Download as pdf or txt
You might also like
- Textbook of Cardiovascular Medicine in Dogs and Cats (VetBooks - Ir)Document1,112 pagesTextbook of Cardiovascular Medicine in Dogs and Cats (VetBooks - Ir)Jonathan Mann100% (1)
- Aspira Drainage System FamiliarizationDocument11 pagesAspira Drainage System FamiliarizationChad BensonNo ratings yet
- Active Cycle Breathing TechniqueDocument20 pagesActive Cycle Breathing TechniqueRAM100% (2)
- Navigating The Pandemic Response Life Cycle: Molecular Diagnostics and Immunoassays in The Context of COVID-19 ManagementDocument19 pagesNavigating The Pandemic Response Life Cycle: Molecular Diagnostics and Immunoassays in The Context of COVID-19 ManagementdebasreenitaNo ratings yet
- 10 1378@chest 123 5 1615Document10 pages10 1378@chest 123 5 1615SAYBLUs FANSNo ratings yet
- Update On AntiretroviralDocument15 pagesUpdate On AntiretroviralAndrea LunaNo ratings yet
- Antibiotico YPronosticoDocument6 pagesAntibiotico YPronosticoagonzale52No ratings yet
- DescargarDocument14 pagesDescargarDelia JMNo ratings yet
- 1 s2.0 S2666524721001154 MainDocument1 page1 s2.0 S2666524721001154 MainAnita DewiNo ratings yet
- Infections of The Spine and Spinal Cord: Continuumaudio Interviewavailable OnlineDocument34 pagesInfections of The Spine and Spinal Cord: Continuumaudio Interviewavailable OnlineYeimy Celis TorresNo ratings yet
- Anantapreecha Et Al 2020 Development of A Pseudotyped Lentiviral Vector Based Neutralization Assay For ChikungunyaDocument7 pagesAnantapreecha Et Al 2020 Development of A Pseudotyped Lentiviral Vector Based Neutralization Assay For ChikungunyaNurshariza AbdullahNo ratings yet
- Cytokines Article Newsletter Poster RecentDocument2 pagesCytokines Article Newsletter Poster RecentVohn Archie EdjanNo ratings yet
- Therapeutic Apheresis in COVID 19Document4 pagesTherapeutic Apheresis in COVID 19Lawrence LauNo ratings yet
- Jamainternal Sun 2021 Oi 210075 1643648297.88061Document10 pagesJamainternal Sun 2021 Oi 210075 1643648297.88061Leidy Nayerli Garcia RodriguezNo ratings yet
- Ijms 24 00169Document15 pagesIjms 24 00169Catherine BasinNo ratings yet
- Journal PNTD 0012035Document8 pagesJournal PNTD 0012035ALLAN COSTA GOMESNo ratings yet
- TreatmentOIGESIDA 2008, NoDocument24 pagesTreatmentOIGESIDA 2008, NoDra Carolina Escalante Neurologa de AdultosNo ratings yet
- Laboratory Diagnosis of Virus DiseasesDocument21 pagesLaboratory Diagnosis of Virus DiseasesVictor CostaNo ratings yet
- Understanding COVID-19 Vaccines and Immunity: Enhanced CPD DO CDocument4 pagesUnderstanding COVID-19 Vaccines and Immunity: Enhanced CPD DO CDevin KwanNo ratings yet
- Impact of Time To Antibiotic Therapy On Clinical Outcome I 2021 Clinical MicDocument7 pagesImpact of Time To Antibiotic Therapy On Clinical Outcome I 2021 Clinical MicSusanyi ErvinNo ratings yet
- 555 FullDocument11 pages555 FullDra Sandra VèlezNo ratings yet
- 7 (2) - Aboul Naga-2022-Behçet Uveitis - Current PracticeDocument16 pages7 (2) - Aboul Naga-2022-Behçet Uveitis - Current Practicekueiying.suNo ratings yet
- Jamadermatol 2020 0013Document2 pagesJamadermatol 2020 0013Mostafa SalahNo ratings yet
