
Irac 100
Irac 100
You might also like
- Technical Manual (Part A) Tatuus-Msv 023: Release 1.03 (27/02/2023)Document80 pagesTechnical Manual (Part A) Tatuus-Msv 023: Release 1.03 (27/02/2023)Nelson Piquet Souto Maior100% (1)
- The Art and Science of CIRS MedicineFrom EverandThe Art and Science of CIRS MedicineRating: 5 out of 5 stars5/5 (5)
- S4H - 074 How To Approach Fit To Standard Analysis - CloudDocument44 pagesS4H - 074 How To Approach Fit To Standard Analysis - CloudRaymundo PiresNo ratings yet
- HHS Public Access: Inhalation Injury in The Burned PatientDocument22 pagesHHS Public Access: Inhalation Injury in The Burned PatientDian Laksamana HatiNo ratings yet
- Cigarette Smoking and Inflammation: Cellular and Molecular MechanismsDocument8 pagesCigarette Smoking and Inflammation: Cellular and Molecular MechanismsAnonymous lF3962RA1cNo ratings yet
- s13054 015 1077 4 PDFDocument12 pagess13054 015 1077 4 PDFWidyani WhardanyNo ratings yet
- Radical Causes of CancerDocument10 pagesRadical Causes of CancerCoșmanBogdanPaulNo ratings yet
- Viral Infections in Allergy and Immunology: How Allergic Inflammation Influences Viral Infections and IllnessDocument12 pagesViral Infections in Allergy and Immunology: How Allergic Inflammation Influences Viral Infections and IllnessFajar SukmajayaNo ratings yet
- 05.jurnal ElpridaDocument8 pages05.jurnal ElpridaElfrida PoerbaNo ratings yet
- 1757 7241 21 31 PDFDocument15 pages1757 7241 21 31 PDFAkbar DeyaHarsyaNo ratings yet
- Anestesia en Ninos QuemadosDocument10 pagesAnestesia en Ninos QuemadosMaria Alejandra EchetoNo ratings yet
- Inflammation and Cancer: Reviewarticle Open AccessDocument8 pagesInflammation and Cancer: Reviewarticle Open AccessIrma NeyraNo ratings yet
- Patofisiologi BurnDocument13 pagesPatofisiologi BurntanjudinNo ratings yet
- Jurnal 3Document11 pagesJurnal 3Razua PradanaNo ratings yet
- Asthma Without Borders: EditorialDocument3 pagesAsthma Without Borders: EditorialHesbon MomanyiNo ratings yet
- In Recent YearsDocument10 pagesIn Recent YearsDr-Muhammad Junaid Hassan SharifNo ratings yet
- Referat BedahDocument38 pagesReferat BedahErlanggaTitaNo ratings yet
- Environmental ImpactsDocument10 pagesEnvironmental ImpactsIndra DwinataNo ratings yet
- Contemporary Treatment of LupusDocument13 pagesContemporary Treatment of LupusRamesh KavaliNo ratings yet
- The Role of Inflammation and Genetics in Periodontal DiseaseDocument14 pagesThe Role of Inflammation and Genetics in Periodontal DiseaseNishtha KumarNo ratings yet
- Effect of Free Radicals & Antioxidants On Oxidative Stress A ReviewDocument4 pagesEffect of Free Radicals & Antioxidants On Oxidative Stress A ReviewSeeptianMaulanaNo ratings yet
- NIH Public Access: Author ManuscriptDocument40 pagesNIH Public Access: Author ManuscriptEmira LekaNo ratings yet
- Antitubercular Isoniazid and Drug Resistance of Mycobacterium Tuberculosis - A ReviewDocument16 pagesAntitubercular Isoniazid and Drug Resistance of Mycobacterium Tuberculosis - A ReviewNini FarmNo ratings yet
- Alrouji 2018Document47 pagesAlrouji 2018farah maulida martaNo ratings yet
- Antibiotic Resistance PHD ThesisDocument6 pagesAntibiotic Resistance PHD Thesiskrystalellisonsavannah100% (1)
- Thesis Oxidative StressDocument7 pagesThesis Oxidative Stresskararusselldurham100% (2)
