Professional Documents
Culture Documents
The American Association of Endocrine Surgeons Guidelines For Definitive Management of Primary Hyperparathyroidism
The American Association of Endocrine Surgeons Guidelines For Definitive Management of Primary Hyperparathyroidism
Uploaded by
henry hernandezOriginal Title
Copyright
Available Formats
Share this document
Did you find this document useful?
Is this content inappropriate?
Report this DocumentCopyright:
Available Formats
The American Association of Endocrine Surgeons Guidelines For Definitive Management of Primary Hyperparathyroidism
The American Association of Endocrine Surgeons Guidelines For Definitive Management of Primary Hyperparathyroidism
Uploaded by
henry hernandezCopyright:
Available Formats
See discussions, stats, and author profiles for this publication at: https://www.researchgate.
net/publication/306267976
The American Association of Endocrine Surgeons Guidelines for Definitive
Management of Primary Hyperparathyroidism
Article in JAMA Surgery · August 2016
DOI: 10.1001/jamasurg.2016.2310
CITATIONS READS
839 1,274
16 authors, including:
Tracy S. Wang Daniel T Ruan
Medical College of Wisconsin Tampa General Hospital
186 PUBLICATIONS 6,053 CITATIONS 92 PUBLICATIONS 8,263 CITATIONS
SEE PROFILE SEE PROFILE
James Lee Sylvia L Asa
Columbia University Case Western Reserve University and University Health Network Toronto
135 PUBLICATIONS 5,220 CITATIONS 862 PUBLICATIONS 66,202 CITATIONS
SEE PROFILE SEE PROFILE
All content following this page was uploaded by Miguel Herrera on 31 May 2018.
The user has requested enhancement of the downloaded file.
Clinical Review & Education
JAMA Surgery | Special Communication
The American Association of Endocrine Surgeons Guidelines
for Definitive Management of Primary Hyperparathyroidism
Scott M. Wilhelm, MD; Tracy S. Wang, MD, MPH; Daniel T. Ruan, MD; James A. Lee, MD; Sylvia L. Asa, MD, PhD;
Quan-Yang Duh, MD; Gerard M. Doherty, MD; Miguel F. Herrera, MD, PhD; Janice L. Pasieka, MD;
Nancy D. Perrier, MD; Shonni J. Silverberg, MD; Carmen C. Solórzano, MD; Cord Sturgeon, MD;
Mitchell E. Tublin, MD; Robert Udelsman, MD, MBA; Sally E. Carty, MD
Invited Commentary
IMPORTANCE Primary hyperparathyroidism (pHPT) is a common clinical problem for which Author Audio Interview at
the only definitive management is surgery. Surgical management has evolved considerably jamasurgery.com
during the last several decades.
Supplemental content at
jamasurgery.com
OBJECTIVE To develop evidence-based guidelines to enhance the appropriate, safe, and
effective practice of parathyroidectomy.
EVIDENCE REVIEW A multidisciplinary panel used PubMed to review the medical literature
from January 1, 1985, to July 1, 2015. Levels of evidence were determined using the American
College of Physicians grading system, and recommendations were discussed until consensus.
FINDINGS Initial evaluation should include 25-hydroxyvitamin D measurement, 24-hour urine
calcium measurement, dual-energy x-ray absorptiometry, and supplementation for vitamin D
deficiency. Parathyroidectomy is indicated for all symptomatic patients, should be considered
for most asymptomatic patients, and is more cost-effective than observation or
pharmacologic therapy. Cervical ultrasonography or other high-resolution imaging is
recommended for operative planning. Patients with nonlocalizing imaging remain surgical
candidates. Preoperative parathyroid biopsy should be avoided. Surgeons who perform a
high volume of operations have better outcomes. The possibility of multigland disease should
be routinely considered. Both focused, image-guided surgery (minimally invasive
parathyroidectomy) and bilateral exploration are appropriate operations that achieve high
cure rates. For minimally invasive parathyroidectomy, intraoperative parathyroid hormone
monitoring via a reliable protocol is recommended. Minimally invasive parathyroidectomy is
not routinely recommended for known or suspected multigland disease. Ex vivo aspiration of
resected parathyroid tissue may be used to confirm parathyroid tissue intraoperatively.