- HIV-Immune-Reconstitution-Inflammatory-Syndrome-In VIH-InfectedDocument16 pagesHIV-Immune-Reconstitution-Inflammatory-Syndrome-In VIH-InfectedkarlosNo ratings yet
- The Evidence Supporting The Revised EORTC-MSGERC Definitions For Invasive Fungal InfectionsDocument2 pagesThe Evidence Supporting The Revised EORTC-MSGERC Definitions For Invasive Fungal Infectionsgwyneth.green.512No ratings yet
- Medical Hypotheses: SciencedirectDocument9 pagesMedical Hypotheses: SciencedirectOanaDavidNo ratings yet
- A Report On The US Vaccine Adverse Events Reporting System (VAERS) J. Rose P. McculloghDocument22 pagesA Report On The US Vaccine Adverse Events Reporting System (VAERS) J. Rose P. Mcculloghnasarmannan100% (3)
- Iris CidDocument7 pagesIris CidDaniel ErasoNo ratings yet
- Aspergilosis InvasivoDocument13 pagesAspergilosis InvasivoVeronica ZendejasNo ratings yet
- Covid-19 mRNA VaccinesDocument16 pagesCovid-19 mRNA VaccinesSargent Goodchild100% (2)
- 2021 - Vaccines and Antivirals Grand Challenges and Great OpportunitiesDocument8 pages2021 - Vaccines and Antivirals Grand Challenges and Great OpportunitiesMaykol Hernán Rojas SánchezNo ratings yet
- A Comprehensive Insight On The Challenges For COVID-19 vaccine-ScienceDirectDocument14 pagesA Comprehensive Insight On The Challenges For COVID-19 vaccine-ScienceDirectGaspar PonceNo ratings yet
- COVID 19 Influences Lung Microbiota Dynamics and Favors The 2021 Journal ofDocument3 pagesCOVID 19 Influences Lung Microbiota Dynamics and Favors The 2021 Journal ofJosé Carlos Bernaola ZevallosNo ratings yet
- 2021 Article 1347Document6 pages2021 Article 1347Rocio Ayaque AguirreNo ratings yet
- Drug Repositioning For Hand, Foot, and Mouth DiseaseDocument19 pagesDrug Repositioning For Hand, Foot, and Mouth DiseaseJuliethNo ratings yet
- IVIg For The Treatment of COVID 19Document3 pagesIVIg For The Treatment of COVID 19lalaine nadulpitNo ratings yet
- A Strategic Approach To COVID-19 Vaccine R&D: Lawrence Corey, John R. Mascola, Anthony S. Fauci, Francis S. CollinsDocument6 pagesA Strategic Approach To COVID-19 Vaccine R&D: Lawrence Corey, John R. Mascola, Anthony S. Fauci, Francis S. CollinsGrace AngelinaNo ratings yet
- Covid Vaccine Nov 2020Document13 pagesCovid Vaccine Nov 2020Office EPHNo ratings yet
- Hepatitis CDocument11 pagesHepatitis CBety Puma PauccaraNo ratings yet
- Ivermectin: A Systematic Review From Antiviral Effects To COVID-19 Complementary RegimenDocument10 pagesIvermectin: A Systematic Review From Antiviral Effects To COVID-19 Complementary Regimenwn6ejrNo ratings yet
- La Ivermectina No Previene La Hospitalización Por Coronavirus, Según EstudioDocument11 pagesLa Ivermectina No Previene La Hospitalización Por Coronavirus, Según EstudioEl Informador Santa MartaNo ratings yet
- Science Journals — AAAS - Haynes-2020-Prospects-for-a-safe-COVID-19-vaccineDocument13 pagesScience Journals — AAAS - Haynes-2020-Prospects-for-a-safe-COVID-19-vaccinerahiteshewNo ratings yet
- Fimmu 13 782198Document11 pagesFimmu 13 782198Suryati HusinNo ratings yet
- Tion at December 2021Document10 pagesTion at December 2021roquessudeNo ratings yet
- Toxicology ReportsDocument11 pagesToxicology ReportsMarcio HenriquesNo ratings yet
- Microorganisms 09 01773Document14 pagesMicroorganisms 09 01773AnhNo ratings yet
