Download as pdf or txt
You might also like
- BODYPUMP 127 BODYPUMP127ChoreographyNotes Row en App Print PDFDocument45 pagesBODYPUMP 127 BODYPUMP127ChoreographyNotes Row en App Print PDFJavier Alonso NiñoNo ratings yet
- Optimal Shoulder Performance - Cressey ReinoldDocument40 pagesOptimal Shoulder Performance - Cressey ReinoldPricope Madalina93% (14)
- 092377-190708 ATTUNE Knee Ordering Info 0Document45 pages092377-190708 ATTUNE Knee Ordering Info 0Elianna SilvaNo ratings yet
- Prometric Questions OrthoDocument13 pagesPrometric Questions OrthoFaisal Mushtaq67% (12)
- Netter Atlas UL ChartsDocument4 pagesNetter Atlas UL ChartsJUSASB100% (1)
- Knee Tibia & Ankle InjuriesDocument88 pagesKnee Tibia & Ankle InjuriesNasser AlQadhibNo ratings yet
- Shoulder InjuriesDocument33 pagesShoulder InjuriesWizz Háķìm ĻêşòwNo ratings yet
- Emergency Ortho BCS 2017Document80 pagesEmergency Ortho BCS 2017Priza Razunip100% (1)
- Injury Around The Elbow: Mohamad Afiq Izzuddin 1001336000 Group 3Document51 pagesInjury Around The Elbow: Mohamad Afiq Izzuddin 1001336000 Group 3Star CruiseNo ratings yet
- Bartoszewski 2018Document2 pagesBartoszewski 2018Tri YulihartiNo ratings yet
- Distal Phalanx (45%) - Metacarpal (30%) - Proximal Phalanx (15%) - Middle Phalanx (10%)Document40 pagesDistal Phalanx (45%) - Metacarpal (30%) - Proximal Phalanx (15%) - Middle Phalanx (10%)Dabessa MosissaNo ratings yet
- Scapula FracturesDocument24 pagesScapula FracturesFrancesco BenazzoNo ratings yet
- ClaviculaDocument24 pagesClaviculaoktavia indahNo ratings yet
- Fractures HFHDocument74 pagesFractures HFHEmmanuel Papa AcquahNo ratings yet
- 7 Injuries of Upper Arm and ElbowDocument75 pages7 Injuries of Upper Arm and Elbowwissam salimNo ratings yet
- Elbow Injuries: DR R B Kalia, Additional Professor Department of OrthopaedicsDocument57 pagesElbow Injuries: DR R B Kalia, Additional Professor Department of OrthopaedicsHajar AlSaediNo ratings yet
- Clay Shoveler's FractureDocument26 pagesClay Shoveler's FracturerineeshNo ratings yet
- Fracture Shaft Humerus - 030014Document60 pagesFracture Shaft Humerus - 030014MohammedShahidNo ratings yet
- Fraktur ClaviculaDocument23 pagesFraktur ClaviculaayuradityoNo ratings yet
- Case ReportDocument57 pagesCase ReportlmandahaNo ratings yet
- Supracondylarfracture PDFDocument40 pagesSupracondylarfracture PDFSurya AbigamikaNo ratings yet
- Orthopedics and Surgery of The Hand and WristDocument157 pagesOrthopedics and Surgery of The Hand and Wristhemasunder903No ratings yet
- Orthopedics Condensed MaterialDocument13 pagesOrthopedics Condensed Materialhznknzbwk7No ratings yet
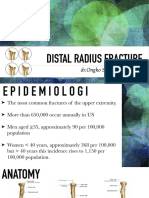
- Distal Radius FractureDocument28 pagesDistal Radius FractureOngko SetunggalNo ratings yet
- Colle's and Smith's Fracture: Prepared by Ali Nassser Supervised by DR - Ali TahaDocument29 pagesColle's and Smith's Fracture: Prepared by Ali Nassser Supervised by DR - Ali Tahaali laftaNo ratings yet
- Fractures of Forearm: Oktya Veny Simbolon Pattiyah Prehandini AyuningtyasDocument90 pagesFractures of Forearm: Oktya Veny Simbolon Pattiyah Prehandini AyuningtyaspattiyahNo ratings yet
- Shoulder Impingement SyndromeDocument29 pagesShoulder Impingement SyndromeindunksNo ratings yet
- Coronoid FractureDocument38 pagesCoronoid FractureRamin MaharjanNo ratings yet
- Colle's FractureDocument7 pagesColle's FracturemadheswariNo ratings yet
- U10-Distal Radius FracturesDocument121 pagesU10-Distal Radius Fracturesrajasekhar ANo ratings yet
- Fraktur Colles Dan SmithDocument29 pagesFraktur Colles Dan SmithWara Permeswari Wardhani100% (1)
