Download as pdf or txt
You might also like
- EC Camp Management PlanDocument4 pagesEC Camp Management PlanJelyn Bujatin100% (18)
- Reading Part A Hip FracturesDocument6 pagesReading Part A Hip Fracturesfernanda1rondelliNo ratings yet
- Operations & Maintenance Handbook - LPG Storage Facilities (Propane Research Council)Document176 pagesOperations & Maintenance Handbook - LPG Storage Facilities (Propane Research Council)KannanGKNo ratings yet
- Epidemiology of OsteoporosisDocument1 pageEpidemiology of OsteoporosisJubaer AlamNo ratings yet
- Osteoporotic Vertebral Compression Fractures and VDocument13 pagesOsteoporotic Vertebral Compression Fractures and VChristopherLawrenceNo ratings yet
- Reviews: Geographic and Ethnic Disparities in Osteoporotic FracturesDocument14 pagesReviews: Geographic and Ethnic Disparities in Osteoporotic Fracturesdeepdreamx6400No ratings yet
- Nickolas 2008Document11 pagesNickolas 2008gamalramadiNo ratings yet
- Public Health Nut8Document17 pagesPublic Health Nut8Fiki FerindraNo ratings yet
- Orthopedic MedicineDocument13 pagesOrthopedic MedicineAnonymous kdBDppigENo ratings yet
- Div Class Title Diet Nutrition and The Prevention of Osteoporosis DivDocument17 pagesDiv Class Title Diet Nutrition and The Prevention of Osteoporosis DivLucas Oliveira MouraNo ratings yet
- VARICELLA Patofisiologi RefratDocument10 pagesVARICELLA Patofisiologi RefrattrisnaningsiNo ratings yet
- Effectiveness of Structured Teaching Programme On Knowledge Regarding Osteoporosis and Its Management Among Menopausal WomenDocument12 pagesEffectiveness of Structured Teaching Programme On Knowledge Regarding Osteoporosis and Its Management Among Menopausal WomenEditor IJTSRDNo ratings yet
- CGJ 18 29 PDFDocument6 pagesCGJ 18 29 PDFZenithaMeidaNo ratings yet
- The Pharmacological Management of OsteoporosisDocument6 pagesThe Pharmacological Management of Osteoporosisarber mulolliNo ratings yet
- Osteoporosis: Epidemiology, Diagnosis, and TreatmentDocument4 pagesOsteoporosis: Epidemiology, Diagnosis, and TreatmentPeach Amparo BuguinaNo ratings yet
- Vertebral Compression Fractures: A Review of Current Management and Multimodal TherapyDocument17 pagesVertebral Compression Fractures: A Review of Current Management and Multimodal TherapyFatimah AssagafNo ratings yet
- Osteoporosis: Disease SummaryDocument10 pagesOsteoporosis: Disease SummaryHohai ConcepcionNo ratings yet
- 2014 OsteoporosisInMen ThematicReport EnglishDocument24 pages2014 OsteoporosisInMen ThematicReport EnglishTatia TsnobiladzeNo ratings yet
- Wagner2015 Article FragilityFracturesOfTheSacrumHDocument14 pagesWagner2015 Article FragilityFracturesOfTheSacrumHSandy DaengNo ratings yet
- Overview of Epidemiology: Rockwood & Green's Fractures in Adults, 6th EditionDocument53 pagesOverview of Epidemiology: Rockwood & Green's Fractures in Adults, 6th EditionSilvia TacheNo ratings yet
- Osteoporosis: Screening, Prevention, and ManagementDocument20 pagesOsteoporosis: Screening, Prevention, and ManagementBernardo RomeroNo ratings yet
- Vertebralfracture: James F. Griffith,, Giuseppe GuglielmiDocument11 pagesVertebralfracture: James F. Griffith,, Giuseppe GuglielmiNiningRahmaNo ratings yet
- 3.osteoporosis Fragility FXDocument7 pages3.osteoporosis Fragility FXThanawat SimaNo ratings yet
- OsteopeniaDocument9 pagesOsteopeniaMohamed EssallaaNo ratings yet
- A Guide To Improving The Care of Patients With Fragility Fractures, Edition 2Document63 pagesA Guide To Improving The Care of Patients With Fragility Fractures, Edition 2Alejandro OrduzNo ratings yet
- Osteo RXDocument27 pagesOsteo RXHarun NasutionNo ratings yet
- I. Background: The Hand (PDF - 1.31MB) Hip (PDF - 1.31MB) Knee Top of PageDocument6 pagesI. Background: The Hand (PDF - 1.31MB) Hip (PDF - 1.31MB) Knee Top of PageRisna Allyn AnnisaNo ratings yet
- Orthopedic May 2013Document11 pagesOrthopedic May 2013javi222222No ratings yet