- Inmunoterapia y NutricionDocument18 pagesInmunoterapia y NutricionNaniihSotomayorNo ratings yet
- American Burn AssociationDocument13 pagesAmerican Burn AssociationRaka GhufranNo ratings yet
- Clara JouralDocument4 pagesClara JouralinjessviewNo ratings yet
- 2018 Article 1448Document18 pages2018 Article 1448Delfina RubioNo ratings yet
- Omega 3 Inflamación GripeDocument12 pagesOmega 3 Inflamación GripeCarlos MendozaNo ratings yet
- Medical Consensus 1 19 2016 Indoor Air KB FinalDocument30 pagesMedical Consensus 1 19 2016 Indoor Air KB Finalsuneet srivastavaNo ratings yet
- Chest: Systemic Effects of SmokingDocument10 pagesChest: Systemic Effects of SmokingArlen ResnawaldiNo ratings yet
- Vit C ElderDocument36 pagesVit C ElderEvangelina RivarolaNo ratings yet
- Immune System An Emerging Player of EDC Effect On Metabolic HealthDocument14 pagesImmune System An Emerging Player of EDC Effect On Metabolic Healthshweta pasiNo ratings yet
- Allen 2001Document9 pagesAllen 2001Widia Ade SeptianaNo ratings yet
- Burns: Pathophysiology of Systemic Complications and Current ManagementDocument13 pagesBurns: Pathophysiology of Systemic Complications and Current ManagementHandayaniNo ratings yet
- Anesthetic Management of Patients With Major Burn InjuryDocument10 pagesAnesthetic Management of Patients With Major Burn InjuryPablo Eduardo AmadorNo ratings yet
- Why Have Clinical Trials in Sepsis FailedDocument9 pagesWhy Have Clinical Trials in Sepsis FailedxiaojianNo ratings yet
- Critical Role of Oxidant and Antioxidant in Cancer 2168 9547.1000e110Document2 pagesCritical Role of Oxidant and Antioxidant in Cancer 2168 9547.1000e110Paulo César López BarrientosNo ratings yet
- Management of Acute Smoke Inhalation Injury: ArticleDocument10 pagesManagement of Acute Smoke Inhalation Injury: ArticleYOshie ParrasNo ratings yet
- Ijerph 07 04111Document16 pagesIjerph 07 04111Sukma ArdillaNo ratings yet
- Nelson 2017Document28 pagesNelson 2017Santiago GonzalezNo ratings yet
- Admin, 65-76 Vitamin C As Prevention in Burn Sepsis Vol 2Document12 pagesAdmin, 65-76 Vitamin C As Prevention in Burn Sepsis Vol 2tephy1394No ratings yet
- Articulo 1 Funda PDFDocument35 pagesArticulo 1 Funda PDFErika Lopez OspinaNo ratings yet
- Pathophysiology and Management of Inhalation Trauma in Burn Patients: Literature ReviewDocument7 pagesPathophysiology and Management of Inhalation Trauma in Burn Patients: Literature ReviewPalupiNo ratings yet
- Asthma, Obesity, and Microbiota - A Complex Immunological InteractionDocument33 pagesAsthma, Obesity, and Microbiota - A Complex Immunological InteractionMarcelo CosendeyNo ratings yet
- Infectious Complications of Burns: Lawrence C. Madoff Florencia PereyraDocument4 pagesInfectious Complications of Burns: Lawrence C. Madoff Florencia PereyraJohannes CordeNo ratings yet
- Biochemical Approach To Dental DiseaseDocument8 pagesBiochemical Approach To Dental Diseaseakash_81087No ratings yet
- JPM 13 01479Document16 pagesJPM 13 01479Andreea RacovitaNo ratings yet
- Schreml 2010Document12 pagesSchreml 2010KenWin NguyễnNo ratings yet
- Aem 00756-16Document11 pagesAem 00756-16John KibuukaNo ratings yet
- Cytoquine Storm and SepsisDocument12 pagesCytoquine Storm and SepsisEduardo ChanonaNo ratings yet
