Download as pdf or txt
You might also like
- Taste of Paradise Chapter 2Document16 pagesTaste of Paradise Chapter 2Gisele Ferreira33% (6)
- TK3723+Data+Sheet+v0 23Document89 pagesTK3723+Data+Sheet+v0 23Phong LêNo ratings yet
- Commentary: Digoxin in Chronic Heart Failure: Possibility of A Second Chance?Document3 pagesCommentary: Digoxin in Chronic Heart Failure: Possibility of A Second Chance?Della Puspita SariNo ratings yet
- Intermittent Low Dose Digoxin May Be Effective and Safe in Patients With Chronic Heart Failure Undergoing Maintenance HemodialysisDocument6 pagesIntermittent Low Dose Digoxin May Be Effective and Safe in Patients With Chronic Heart Failure Undergoing Maintenance Hemodialysisdella psNo ratings yet
- Taking The Wrong Medication of Digoxin TabletsDocument3 pagesTaking The Wrong Medication of Digoxin TabletsMarfu'ah Mar'ahNo ratings yet
- Digoxin, MortalityDocument12 pagesDigoxin, MortalityKenWin NguyễnNo ratings yet
- Sethi 2018Document31 pagesSethi 2018Dina saniasihNo ratings yet
- 4 DigoxinDocument9 pages4 DigoxinThảo VươngNo ratings yet
- Dibacakan Oleh:: Achmad Nur Affendick Adriana Wulandari Dionisia I. Madin Ineke Lani Dimara Lis AmitasariDocument39 pagesDibacakan Oleh:: Achmad Nur Affendick Adriana Wulandari Dionisia I. Madin Ineke Lani Dimara Lis AmitasariMc'onethree BrownNo ratings yet
- 5 Ijca - 3 (2) - 316-323Document8 pages5 Ijca - 3 (2) - 316-323Mythology KingdomNo ratings yet
- Use of Digoxin For Heart Failure and Atrial FibrillationDocument9 pagesUse of Digoxin For Heart Failure and Atrial FibrillationeeleeNo ratings yet
- Effectiveness and Outcomes of H-Isdn in Addition To Conventional Therapy in Acute Heart Failure Patients With Renal ImpairmentDocument10 pagesEffectiveness and Outcomes of H-Isdn in Addition To Conventional Therapy in Acute Heart Failure Patients With Renal ImpairmentIJAR JOURNALNo ratings yet
- Use of Dexmedetomidine As A Sedative and Analgesic Agent in Critically Ill Adult Patients: A Meta-AnalysisDocument14 pagesUse of Dexmedetomidine As A Sedative and Analgesic Agent in Critically Ill Adult Patients: A Meta-AnalysisPatty Alarcón ParraNo ratings yet
- Acute Subdural Hematoma in Patients On OralDocument17 pagesAcute Subdural Hematoma in Patients On OralCinDy Advenia SiarNo ratings yet
- Journal Homepage: - : IntroductionDocument9 pagesJournal Homepage: - : IntroductionIJAR JOURNALNo ratings yet
- 1 s2.0 S105307702300784X MainDocument7 pages1 s2.0 S105307702300784X MainalfintonNo ratings yet
- Jiang 2022Document9 pagesJiang 2022Olivia LimNo ratings yet
- Bo-Jie Wang, Chun-Jing Li, Jian Hu, Huai-Jin Li, Chao Guo, Zhen-Han Wang, Qiao-Chu Zhang, Dong-Liang Mu, Dong-Xin WangDocument6 pagesBo-Jie Wang, Chun-Jing Li, Jian Hu, Huai-Jin Li, Chao Guo, Zhen-Han Wang, Qiao-Chu Zhang, Dong-Liang Mu, Dong-Xin WangferrevNo ratings yet
- PDFDocument14 pagesPDFJardee DatsimaNo ratings yet
- EBPG Guideline On Haemodynamic InstabilityDocument23 pagesEBPG Guideline On Haemodynamic InstabilityJevon JavierNo ratings yet
- Haloperidol RX Delirium Metaanalysis July 2023Document9 pagesHaloperidol RX Delirium Metaanalysis July 2023Jonty ArputhemNo ratings yet
- Digoxin: The Art and Science: ReviewDocument3 pagesDigoxin: The Art and Science: ReviewVisco Da GamaNo ratings yet