Clinically relevant thyroid disease should be assessed preoperatively and managed during
parathyroidectomy. Devascularized normal parathyroid tissue should be autotransplanted.
Patients should be observed postoperatively for hematoma, evaluated for hypocalcemia and
symptoms of hypocalcemia, and followed up to assess for cure defined as eucalcemia at more
than 6 months. Calcium supplementation may be indicated postoperatively. Familial pHPT,
reoperative parathyroidectomy, and parathyroid carcinoma are challenging entities that
require special consideration and expertise.
CONCLUSIONS AND RELEVANCE Evidence-based recommendations were created to assist
clinicians in the optimal treatment of patients with pHPT.
Author Affiliations: Author
affiliations are listed at the end of this
article.
Corresponding Author: Scott M.
Wilhelm, MD, Department of Surgery,
University Hospitals/Case Medical
Center, 11100 Euclid Ave, Cleveland,
JAMA Surg. doi:10.1001/jamasurg.2016.2310 OH 44118 (scott.wilhelm
Published online August 10, 2016. @uhhospitals.org).
(Reprinted) E1
Copyright 2016 American Medical Association. All rights reserved.
Downloaded From: http://archsurg.jamanetwork.com/ by a University Health Network (UNH) User on 08/19/2016
Clinical Review & Education Special Communication AAES Guidelines for Primary Hyperparathyroidism Management
T
he surgical treatment of primary hyperparathyroidism normal parathyroid glands. The disease is characterized by the per-
(pHPT) has undergone extensive change in the past sistent elevation of total serum calcium levels with corresponding
2 decades. The presentation, diagnosis, and medical man- elevated or inappropriately normal (ie, nonsuppressed) PTH lev-
agement have been previously addressed by an international els. The diagnosis of pHPT is biochemical. The clinical presentation
workshop.1-4 To meet the need for a detailed focus on operative is heterogeneous, and the associated symptoms overlap with those
management, the American Association of Endocrine Surgeons of aging and disease. Patients with symptomatic pHPT have overt
(AAES) developed evidence-based guidelines to delineate the safe signs and symptoms; however, the definition of symptomatic dis-
and effective practice of parathyroidectomy to achieve definitive ease is still evolving. Patients with asymptomatic pHPT have no
treatment. disease-specific symptoms.
Normocalcemic pHPT is a recently recognized, incompletely
characterized variant that presents with high PTH levels and nor-
mal total and ionized serum calcium levels. Some, but not all,
Methods
patients may progress over time to hypercalcemic pHPT.6
A multidisciplinary panel of endocrinologists, pathologists, sur-
geons, and radiologists established PubMed search parameters for Establishing the Diagnosis: Laboratory Testing
the worldwide medical literature from January 1, 1985, to July 1, 2015, In pHPT, patients may occasionally have normal total and/or ion-
using the National Library of Medicine Medical Subject Headings and ized calcium levels but are hypercalcemic most of the time. Thus,
keywords (hyperparathyroidism, primary; parathyroid neoplasms; repeated measurements of calcium are required.3 Total serum cal-
and hyperparathyroidism) linked by boolean operators. The writ- cium levels are reported in milligrams per deciliter (to convert to mil-
ing group adopted the American College of Physicians grading sys- limoles per liter, multiply by 0.25) and should be corrected for
tem for evidence-based guidelines,5 which uses a validated scale to serum albumin (eAppendix in the Supplement). Although pHPT
critically evaluate the strength and quality of the evidence. Recom- and malignant tumors are the most common causes of hypercalce-
mendations are designated strong when benefits clearly outweigh mia in adults, other causes should be considered. Patients with
risks and/or the recommendation should be applied to all or most normocalcemic pHPT have normal serum and ionized calcium lev-
patients without reservation, weak for equivalent risks or uncer- els; thus, measurement of ionized calcium is necessary to establish
tainty, and insufficient when evidence is conflicting or of poor qual- the diagnosis of normocalcemic, but not hypercalcemic, pHPT.