- Ceem 14 029 PDFDocument11 pagesCeem 14 029 PDFLegina AromatikaNo ratings yet
- Oxidative Stress in Developmental Origins of DiseaseDocument15 pagesOxidative Stress in Developmental Origins of Diseasem.sonbulNo ratings yet
- Articulo 1Document8 pagesArticulo 1Lisa MarroquinNo ratings yet
- PreviewpdfDocument57 pagesPreviewpdfluisa bibiana garcía martinezNo ratings yet
- Vitagenes Carnitina Hormesis NeurodegeneracionDocument36 pagesVitagenes Carnitina Hormesis NeurodegeneracioncumbredinNo ratings yet
- Extracellular Superoxide Dismutase in Macrophages Augments Bacterial Killing by Promoting PhagocytosisDocument8 pagesExtracellular Superoxide Dismutase in Macrophages Augments Bacterial Killing by Promoting PhagocytosisRezdy Tofan BhaskaraNo ratings yet
- Producing Macrophages T Cells and IL-10 Immunological Priming Requires RegulatoryDocument15 pagesProducing Macrophages T Cells and IL-10 Immunological Priming Requires RegulatoryLaurenceNo ratings yet
- Photodynamic Therapy in Cancer Treatment - An Update ReviewDocument20 pagesPhotodynamic Therapy in Cancer Treatment - An Update ReviewJúnior LimaNo ratings yet
- Immunology Science and Public Health TheDocument1 pageImmunology Science and Public Health ThezishidayatullahbatamNo ratings yet
- EXPERIMENTAL - PDF (Journal Article)Document10 pagesEXPERIMENTAL - PDF (Journal Article)Jeric C. ManaliliNo ratings yet
- Introduction To Mineral Processing 2010Document24 pagesIntroduction To Mineral Processing 2010elmonemNo ratings yet
- TR Technology Radar Vol 27 enDocument43 pagesTR Technology Radar Vol 27 enstart-up.roNo ratings yet
- Fourier OpticsDocument9 pagesFourier Opticssal.paradise.1No ratings yet
- Grade 2 - Assessment ADocument11 pagesGrade 2 - Assessment Aapi-251068386No ratings yet
- All Pass Comb FiltersDocument13 pagesAll Pass Comb Filterspho144No ratings yet
- Kobelco Sk200 8 Excavator Parts Catalog ManualDocument5 pagesKobelco Sk200 8 Excavator Parts Catalog ManualWahyu Yudi100% (2)
- ALB067 Albeo ALV2 Series LED Low Bay Industrial Luminaire Spec SheetDocument4 pagesALB067 Albeo ALV2 Series LED Low Bay Industrial Luminaire Spec SheetsamuelNo ratings yet
- Walt Disney Was Born in ChicagoDocument24 pagesWalt Disney Was Born in ChicagoNyimaSherpaNo ratings yet
- Dhaka University Affiliated Colleges: Third Year Syllabus Department of MathematicsDocument8 pagesDhaka University Affiliated Colleges: Third Year Syllabus Department of MathematicsHasibul Hassan ShantoNo ratings yet
- Db2 Interview QUESTIONS - Advertisement: Java Inteview Questions DB2 SQL Tutorial Mainframe Inteview QuestionsDocument21 pagesDb2 Interview QUESTIONS - Advertisement: Java Inteview Questions DB2 SQL Tutorial Mainframe Inteview Questionssroul4No ratings yet
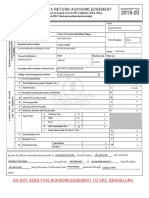
- Acknowledgement ItrDocument1 pageAcknowledgement ItrSourav KumarNo ratings yet
- English ReviewDocument5 pagesEnglish ReviewCherry PinoNo ratings yet
- List of Companies Having SAPDocument2 pagesList of Companies Having SAPKrushikeshNo ratings yet
- 1 - Proposal For 'Vision'Document3 pages1 - Proposal For 'Vision'hiram lodgeNo ratings yet
- Homework Punch CardsDocument5 pagesHomework Punch Cardsafetynbpy100% (1)
- Reflection Paper: Chapter 2Document3 pagesReflection Paper: Chapter 2RedgiemarkNo ratings yet