- Osteoporosis: Dr. Muhammad Khairussyakirin B Mohd AliDocument46 pagesOsteoporosis: Dr. Muhammad Khairussyakirin B Mohd AliSaif HadiNo ratings yet
- Dhanwal DK2011Document9 pagesDhanwal DK2011M MNo ratings yet
- Guidelines For Diagnosis and Management of OsteoporosisDocument17 pagesGuidelines For Diagnosis and Management of OsteoporosisVanessaCockerNo ratings yet
- The Fractured Femur: Directed Readings in The ClassroomDocument68 pagesThe Fractured Femur: Directed Readings in The ClassroomEddie Wyatt100% (1)
- Osteoporosis Review of EtiologyDocument17 pagesOsteoporosis Review of EtiologyClaudiaGuerreroNo ratings yet
- OsteoporosisDocument20 pagesOsteoporosisapi-382589667% (3)
- Osteoporosis and Periodontal Disease: History and Physical ExaminationDocument15 pagesOsteoporosis and Periodontal Disease: History and Physical ExaminationYenniy IsmullahNo ratings yet
- Shoolar Ederly OsteoDocument9 pagesShoolar Ederly OsteoBayu Surya AwalludinNo ratings yet
- High Prevalence of Vitamin D Deficiency and Osteoporosis in Patients With Fragility Fractures of Hip - A Pilot StudyDocument4 pagesHigh Prevalence of Vitamin D Deficiency and Osteoporosis in Patients With Fragility Fractures of Hip - A Pilot StudyDiah Rindayani HasbiNo ratings yet
- Best Practice & Research Clinical Rheumatology: Lídia S Anchez-Riera, Nicholas WilsonDocument23 pagesBest Practice & Research Clinical Rheumatology: Lídia S Anchez-Riera, Nicholas WilsonEliacim YnfanteNo ratings yet
- Osteoporosis: Current Concepts: Ibrahim Akkawi Hassan ZmerlyDocument6 pagesOsteoporosis: Current Concepts: Ibrahim Akkawi Hassan ZmerlyDimas M IlhamNo ratings yet
- Osteoporosis: Best PracticeDocument7 pagesOsteoporosis: Best PracticePerez Wahyu PurnasariNo ratings yet
- 2018 Update On OsteoporosisDocument16 pages2018 Update On OsteoporosisManel PopescuNo ratings yet
- Screening, Diagnosis and Treatment of Osteoporosis: A Brief ReviewDocument7 pagesScreening, Diagnosis and Treatment of Osteoporosis: A Brief ReviewraffellaNo ratings yet
- Understanding OsteoporosisDocument6 pagesUnderstanding OsteoporosisPriyank GuptaNo ratings yet
- Geriatria y OrtopediaDocument28 pagesGeriatria y OrtopediaHector VallejosNo ratings yet
- Osteoporosis in The Aging Male: Treatment Options: BackgroundDocument16 pagesOsteoporosis in The Aging Male: Treatment Options: BackgroundcumbredinNo ratings yet
- Lorentz On 2015Document23 pagesLorentz On 2015Sanita AurinNo ratings yet
- Osteoporosis The Evolution in DiagnosisDocument12 pagesOsteoporosis The Evolution in DiagnosisPakistan RevolutionNo ratings yet
- Bone Fragility Fractures in CKD PatientsDocument12 pagesBone Fragility Fractures in CKD PatientsPawan MishraNo ratings yet
- Osteoporosis&Hip Fracture 2017Document2 pagesOsteoporosis&Hip Fracture 2017Ro KohnNo ratings yet
- Bone Reports: A A B C C B CDocument9 pagesBone Reports: A A B C C B Caeroforce20No ratings yet
- Osteoporosis Nejm-2 PDFDocument9 pagesOsteoporosis Nejm-2 PDFDantas Foletto HenriquesNo ratings yet
- Chest: Recent Advances in Chest MedicineDocument10 pagesChest: Recent Advances in Chest MedicineJohn TayNo ratings yet
- Vertebroplasty and Kyphoplasty For The Treatment.6Document12 pagesVertebroplasty and Kyphoplasty For The Treatment.6cooperorthopaedicsNo ratings yet
- Postmenopausal Osteoporosis:: Latest GuidelinesDocument12 pagesPostmenopausal Osteoporosis:: Latest Guidelinesmedicina internaNo ratings yet
- Osteoporosis: Signs and SymptomsDocument9 pagesOsteoporosis: Signs and SymptomschelseachoirNo ratings yet
- Nejmcp 2307353Document13 pagesNejmcp 2307353mohammad.taraz63No ratings yet
- Osteonecrosis of The Femoral Head: Evaluation and TreatmentDocument10 pagesOsteonecrosis of The Femoral Head: Evaluation and TreatmentHector Ulises Quintanilla SotoNo ratings yet
- OsteoarthritisDocument8 pagesOsteoarthritisErick CalcaligongNo ratings yet