- Jaicm MS Id 555727Document7 pagesJaicm MS Id 555727Mita KerjapyNo ratings yet
- Brain and Behavior - 2020 - Feng - Reduced Thiamine Is A Predictor For Cognitive Impairment of Cerebral InfarctionDocument8 pagesBrain and Behavior - 2020 - Feng - Reduced Thiamine Is A Predictor For Cognitive Impairment of Cerebral InfarctionJasna BuhariNo ratings yet
- Anesth Analg 2019 129 6 1504-11Document8 pagesAnesth Analg 2019 129 6 1504-11Fernando SousaNo ratings yet
- Dex Review 2007Document11 pagesDex Review 2007Jackelyne VilelaNo ratings yet
- Pone 0168582Document22 pagesPone 0168582Hening Tirta KusumawardaniNo ratings yet
- Intranasal Midazolam Versus Intravenous Diazepam For The Treatment of Acute Seizures in Paediatric PatientsDocument5 pagesIntranasal Midazolam Versus Intravenous Diazepam For The Treatment of Acute Seizures in Paediatric PatientsArif KusumawidjayaNo ratings yet
- Digoxin Toxicity: Crucial To Diagnose: International Journal of Basic & Clinical PharmacologyDocument2 pagesDigoxin Toxicity: Crucial To Diagnose: International Journal of Basic & Clinical PharmacologyGima Amezia SariNo ratings yet
- Impact of Postoperative Dexmedetomidine Infusion On Incidence of Delirium in Elderly Patients Undergoing Major Elective Noncardiac Surgery2019Document12 pagesImpact of Postoperative Dexmedetomidine Infusion On Incidence of Delirium in Elderly Patients Undergoing Major Elective Noncardiac Surgery2019Cláudia Regina FernandesNo ratings yet
- Sio Jurnal Pertemuan 1Document9 pagesSio Jurnal Pertemuan 1raudatul jannahNo ratings yet
- Hayashi 2015Document5 pagesHayashi 2015Nur Syamsiah MNo ratings yet
- JurnalDocument8 pagesJurnalzefri suhendarNo ratings yet
- Nihms 666087Document24 pagesNihms 666087SouleymaneNo ratings yet
- Guideline For Stress Ulcer Prophylaxis in The Intensive Care UnitDocument4 pagesGuideline For Stress Ulcer Prophylaxis in The Intensive Care Unitannisa edwarNo ratings yet
- Meyfroidt-Smith2019 Article FocusOnDeliriumSedationAndNeurDocument3 pagesMeyfroidt-Smith2019 Article FocusOnDeliriumSedationAndNeurmedicnanaNo ratings yet
- Monitoreo de DigoxinaDocument13 pagesMonitoreo de DigoxinaWalter ReyesNo ratings yet
- Mechanism Underlying Linezolid-Induced Peripheral Neuropathy in Multidrug-Resistant Tuberculosis 2022Document12 pagesMechanism Underlying Linezolid-Induced Peripheral Neuropathy in Multidrug-Resistant Tuberculosis 2022awaluddin andyNo ratings yet
- Impact of Nitrate Use On Survival in Acute Heart Failure: A Propensity-Matched AnalysisDocument12 pagesImpact of Nitrate Use On Survival in Acute Heart Failure: A Propensity-Matched Analysisagung putraNo ratings yet
- Segunda Entrega InvestigacionDocument2 pagesSegunda Entrega InvestigacionDel Rio LauraNo ratings yet
- Surve Rohini 2016Document7 pagesSurve Rohini 2016Amro MahmoudNo ratings yet
- JurnalDocument10 pagesJurnalZaoldyeck PutriNo ratings yet
- Journal Homepage: - : Manuscript HistoryDocument10 pagesJournal Homepage: - : Manuscript HistoryIJAR JOURNALNo ratings yet
- Journal Medicine: The New EnglandDocument9 pagesJournal Medicine: The New Englanddigocivil77No ratings yet