- Workstationst Modbus® Instruction Guide: Gei-100696EDocument41 pagesWorkstationst Modbus® Instruction Guide: Gei-100696EЕсет ДаулетжанNo ratings yet
- Media Preparation and Uses in Medical MicrobiologyDocument20 pagesMedia Preparation and Uses in Medical MicrobiologyPrincewill SeiyefaNo ratings yet
- Amazon Invoice - Laptop Stand PDFDocument1 pageAmazon Invoice - Laptop Stand PDFAl-Harbi Pvt LtdNo ratings yet
- Mechanism of Titanium Sponge Formation in The Kroll Reduction ReactorDocument11 pagesMechanism of Titanium Sponge Formation in The Kroll Reduction ReactorSrinivasulu PuduNo ratings yet
- Lecture3-Inode Table Content and InodeConversionDocument33 pagesLecture3-Inode Table Content and InodeConversionYaminiNo ratings yet
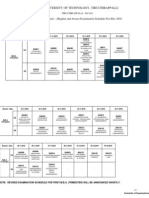
- Anna University of Technology, TiruchirappalliDocument2 pagesAnna University of Technology, TiruchirappallisanjeevrksNo ratings yet
- 5 Practical Use Cases Sankey DiagramDocument5 pages5 Practical Use Cases Sankey DiagramRaviNo ratings yet
- Somewhere I Have Never TravelledDocument221 pagesSomewhere I Have Never TravelledLucy SummerNo ratings yet
- Cholistan Water Relief Project: Presented By: Zohaib Nishad Muhammad Mohsin Mansur Ahsan Zahid Ghazala Baraki Iqra AbidDocument11 pagesCholistan Water Relief Project: Presented By: Zohaib Nishad Muhammad Mohsin Mansur Ahsan Zahid Ghazala Baraki Iqra AbidMansoor SaeedNo ratings yet
- Clarkson Lumber Case QuestionsDocument2 pagesClarkson Lumber Case QuestionsJeffery KaoNo ratings yet
- 0.5ab Sin C 2018-03-19Document10 pages0.5ab Sin C 2018-03-19梁倬林No ratings yet
























































































Download as pdf or txt
You might also like
- Technical Manual (Part A) Tatuus-Msv 023: Release 1.03 (27/02/2023)Document80 pagesTechnical Manual (Part A) Tatuus-Msv 023: Release 1.03 (27/02/2023)Nelson Piquet Souto Maior100% (1)
- The Art and Science of CIRS MedicineFrom EverandThe Art and Science of CIRS MedicineRating: 5 out of 5 stars5/5 (5)
- S4H - 074 How To Approach Fit To Standard Analysis - CloudDocument44 pagesS4H - 074 How To Approach Fit To Standard Analysis - CloudRaymundo PiresNo ratings yet
- HHS Public Access: Inhalation Injury in The Burned PatientDocument22 pagesHHS Public Access: Inhalation Injury in The Burned PatientDian Laksamana HatiNo ratings yet
- Cigarette Smoking and Inflammation: Cellular and Molecular MechanismsDocument8 pagesCigarette Smoking and Inflammation: Cellular and Molecular MechanismsAnonymous lF3962RA1cNo ratings yet
- s13054 015 1077 4 PDFDocument12 pagess13054 015 1077 4 PDFWidyani WhardanyNo ratings yet
- Radical Causes of CancerDocument10 pagesRadical Causes of CancerCoșmanBogdanPaulNo ratings yet
- Viral Infections in Allergy and Immunology: How Allergic Inflammation Influences Viral Infections and IllnessDocument12 pagesViral Infections in Allergy and Immunology: How Allergic Inflammation Influences Viral Infections and IllnessFajar SukmajayaNo ratings yet
- 05.jurnal ElpridaDocument8 pages05.jurnal ElpridaElfrida PoerbaNo ratings yet
- 1757 7241 21 31 PDFDocument15 pages1757 7241 21 31 PDFAkbar DeyaHarsyaNo ratings yet
- Anestesia en Ninos QuemadosDocument10 pagesAnestesia en Ninos QuemadosMaria Alejandra EchetoNo ratings yet
