter VC Group 5ErleNo ratings yet
- Textbook of Pediatric Dentistry-3rd EditionDocument18 pagesTextbook of Pediatric Dentistry-3rd EditionAnna NgNo ratings yet
- Clinical Care Plan GuideDocument13 pagesClinical Care Plan Guidej.siemens1dNo ratings yet
- Kenapa Pasien Icu Masalah Tidur PDFDocument10 pagesKenapa Pasien Icu Masalah Tidur PDFCONSTANTIUS AUGUSTONo ratings yet
- Ncps For CvaDocument14 pagesNcps For Cvalouie roderos0% (2)
- NCP Med WingDocument4 pagesNCP Med WingACOB, Jamil C.No ratings yet
- NCM 101Document8 pagesNCM 101Anna LaritaNo ratings yet
- Nursing Diagnosis - FinalDocument2 pagesNursing Diagnosis - FinalJM Mizraime Gallo Dela-peñaNo ratings yet
- Health Assessment PrelimsDocument21 pagesHealth Assessment PrelimsIvan MaximusNo ratings yet
- General Principles and Empirically Supported Techniques of Cognitive Behavior TherapyFrom EverandGeneral Principles and Empirically Supported Techniques of Cognitive Behavior TherapyNo ratings yet
- Adult Day Care Center PDFDocument64 pagesAdult Day Care Center PDFFlorencia Medina100% (2)
- The Journal of The Royal Society For The Promotion of Health-2004-Chamberlain-284-6Document4 pagesThe Journal of The Royal Society For The Promotion of Health-2004-Chamberlain-284-6mauricioelvis100% (1)
- Community Health Nursing IntroductionDocument3 pagesCommunity Health Nursing IntroductionBianca Denise RopilaNo ratings yet
- Complementary Feeding HambantotaDocument39 pagesComplementary Feeding Hambantotasampath muthunayakeNo ratings yet
- Nursing AssessmentDocument32 pagesNursing AssessmentKang RezzaNo ratings yet
- Nitsbin I Medicine 2nd Edition Final Revised 1Document1,682 pagesNitsbin I Medicine 2nd Edition Final Revised 1Dawit g/kidanNo ratings yet
- CPG Management of ThalassaemiaDocument100 pagesCPG Management of Thalassaemiamrace_amNo ratings yet
- Basic Life Support in Infants and ChildrenDocument9 pagesBasic Life Support in Infants and ChildrenMelissa Espinoza PeñaNo ratings yet
- Sars-Cov-2/Covid-19 Test Report: Amendments / CorrectionsDocument1 pageSars-Cov-2/Covid-19 Test Report: Amendments / CorrectionsSebastian PradaNo ratings yet
- ADNICDocument2 pagesADNICTRTNo ratings yet
- Flyer PIT IDI Bandung LINKDocument1 pageFlyer PIT IDI Bandung LINKBabo SanNo ratings yet
- BrochureDocument1 pageBrochureSa Rah Kamad DagendelNo ratings yet
- Medip, IJRMS-7730 ODocument6 pagesMedip, IJRMS-7730 OsundarcetNo ratings yet
- Health Care Waste Managementan Advocacypaper For Final RevisionDocument62 pagesHealth Care Waste Managementan Advocacypaper For Final RevisionNikki BarenaNo ratings yet
- Shahdevinandar, JPHV 2241 PUBLISHDocument6 pagesShahdevinandar, JPHV 2241 PUBLISHGinanjar Putri SariNo ratings yet
- Definition of Medical TreatmentDocument2 pagesDefinition of Medical Treatmentfikadu100% (1)
- Ashley Holmquist: Shawn and Michaela Cielinski, Buckman MN - NannyDocument2 pagesAshley Holmquist: Shawn and Michaela Cielinski, Buckman MN - Nannyapi-545556079No ratings yet
- Las Health-6 q4 WK 4-8 R. PolvorizaDocument7 pagesLas Health-6 q4 WK 4-8 R. PolvorizaANGELINA RAMBOYONGNo ratings yet
- Case StudyDocument3 pagesCase StudySandeepNagarkotiNo ratings yet
- BSCN Collaborative Program - Year 1: Registration Tip Sheet 2021-2022Document1 pageBSCN Collaborative Program - Year 1: Registration Tip Sheet 2021-2022Ryan Christian PatriarcaNo ratings yet
- Funda LabDocument4 pagesFunda LabEmily BernatNo ratings yet
- Jurnal Kanker Mamae-Survival Life Penderita Kanker Payudara Pada WanitaDocument7 pagesJurnal Kanker Mamae-Survival Life Penderita Kanker Payudara Pada WanitarosmawatiNo ratings yet
- Voluson E8: Advanced Features Simplified WorkflowDocument3 pagesVoluson E8: Advanced Features Simplified WorkflowRirin Dwi LestariNo ratings yet
- Assessment of Disability & CompensationDocument79 pagesAssessment of Disability & CompensationPrasannaKadethotaNo ratings yet
- Anjali Bhure, Neelakshi Kalita, Prasad Ingley, C.P. Gadkari: Research ArticleDocument5 pagesAnjali Bhure, Neelakshi Kalita, Prasad Ingley, C.P. Gadkari: Research ArticleTedja PrakosoNo ratings yet
- Cervical Cancer StagingDocument3 pagesCervical Cancer StagingMeka Medina RahmanNo ratings yet
- Ashoka Medicover OMDocument7 pagesAshoka Medicover OMnobleboy99No ratings yet
- The Medical City ClarkDocument16 pagesThe Medical City ClarkPaopao Bacaling0% (1)
- A Proven Pathway To AccreditationDocument25 pagesA Proven Pathway To AccreditationkukunNo ratings yet