- Harmful Effects of Nsaids Among Patients With Hypertension and Coronary Artery DiseaseDocument7 pagesHarmful Effects of Nsaids Among Patients With Hypertension and Coronary Artery DiseaseFuchsia ZeinNo ratings yet
- Traa 144Document9 pagesTraa 144RashifNo ratings yet
- Evaluation of Sodium Nitroprusside For Controlled Hypotension in Children During SurgeryDocument8 pagesEvaluation of Sodium Nitroprusside For Controlled Hypotension in Children During SurgeryAudra Firthi Dea NoorafiattyNo ratings yet
- Recognize and Treatment of Digitalis Intoxication: Case ReportDocument6 pagesRecognize and Treatment of Digitalis Intoxication: Case ReportKilroy Vincent SterlingNo ratings yet
- Pathological Profile and Recovery Rate in Patients With Drug-Induced Acute Kidney Injury: A Retrospective Study From North-East IndiaDocument7 pagesPathological Profile and Recovery Rate in Patients With Drug-Induced Acute Kidney Injury: A Retrospective Study From North-East IndiaIJAR JOURNALNo ratings yet
- JURDING InternaDocument11 pagesJURDING Internadysha hasyaNo ratings yet
- Indian J PharaDocument7 pagesIndian J PharaprabaNo ratings yet
- Dexmedetomidine: An Updated Review: Annals of Pharmacotherapy March 2007Document11 pagesDexmedetomidine: An Updated Review: Annals of Pharmacotherapy March 2007eriza amalia zainNo ratings yet
- Dexmedetomidine: An Updated Review: Annals of Pharmacotherapy March 2007Document11 pagesDexmedetomidine: An Updated Review: Annals of Pharmacotherapy March 2007eriza amalia zainNo ratings yet
- DDDT 14 4695Document7 pagesDDDT 14 4695IvanGómezNo ratings yet
- MeduriDocument4 pagesMeduriSilvia Leticia BrunoNo ratings yet
- Medi 99 E11005Document6 pagesMedi 99 E11005maninagaNo ratings yet
- Jamaneurology - Meinel - 2023 Intravenous Thrombolysis in Patients With Ischemic Stroke and Recent Ingestion of Direct Oral AnticoagulantsDocument11 pagesJamaneurology - Meinel - 2023 Intravenous Thrombolysis in Patients With Ischemic Stroke and Recent Ingestion of Direct Oral AnticoagulantsAna Margarida J. - PsicólogaNo ratings yet
- Rathore SS. Digoxin in Treatment of Heart FailureDocument8 pagesRathore SS. Digoxin in Treatment of Heart FailureDinhLinhNo ratings yet
- DM - Thiazolidinedione Use, Fluid Retention, and Congestive Heart FailureDocument8 pagesDM - Thiazolidinedione Use, Fluid Retention, and Congestive Heart FailureIntan Siti HulaimaNo ratings yet
- Positive Inotropic Drugs and Drugs Used in DysrhythmiasDocument30 pagesPositive Inotropic Drugs and Drugs Used in DysrhythmiasBurnley JenifferNo ratings yet
- Delirium 5Document5 pagesDelirium 5Raja Friska YulandaNo ratings yet
- Infusion Therapy: For Pain, Headache and Related ConditionsFrom EverandInfusion Therapy: For Pain, Headache and Related ConditionsAlaa Abd-ElsayedNo ratings yet
- Swahili LanguageDocument14 pagesSwahili LanguagenedNo ratings yet
- Lesson 3. The Relationship of Percent Composition and Chemical FormulaDocument4 pagesLesson 3. The Relationship of Percent Composition and Chemical FormulaRandel MontielNo ratings yet
- Avascular Necrosis of The Fibular SesamoidDocument7 pagesAvascular Necrosis of The Fibular SesamoidAlex Yvan Escobedo HinostrozaNo ratings yet
- Bersa Arms 2011 CatalogDocument16 pagesBersa Arms 2011 CatalogAmmoLand Shooting Sports News100% (1)