- Inflammation and Cancer: Reviewarticle Open AccessDocument8 pagesInflammation and Cancer: Reviewarticle Open AccessIrma NeyraNo ratings yet
- Patofisiologi BurnDocument13 pagesPatofisiologi BurntanjudinNo ratings yet
- Jurnal 3Document11 pagesJurnal 3Razua PradanaNo ratings yet
- Asthma Without Borders: EditorialDocument3 pagesAsthma Without Borders: EditorialHesbon MomanyiNo ratings yet
- In Recent YearsDocument10 pagesIn Recent YearsDr-Muhammad Junaid Hassan SharifNo ratings yet
- Referat BedahDocument38 pagesReferat BedahErlanggaTitaNo ratings yet
- Environmental ImpactsDocument10 pagesEnvironmental ImpactsIndra DwinataNo ratings yet
- Contemporary Treatment of LupusDocument13 pagesContemporary Treatment of LupusRamesh KavaliNo ratings yet
- The Role of Inflammation and Genetics in Periodontal DiseaseDocument14 pagesThe Role of Inflammation and Genetics in Periodontal DiseaseNishtha KumarNo ratings yet
- Effect of Free Radicals & Antioxidants On Oxidative Stress A ReviewDocument4 pagesEffect of Free Radicals & Antioxidants On Oxidative Stress A ReviewSeeptianMaulanaNo ratings yet
- NIH Public Access: Author ManuscriptDocument40 pagesNIH Public Access: Author ManuscriptEmira LekaNo ratings yet
- Antitubercular Isoniazid and Drug Resistance of Mycobacterium Tuberculosis - A ReviewDocument16 pagesAntitubercular Isoniazid and Drug Resistance of Mycobacterium Tuberculosis - A ReviewNini FarmNo ratings yet
- Alrouji 2018Document47 pagesAlrouji 2018farah maulida martaNo ratings yet
- Antibiotic Resistance PHD ThesisDocument6 pagesAntibiotic Resistance PHD Thesiskrystalellisonsavannah100% (1)
- Thesis Oxidative StressDocument7 pagesThesis Oxidative Stresskararusselldurham100% (2)
- Inmunoterapia y NutricionDocument18 pagesInmunoterapia y NutricionNaniihSotomayorNo ratings yet
- American Burn AssociationDocument13 pagesAmerican Burn AssociationRaka GhufranNo ratings yet
- Clara JouralDocument4 pagesClara JouralinjessviewNo ratings yet
- 2018 Article 1448Document18 pages2018 Article 1448Delfina RubioNo ratings yet
- Omega 3 Inflamación GripeDocument12 pagesOmega 3 Inflamación GripeCarlos MendozaNo ratings yet
- Medical Consensus 1 19 2016 Indoor Air KB FinalDocument30 pagesMedical Consensus 1 19 2016 Indoor Air KB Finalsuneet srivastavaNo ratings yet
- Chest: Systemic Effects of SmokingDocument10 pagesChest: Systemic Effects of SmokingArlen ResnawaldiNo ratings yet
- Vit C ElderDocument36 pagesVit C ElderEvangelina RivarolaNo ratings yet
- Immune System An Emerging Player of EDC Effect On Metabolic HealthDocument14 pagesImmune System An Emerging Player of EDC Effect On Metabolic Healthshweta pasiNo ratings yet
- Allen 2001Document9 pagesAllen 2001Widia Ade SeptianaNo ratings yet
- Burns: Pathophysiology of Systemic Complications and Current ManagementDocument13 pagesBurns: Pathophysiology of Systemic Complications and Current ManagementHandayaniNo ratings yet
- Anesthetic Management of Patients With Major Burn InjuryDocument10 pagesAnesthetic Management of Patients With Major Burn InjuryPablo Eduardo AmadorNo ratings yet
- Why Have Clinical Trials in Sepsis FailedDocument9 pagesWhy Have Clinical Trials in Sepsis FailedxiaojianNo ratings yet