- Clavicle AC SC JointsDocument97 pagesClavicle AC SC Jointsdr.maulanahutabaratNo ratings yet
- Galeazzi FractureDocument37 pagesGaleazzi FractureRamin MaharjanNo ratings yet
- Ortho Fraktur 1/3 Proximal Humerus DextraDocument57 pagesOrtho Fraktur 1/3 Proximal Humerus DextraFian ChristoNo ratings yet
- Dens FractureDocument4 pagesDens FracturepuchioNo ratings yet
- 18 Rosenwasser Distal Radius Fractures HandoutDocument13 pages18 Rosenwasser Distal Radius Fractures HandoutAzmi FarhadiNo ratings yet
- Distal Radius and UlnaDocument40 pagesDistal Radius and UlnaDia CembranoNo ratings yet
- Forearm Fractures: Derek J. Donegan, M.D. University of PennsylvaniaDocument55 pagesForearm Fractures: Derek J. Donegan, M.D. University of PennsylvaniaSherly DesnitaNo ratings yet
- Fracture Distal Humerus (Surgical Anatomy, Classification and Treatment)Document98 pagesFracture Distal Humerus (Surgical Anatomy, Classification and Treatment)drakkashmiri100% (4)
- Distal Radial Injury: Department of Orthopaedics SGH Didactic LectureDocument52 pagesDistal Radial Injury: Department of Orthopaedics SGH Didactic Lecturedrscribd1No ratings yet
- (Ortho) Pemeriksaan Dan Kegawatan Bedah OrthopediDocument59 pages(Ortho) Pemeriksaan Dan Kegawatan Bedah OrthopediclarestaNo ratings yet
- Musculoskeletal Trauma Cases in Lower Extremities and Its ManagementDocument41 pagesMusculoskeletal Trauma Cases in Lower Extremities and Its ManagementAli AbdullahNo ratings yet
- Fractures of The Lower LimbDocument50 pagesFractures of The Lower LimbVishwajit Hegde100% (1)
- Paediatric Elbow TraumaDocument59 pagesPaediatric Elbow TraumaJoel ChongNo ratings yet
- Hip FracturesDocument74 pagesHip FracturesMina SamirNo ratings yet
- Imaging of Atlanto-Occipital and Atlantoaxial Traumatic InjuriesDocument43 pagesImaging of Atlanto-Occipital and Atlantoaxial Traumatic InjuriesMaroofAliNo ratings yet
- Musculoskeletal TraumaDocument33 pagesMusculoskeletal TraumaMario RodriguezNo ratings yet
- Distal End Humerus Fractures: BY:-Dr. Anshu Sharma Guide:-Dr.A.K. MathurDocument76 pagesDistal End Humerus Fractures: BY:-Dr. Anshu Sharma Guide:-Dr.A.K. MathurToàn Đặng Phan VĩnhNo ratings yet
- Supracondylar FractureDocument53 pagesSupracondylar Fracturedesire kbpNo ratings yet
- Blue Writing Is What I Added To These Notes: RadiographyDocument46 pagesBlue Writing Is What I Added To These Notes: Radiographybjpalmer100% (2)
- AC JointDocument29 pagesAC JointMuhammad Muttaqee MisranNo ratings yet
- Scaphoid FractureDocument77 pagesScaphoid FractureTanuGarg100% (1)
- AO Trauma Vol.2Document100 pagesAO Trauma Vol.2Cujba GheorgheNo ratings yet
- Distal Radial FractureDocument40 pagesDistal Radial Fractureanhhoangdr81No ratings yet
- Injuries Around The ShoulderDocument81 pagesInjuries Around The ShoulderMisoNo ratings yet
- SC - Fracture ZMHDocument51 pagesSC - Fracture ZMHMis StromNo ratings yet
- Dis EctomyDocument10 pagesDis EctomyNicholas ChenNo ratings yet
- Common Orthopedic Emergency Conditions and Their ManagementDocument6 pagesCommon Orthopedic Emergency Conditions and Their ManagementDhruva PatelNo ratings yet
- Distal Humerus Fracture: Presentor:Dr Balaji Vinayaka Mission Kirubananda Variyar Medical College. SalemDocument48 pagesDistal Humerus Fracture: Presentor:Dr Balaji Vinayaka Mission Kirubananda Variyar Medical College. SalemNicholas DelaliNo ratings yet
- Upload Scribd 4Document7 pagesUpload Scribd 4Yoga AninditaNo ratings yet
- Spine FractureDocument72 pagesSpine Fracturevatil62891No ratings yet
- Elbow and Shoulder Dislocation InjuriesDocument42 pagesElbow and Shoulder Dislocation InjuriesWizz Háķìm ĻêşòwNo ratings yet