- A Clinical Review of Viral HepatitisDocument6 pagesA Clinical Review of Viral HepatitisPAULA JULIANA PARRA PRADANo ratings yet
- Old and New Vaccine Approaches: Ruth Arnon, Tamar Ben-YedidiaDocument10 pagesOld and New Vaccine Approaches: Ruth Arnon, Tamar Ben-YedidiahansmeetNo ratings yet
- Antibiotecoterapia en SepsisDocument13 pagesAntibiotecoterapia en SepsisJuan Pablo Arteaga VargasNo ratings yet
- COVID-19 Vaccination Efficacy and Safety Literature Review: ArticleDocument19 pagesCOVID-19 Vaccination Efficacy and Safety Literature Review: ArticlePromiseNo ratings yet
- 1 s2.0 S2213219822000228 MainDocument9 pages1 s2.0 S2213219822000228 MainEducation serviceNo ratings yet
- NIH Public Access: Author ManuscriptDocument23 pagesNIH Public Access: Author ManuscriptntnquynhproNo ratings yet
- Main PDFDocument12 pagesMain PDFLuz Betty Alejo MamaniNo ratings yet
- Antibiotico en SepsisDocument13 pagesAntibiotico en Sepsismaomed2014No ratings yet
- B.Pharm. Industrial Training Daily ReportDocument12 pagesB.Pharm. Industrial Training Daily ReportSanya misraNo ratings yet
- Jiaa 221Document13 pagesJiaa 221AndradaLavricNo ratings yet
- Assessing Risk For Chronic Disorders Caused by Human Papillomavirus Vaccines and Mrna Covid 19 VaccinesDocument6 pagesAssessing Risk For Chronic Disorders Caused by Human Papillomavirus Vaccines and Mrna Covid 19 VaccinesHerald Scholarly Open AccessNo ratings yet
- International Journal of Infectious Diseases: SciencedirectDocument10 pagesInternational Journal of Infectious Diseases: Sciencedirectbe a doctor for you Medical studentNo ratings yet
- Artikel VaksinDocument9 pagesArtikel VaksinrajyurafNo ratings yet
- Protein Subunits VaccineDocument14 pagesProtein Subunits Vaccineahmed 9No ratings yet
- 142-Texto Do Artigo-230-1-10-20200403Document16 pages142-Texto Do Artigo-230-1-10-20200403Celiane de FariasNo ratings yet
- Biomedicine & Pharmacotherapy: SciencedirectDocument10 pagesBiomedicine & Pharmacotherapy: SciencedirectCamilo Andrés CastroNo ratings yet
- Flange Bolt Torque Sequence and Torque Table - A Complete Bolt Tightening ProcedureDocument34 pagesFlange Bolt Torque Sequence and Torque Table - A Complete Bolt Tightening ProcedureHoussemSoltanaNo ratings yet
- NAWPPL-BIMSAUR-NPPL-000-EL-ITP-00001 - 001 - Procurement Inspection Test PlanDocument14 pagesNAWPPL-BIMSAUR-NPPL-000-EL-ITP-00001 - 001 - Procurement Inspection Test PlanHoussemSoltanaNo ratings yet
- Nawppl-Bimssil-Nppl-000 - Qc-Itp-00001-000Document9 pagesNawppl-Bimssil-Nppl-000 - Qc-Itp-00001-000HoussemSoltanaNo ratings yet
- NAWPPL-BIMSVAL-NPPL-000-QC-ITP-00002-002 - INSPECTION AND TEST PLAN - ActuatorsDocument11 pagesNAWPPL-BIMSVAL-NPPL-000-QC-ITP-00002-002 - INSPECTION AND TEST PLAN - ActuatorsHoussemSoltanaNo ratings yet
- 4:: TTRZS: Ilef8CljDocument9 pages4:: TTRZS: Ilef8CljHoussemSoltanaNo ratings yet
- NAWPPL-BIMSVAL-NPPL-000-QC-ITP-00200 - 002 - QUALITY PLAN (Incl. Inspection and Test Plan) FOR GLOBE & CHECK VALVESDocument10 pagesNAWPPL-BIMSVAL-NPPL-000-QC-ITP-00200 - 002 - QUALITY PLAN (Incl. Inspection and Test Plan) FOR GLOBE & CHECK VALVESHoussemSoltanaNo ratings yet