- Critical Role of Oxidant and Antioxidant in Cancer 2168 9547.1000e110Document2 pagesCritical Role of Oxidant and Antioxidant in Cancer 2168 9547.1000e110Paulo César López BarrientosNo ratings yet
- Management of Acute Smoke Inhalation Injury: ArticleDocument10 pagesManagement of Acute Smoke Inhalation Injury: ArticleYOshie ParrasNo ratings yet
- Ijerph 07 04111Document16 pagesIjerph 07 04111Sukma ArdillaNo ratings yet
- Nelson 2017Document28 pagesNelson 2017Santiago GonzalezNo ratings yet
- Admin, 65-76 Vitamin C As Prevention in Burn Sepsis Vol 2Document12 pagesAdmin, 65-76 Vitamin C As Prevention in Burn Sepsis Vol 2tephy1394No ratings yet
- Articulo 1 Funda PDFDocument35 pagesArticulo 1 Funda PDFErika Lopez OspinaNo ratings yet
- Pathophysiology and Management of Inhalation Trauma in Burn Patients: Literature ReviewDocument7 pagesPathophysiology and Management of Inhalation Trauma in Burn Patients: Literature ReviewPalupiNo ratings yet
- Asthma, Obesity, and Microbiota - A Complex Immunological InteractionDocument33 pagesAsthma, Obesity, and Microbiota - A Complex Immunological InteractionMarcelo CosendeyNo ratings yet
- Infectious Complications of Burns: Lawrence C. Madoff Florencia PereyraDocument4 pagesInfectious Complications of Burns: Lawrence C. Madoff Florencia PereyraJohannes CordeNo ratings yet
- Biochemical Approach To Dental DiseaseDocument8 pagesBiochemical Approach To Dental Diseaseakash_81087No ratings yet
- JPM 13 01479Document16 pagesJPM 13 01479Andreea RacovitaNo ratings yet
- Schreml 2010Document12 pagesSchreml 2010KenWin NguyễnNo ratings yet
- Aem 00756-16Document11 pagesAem 00756-16John KibuukaNo ratings yet
- Cytoquine Storm and SepsisDocument12 pagesCytoquine Storm and SepsisEduardo ChanonaNo ratings yet
- Ceem 14 029 PDFDocument11 pagesCeem 14 029 PDFLegina AromatikaNo ratings yet
- Oxidative Stress in Developmental Origins of DiseaseDocument15 pagesOxidative Stress in Developmental Origins of Diseasem.sonbulNo ratings yet
- Articulo 1Document8 pagesArticulo 1Lisa MarroquinNo ratings yet
- PreviewpdfDocument57 pagesPreviewpdfluisa bibiana garcía martinezNo ratings yet
- Vitagenes Carnitina Hormesis NeurodegeneracionDocument36 pagesVitagenes Carnitina Hormesis NeurodegeneracioncumbredinNo ratings yet
- Extracellular Superoxide Dismutase in Macrophages Augments Bacterial Killing by Promoting PhagocytosisDocument8 pagesExtracellular Superoxide Dismutase in Macrophages Augments Bacterial Killing by Promoting PhagocytosisRezdy Tofan BhaskaraNo ratings yet
- Producing Macrophages T Cells and IL-10 Immunological Priming Requires RegulatoryDocument15 pagesProducing Macrophages T Cells and IL-10 Immunological Priming Requires RegulatoryLaurenceNo ratings yet
- Photodynamic Therapy in Cancer Treatment - An Update ReviewDocument20 pagesPhotodynamic Therapy in Cancer Treatment - An Update ReviewJúnior LimaNo ratings yet
- Immunology Science and Public Health TheDocument1 pageImmunology Science and Public Health ThezishidayatullahbatamNo ratings yet
- EXPERIMENTAL - PDF (Journal Article)Document10 pagesEXPERIMENTAL - PDF (Journal Article)Jeric C. ManaliliNo ratings yet
- Introduction To Mineral Processing 2010Document24 pagesIntroduction To Mineral Processing 2010elmonemNo ratings yet