- OsteoporosisDocument3 pagesOsteoporosissamtaynbNo ratings yet
- Patogenesis Osteoporosis V PDFDocument15 pagesPatogenesis Osteoporosis V PDFaji pangestuNo ratings yet
- Patogenesis Osteoporosis VDocument15 pagesPatogenesis Osteoporosis Vaji pangestuNo ratings yet
- Math 5 Q3 Week 7Document11 pagesMath 5 Q3 Week 7Cristina Morante100% (2)
- Molykote P40 Grease For Marine IndustryDocument1 pageMolykote P40 Grease For Marine IndustryProject Sales CorpNo ratings yet
- Cell BiologyDocument19 pagesCell BiologyZemetu Gimjaw AlemuNo ratings yet
- SQN 90 Dumper ActuarorDocument9 pagesSQN 90 Dumper ActuarorRomica CiorneiNo ratings yet
- Mathematical Preliminaries and Error Analysis: Per-Olof PerssonDocument16 pagesMathematical Preliminaries and Error Analysis: Per-Olof PerssonLeoncio LadeiraNo ratings yet
- Msds Aerosil R 974Document8 pagesMsds Aerosil R 974Galih Hadi KusumaNo ratings yet
- Chapter 2.1Document152 pagesChapter 2.1Naoto MikaNo ratings yet
- Designing Unstable Landscapes Improvisational Dance Within Cognitive Systems by Marlon Barrios SolanoDocument12 pagesDesigning Unstable Landscapes Improvisational Dance Within Cognitive Systems by Marlon Barrios SolanoMarlon Barrios SolanoNo ratings yet
- E61 DiagramDocument79 pagesE61 Diagramthanes1027No ratings yet
- Alternating Current and Direct Current PDFDocument5 pagesAlternating Current and Direct Current PDFHafiz HamzaNo ratings yet
- PPE Risk Assessment DocumentDocument5 pagesPPE Risk Assessment DocumentFarzanaNo ratings yet
- Tiếng anh 7Document3 pagesTiếng anh 7NGHI PHẠM NGUYỄN GIANo ratings yet
- Training in Sports Class-XII: By: Raman Sharma, Modern Vidya Niketan School, Aravalli HillsDocument18 pagesTraining in Sports Class-XII: By: Raman Sharma, Modern Vidya Niketan School, Aravalli HillsAnish RawatNo ratings yet
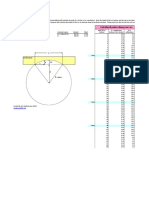
- Arc Layout Calculator: Calculated Points Along Your Arc Enter These ValuesDocument1 pageArc Layout Calculator: Calculated Points Along Your Arc Enter These ValuesPaco PacoNo ratings yet
- Catalogo S20Document25 pagesCatalogo S20Jaime Zzaa100% (1)
- Snapdragon 8 Plus Gen 1 Product BriefDocument2 pagesSnapdragon 8 Plus Gen 1 Product BriefCoc Second AccountNo ratings yet
- 1.introduction To How Differentials WorkDocument9 pages1.introduction To How Differentials WorkSameera SdNo ratings yet
- Food Waste Behavior of Young Fast-Food Consumers in The PhilippinesDocument17 pagesFood Waste Behavior of Young Fast-Food Consumers in The PhilippinesKYLE BRYAN DEL VALLENo ratings yet
- Elcksha23030123 Check BLDocument2 pagesElcksha23030123 Check BLWen'z DinaNo ratings yet
- Alternators Starters PDFDocument1,346 pagesAlternators Starters PDFДима СелютинNo ratings yet
- 36 - Problems On Cost Sheet1Document6 pages36 - Problems On Cost Sheet1Arul JoshNo ratings yet
- Journal of Developmental Psychology. Doi:10.1111/bjdp.12202: VSWM in Children With MLD 1Document27 pagesJournal of Developmental Psychology. Doi:10.1111/bjdp.12202: VSWM in Children With MLD 1Matteo ArcaNo ratings yet
- S5 10-11 Math Yearly Exam Paper 2Document12 pagesS5 10-11 Math Yearly Exam Paper 2Shao Jiaren (Jwss)No ratings yet
- ASV Posi-Track PT-100 Track Loader Mater Parts Catalogue Manual PDFDocument16 pagesASV Posi-Track PT-100 Track Loader Mater Parts Catalogue Manual PDFfisekkkd100% (2)
- Class 10 Social Science Geography Ch-7Document9 pagesClass 10 Social Science Geography Ch-7todiwov781No ratings yet
- I. General InformationDocument9 pagesI. General InformationIlda Lekka RequizaNo ratings yet
- TaxonomyAndClassification GradesK 2Document16 pagesTaxonomyAndClassification GradesK 2BALQIS NURAZIZAHNo ratings yet
- List of Multinational Companies With Research and Development Centres in IsraelDocument10 pagesList of Multinational Companies With Research and Development Centres in IsraelEDUARDONo ratings yet