- Apley 24Document16 pagesApley 24Muhammad DzulfikarNo ratings yet
- Penanganan FrakturDocument78 pagesPenanganan FrakturelizabethmargarethNo ratings yet
- Acromioclavicular Joint Injury, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsFrom EverandAcromioclavicular Joint Injury, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsNo ratings yet
- Varus Knee Classification and CorrectionDocument8 pagesVarus Knee Classification and CorrectionPraharshaNo ratings yet
- 10 Weeks To Fit Program Calendar ScheduleDocument4 pages10 Weeks To Fit Program Calendar ScheduleAnita KokaNo ratings yet
- Biomechanics and Pathomechanics of Elbow JointDocument44 pagesBiomechanics and Pathomechanics of Elbow JointAshwini BajajNo ratings yet
- 10th Lec Muscles Posterior of ForearmDocument16 pages10th Lec Muscles Posterior of ForearmMudasir razaNo ratings yet
- Self Massage Therapy Guide - Physix Gear Sport PDFDocument25 pagesSelf Massage Therapy Guide - Physix Gear Sport PDFAlexandria Trahan100% (1)
- 03 Quadrangular and Triangular SpacesDocument2 pages03 Quadrangular and Triangular Spacesطه طارقNo ratings yet
- Chapter 18Document182 pagesChapter 18ryllerylle05No ratings yet
- Scapula DyskinesiaDocument5 pagesScapula Dyskinesiamiguelax1No ratings yet
- Dops Rom PasifDocument5 pagesDops Rom Pasifmutia aNo ratings yet
- Muscles Covered in The Trigger Point ChartsDocument19 pagesMuscles Covered in The Trigger Point ChartsSaninan Mat100% (5)
- Anatomical Shoulder Fracture System Surgical Technique PDFDocument24 pagesAnatomical Shoulder Fracture System Surgical Technique PDFAdrian TudorNo ratings yet
- Kinetic Chain ArticleDocument9 pagesKinetic Chain Articler.zaczek93No ratings yet
- Total Knee Replacement Brochure PDFDocument2 pagesTotal Knee Replacement Brochure PDFapi-260874114No ratings yet
- Muscles of The Upper Limb Muscles of The Back Superficial Back Proximal Distal Action InnervationDocument7 pagesMuscles of The Upper Limb Muscles of The Back Superficial Back Proximal Distal Action InnervationKris GulleyNo ratings yet
- Noise Around The KneeDocument8 pagesNoise Around The KneeAbraham SaldañaNo ratings yet
- Can Vastus Medialis Oblique Be Preferentially ActivatedDocument30 pagesCan Vastus Medialis Oblique Be Preferentially ActivatedGorkaBuesaNo ratings yet
- Biomechanics of The Knee: Tibiofemoral JointDocument7 pagesBiomechanics of The Knee: Tibiofemoral JointManuel Azael Rodríguez CigalaNo ratings yet
- Saint Francis of Assisi College School of Nursing Performance Checklist For Range of Motion (Rom)Document5 pagesSaint Francis of Assisi College School of Nursing Performance Checklist For Range of Motion (Rom)Carol Neng CalupitanNo ratings yet
- Shoulder Impingement SyndromeDocument37 pagesShoulder Impingement SyndromeDADDYGUS100% (1)
- 3-Women Athletes Knee Injuries - 2005Document9 pages3-Women Athletes Knee Injuries - 2005Fernanda CarvalhoNo ratings yet
- Manual/Assisted Stretching Techniques: WWW - Fisiokinesiterapia.bizDocument26 pagesManual/Assisted Stretching Techniques: WWW - Fisiokinesiterapia.bizLuca AnamariaNo ratings yet
- Open and Closed Packed Positions of JointsDocument1 pageOpen and Closed Packed Positions of JointsRaymond100% (4)
- Monteggia FractureDocument29 pagesMonteggia Fracture'-dooublleaiienn Itouehh IinNo ratings yet
- Rodrigo Py Gonçalves Barreto Bilateral MagneticDocument8 pagesRodrigo Py Gonçalves Barreto Bilateral MagneticfilipecorsairNo ratings yet
- Manual Muscle Testing of The Shoulder: PHTH 224Document97 pagesManual Muscle Testing of The Shoulder: PHTH 224Meet ShahNo ratings yet