- TR Technology Radar Vol 27 enDocument43 pagesTR Technology Radar Vol 27 enstart-up.roNo ratings yet
- Fourier OpticsDocument9 pagesFourier Opticssal.paradise.1No ratings yet
- Grade 2 - Assessment ADocument11 pagesGrade 2 - Assessment Aapi-251068386No ratings yet
- All Pass Comb FiltersDocument13 pagesAll Pass Comb Filterspho144No ratings yet
- Kobelco Sk200 8 Excavator Parts Catalog ManualDocument5 pagesKobelco Sk200 8 Excavator Parts Catalog ManualWahyu Yudi100% (2)
- ALB067 Albeo ALV2 Series LED Low Bay Industrial Luminaire Spec SheetDocument4 pagesALB067 Albeo ALV2 Series LED Low Bay Industrial Luminaire Spec SheetsamuelNo ratings yet
- Walt Disney Was Born in ChicagoDocument24 pagesWalt Disney Was Born in ChicagoNyimaSherpaNo ratings yet
- Dhaka University Affiliated Colleges: Third Year Syllabus Department of MathematicsDocument8 pagesDhaka University Affiliated Colleges: Third Year Syllabus Department of MathematicsHasibul Hassan ShantoNo ratings yet
- Db2 Interview QUESTIONS - Advertisement: Java Inteview Questions DB2 SQL Tutorial Mainframe Inteview QuestionsDocument21 pagesDb2 Interview QUESTIONS - Advertisement: Java Inteview Questions DB2 SQL Tutorial Mainframe Inteview Questionssroul4No ratings yet
- Acknowledgement ItrDocument1 pageAcknowledgement ItrSourav KumarNo ratings yet
- English ReviewDocument5 pagesEnglish ReviewCherry PinoNo ratings yet
- List of Companies Having SAPDocument2 pagesList of Companies Having SAPKrushikeshNo ratings yet
- 1 - Proposal For 'Vision'Document3 pages1 - Proposal For 'Vision'hiram lodgeNo ratings yet
- Homework Punch CardsDocument5 pagesHomework Punch Cardsafetynbpy100% (1)
- Reflection Paper: Chapter 2Document3 pagesReflection Paper: Chapter 2RedgiemarkNo ratings yet
- Workstationst Modbus® Instruction Guide: Gei-100696EDocument41 pagesWorkstationst Modbus® Instruction Guide: Gei-100696EЕсет ДаулетжанNo ratings yet
- Media Preparation and Uses in Medical MicrobiologyDocument20 pagesMedia Preparation and Uses in Medical MicrobiologyPrincewill SeiyefaNo ratings yet
- Amazon Invoice - Laptop Stand PDFDocument1 pageAmazon Invoice - Laptop Stand PDFAl-Harbi Pvt LtdNo ratings yet
- Mechanism of Titanium Sponge Formation in The Kroll Reduction ReactorDocument11 pagesMechanism of Titanium Sponge Formation in The Kroll Reduction ReactorSrinivasulu PuduNo ratings yet
- Lecture3-Inode Table Content and InodeConversionDocument33 pagesLecture3-Inode Table Content and InodeConversionYaminiNo ratings yet
- Anna University of Technology, TiruchirappalliDocument2 pagesAnna University of Technology, TiruchirappallisanjeevrksNo ratings yet
- 5 Practical Use Cases Sankey DiagramDocument5 pages5 Practical Use Cases Sankey DiagramRaviNo ratings yet
- Somewhere I Have Never TravelledDocument221 pagesSomewhere I Have Never TravelledLucy SummerNo ratings yet
- Cholistan Water Relief Project: Presented By: Zohaib Nishad Muhammad Mohsin Mansur Ahsan Zahid Ghazala Baraki Iqra AbidDocument11 pagesCholistan Water Relief Project: Presented By: Zohaib Nishad Muhammad Mohsin Mansur Ahsan Zahid Ghazala Baraki Iqra AbidMansoor SaeedNo ratings yet
- Clarkson Lumber Case QuestionsDocument2 pagesClarkson Lumber Case QuestionsJeffery KaoNo ratings yet
- 0.5ab Sin C 2018-03-19Document10 pages0.5ab Sin C 2018-03-19梁倬林No ratings yet