- European Standard Norme Européenne Europäische Norm: Final Draft Fpren 15316-4-5Document30 pagesEuropean Standard Norme Européenne Europäische Norm: Final Draft Fpren 15316-4-5raduvlasaNo ratings yet
- Poultry Anatomy and PhysiologyDocument40 pagesPoultry Anatomy and PhysiologyMamtaNo ratings yet
- KRTB LFLP71.32Document31 pagesKRTB LFLP71.32Ranadheer BNo ratings yet
- Fundamentals of Breathing The Right Way UpdatedDocument25 pagesFundamentals of Breathing The Right Way UpdatedJohnNo ratings yet
- Test Certificate For Vista Superplast Hs 400 Consignee: Dhariwal Buildtech Ltd. Quantity: 22.022 MT Date: 14-12-2022 Batch No.: VK/2022-23/228Document1 pageTest Certificate For Vista Superplast Hs 400 Consignee: Dhariwal Buildtech Ltd. Quantity: 22.022 MT Date: 14-12-2022 Batch No.: VK/2022-23/228Deepak PachauriaNo ratings yet
- Extended Sample Invoice 0001Document1 pageExtended Sample Invoice 0001importvalleNo ratings yet
- Good and Evil of Moby Dick and Captain AhabDocument4 pagesGood and Evil of Moby Dick and Captain AhabCismaru ElenaNo ratings yet
- Exposure: The PhotoreactionDocument16 pagesExposure: The PhotoreactionGeetha ThiruvengadamNo ratings yet
- Si47 1971 Frenic Lift Loader Im WebDocument128 pagesSi47 1971 Frenic Lift Loader Im WebLogic EngineeringNo ratings yet
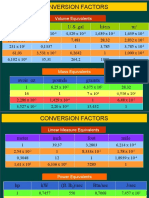
- Conversion Factors: in FT U.S. Gal Liters MDocument8 pagesConversion Factors: in FT U.S. Gal Liters MSamuel MahendraNo ratings yet
- Qualitative Analysis For Active Sulfur Species in Fuels and Solvents (Doctor Test)Document2 pagesQualitative Analysis For Active Sulfur Species in Fuels and Solvents (Doctor Test)Mikael Salamanca100% (1)
- Perfume & Makeup Sale 15.7Document15 pagesPerfume & Makeup Sale 15.7Shane PentonyNo ratings yet
- Surgicals RFQ Fy 2024-25Document225 pagesSurgicals RFQ Fy 2024-25Keshav KumarNo ratings yet
- Avinash Mathematics Project-1 (Edited)Document20 pagesAvinash Mathematics Project-1 (Edited)Harsh SharmaNo ratings yet
- Theology Finals - Grade 11Document7 pagesTheology Finals - Grade 11Sophia BiancaNo ratings yet
- Green Productivity PDFDocument341 pagesGreen Productivity PDFSisca Wiryawan100% (1)
- GY 112 Lecture NotesDocument13 pagesGY 112 Lecture NotesSyed Jabed Miadad AliNo ratings yet
- Bridge Axi AhbDocument22 pagesBridge Axi Ahbkrishnaav100% (1)
- Airport 170923125652Document46 pagesAirport 170923125652Raj GuptaNo ratings yet
- Samsung SH09xWH SH12xWH SERVICE MANUALDocument46 pagesSamsung SH09xWH SH12xWH SERVICE MANUALIoannis Perperis100% (1)
- Practice Test 1: (Code: B1T1)Document16 pagesPractice Test 1: (Code: B1T1)Sách Pháp Hiếu NhânNo ratings yet
- Daniel Dennett-Philosophy Has A Big Role To Play, "If Only It Will Play It" (Prospect)Document3 pagesDaniel Dennett-Philosophy Has A Big Role To Play, "If Only It Will Play It" (Prospect)AidanNo ratings yet
- Heiser - Temperature Charts For Induction and Constant Temperature HeatingDocument10 pagesHeiser - Temperature Charts For Induction and Constant Temperature Heatingsharkdude1134No ratings yet
- Pressurised Mud Cap Drilling Paper (Spe-125311-By Dany)Document7 pagesPressurised Mud Cap Drilling Paper (Spe-125311-By Dany)Hammad KhalidNo ratings yet