- WC BPR - Prevention and Management of Burns 1791r3e FinalDocument68 pagesWC BPR - Prevention and Management of Burns 1791r3e FinalSiti ChodijahNo ratings yet
- 512 vPEP HC IFU PN 352rev07.1 Webview Version 1Document2 pages512 vPEP HC IFU PN 352rev07.1 Webview Version 1Nandhini SivakumarNo ratings yet
- Ewc PreviousDocument3 pagesEwc PreviousUzir RashidinNo ratings yet
- Human Anatomy Chapter 26Document10 pagesHuman Anatomy Chapter 26jinni0926No ratings yet
- Immaculate Heart of Mary Academy Long Test in Music 7Document6 pagesImmaculate Heart of Mary Academy Long Test in Music 7Cryzel MuniNo ratings yet
- Ultrasound-Guided Nerve Blocks in The Head and Neck For Chronic Pain Management - The Anatomy, Sonoanatomy, and ProcedureDocument16 pagesUltrasound-Guided Nerve Blocks in The Head and Neck For Chronic Pain Management - The Anatomy, Sonoanatomy, and Proceduremarcus moraisNo ratings yet
- Definition and Staging of Chronic Kidney Disease in Adults - UpToDateDocument1 pageDefinition and Staging of Chronic Kidney Disease in Adults - UpToDateLauraNo ratings yet
- GC Geria ToolDocument16 pagesGC Geria ToolRomelyn OrdillasNo ratings yet
- Medical Ionization: Iontophoresis DR - Saira DDocument22 pagesMedical Ionization: Iontophoresis DR - Saira DAnonymous -No ratings yet
- Soal Dan Pembahasan Bahasa InggrisDocument2 pagesSoal Dan Pembahasan Bahasa Inggrislintang wNo ratings yet
- Diabetes Educacion Manual AfricaDocument238 pagesDiabetes Educacion Manual AfricaPsico AstralNo ratings yet
- Anestesia e Esclerose TuberosaDocument5 pagesAnestesia e Esclerose TuberosaMarina MelekNo ratings yet
- Urticaria LesionsDocument9 pagesUrticaria LesionsluckyNo ratings yet
- Medical Surgical NursingDocument6 pagesMedical Surgical NursingHCX dghhq100% (2)
- Vulvovaginitis in Kids - Symptoms, Causes, and TreatmentDocument1 pageVulvovaginitis in Kids - Symptoms, Causes, and TreatmentHabtamu tamiruNo ratings yet
- Notification MMRCL Various Vacancy PostsDocument14 pagesNotification MMRCL Various Vacancy PostsabhishekNo ratings yet
- Biosafety Levels: Primary ContainmentDocument8 pagesBiosafety Levels: Primary ContainmentAbeer FatimaNo ratings yet
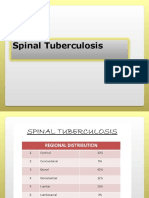
- Spinal TuberculosisDocument54 pagesSpinal TuberculosisGagandeep YadavNo ratings yet
- MonsantoDocument1 pageMonsantoAmerican English CourseNo ratings yet
- My Basal GangliaDocument18 pagesMy Basal GangliaPriya GKNo ratings yet
- Eyal Herzog (Editor) - Pulmonary Embolism-Springer (2021)Document288 pagesEyal Herzog (Editor) - Pulmonary Embolism-Springer (2021)Frederico PóvoaNo ratings yet
- Giamberardino Referred Muscle Pain and Hyperalgesia From VisceraDocument6 pagesGiamberardino Referred Muscle Pain and Hyperalgesia From ViscerapartecipazionilsNo ratings yet
- Bone BiopsyDocument3 pagesBone BiopsySophia A. GoNo ratings yet
- Acute Infections During PregnancyDocument63 pagesAcute Infections During PregnancyHussein AliNo ratings yet
- Recurrent SnezzingDocument7 pagesRecurrent Snezzingrahulsinghroy17025No ratings yet
- Cvs2-k1 (JP-PJB Pada Dewasa)Document81 pagesCvs2-k1 (JP-PJB Pada Dewasa)32 sebastian Josia N.No ratings yet
- Different Plants DescriptionDocument55 pagesDifferent Plants DescriptionPushkar ChoudharyNo ratings yet