ity. Evidence quality is graded high for randomized clinical trials or In pHPT, PTH levels are high or inappropriately normal (ie, not
overwhelming evidence, moderate for randomized clinical trials with suppressed despite hypercalcemia). Diagnosis of normocalcemic
significant limitations or large observational studies, and low for small pHPT requires the exclusion of other causes of secondary eleva-
observational or case studies. tion of PTH (eTable 2 in the Supplement). Nonparathyroid causes
In guidelines construction, the evidence was rigorously examined, of hypercalcemia are associated with suppressed PTH. Renal func-
recommendations were graded, and text was amended to achieve tion and vitamin D status should be assessed preoperatively.
consensus. Feedback was sought from an independent group of non- • Recommendation 1-1: The biochemical evaluation of suspected
author clinicians, the AAES membership, and other expert sources. pHPT should include serum total calcium, PTH, creatinine, and
These guidelines present a process for the evaluation and sur- 25-hydroxyvitamin D levels (strong recommendation; moderate-
gical treatment of pHPT based on evidence at the time of writing. quality evidence).
They do not represent the only approach to the management of adult A 24-hour urinary calcium level is important to distinguish pHPT
pHPT and are not meant to replace an individual physician’s judg- from familial hypocalciuric hypercalcemia, which is an autosomal
ment. Adherence to the guidelines is not mandatory, may require dominant disorder of the renal calcium-sensing receptor that can
adaptation in practice settings with barriers to implementation, and mimic pHPT. Familial hypocalciuric hypercalcemia should be con-
does not constitute a legal standard of care. The writing group had sidered in patients with long-standing hypercalcemia, urinary cal-
complete independence from the AAES in the production of the evi- cium levels less than 100 mg/24 hours, and a calcium to creatinine
dence-based guidelines. clearance ratio less than 0.01 (eAppendix in the Supplement).
• Recommendation 1-2: A 24-hour urine measurement of calcium
and creatinine should be considered in patients undergoing evalu-
ation for possible pHPT (strong recommendation; moderate-
Recommendations
quality evidence).
The full evidence statements supporting the recommendations
appear in the eAppendix and eTable 1 in the Supplement. The Investigation of Symptoms, Features,
Supplement also includes additional details, technical descrip- and Complications
tions, discussions of controversy, and expert advice on the surgical A careful history should be performed for objective renal and skel-
management of pHPT. etal manifestations, including nephrolithiasis, fragility fractures, and
osteoporosis. Subjective symptoms, including neuropsychiatric, cog-
nitive, musculoskeletal, and gastrointestinal complaints (eAppen-
dix in the Supplement), should be documented because parathy-
Diagnosis and Evaluation
roidectomy may lead to improvement or resolution of these
Primary hyperparathyroidism is a common disorder that arises from symptoms. Certain medications can cause biochemical changes that
autonomous overproduction of parathyroid hormone (PTH) by ab- mimic pHPT (eAppendix in the Supplement). In 3% to 5% of pa-
E2 JAMA Surgery Published online August 10, 2016 (Reprinted) jamasurgery.com
Copyright 2016 American Medical Association. All rights reserved.
Downloaded From: http://archsurg.jamanetwork.com/ by a University Health Network (UNH) User on 08/19/2016
AAES Guidelines for Primary Hyperparathyroidism Management Special Communication Clinical Review & Education
tients, pHPT occurs as a component of an inherited syndrome occur as germline alterations in hyperparathyroidism–jaw tumor syn-
(eAppendix in the Supplement).7-9 drome and familial isolated hyperparathyroidism and as somatic
• Recommendation 1-3: In patients with suspected pHPT, a per- events in sporadic parathyroid cancer (PCA) (eAppendix in the
sonal and family history should be taken (strong recommenda- Supplement).
tion; moderate-quality evidence). • Recommendation 2-2: Exposure-related and genotype-
Patients with otherwise asymptomatic pHPT may have neph- phenotype correlations are predictive of parathyroid anatomical
rocalcinosis or silent nephrolithiasis; both are indications for and pathophysiologic features and should be considered be-
parathyroidectomy.4 cause they may affect the planning and conduct of surgery (strong
• Recommendation 1-4: In patients with asymptomatic pHPT, recommendation; moderate-quality evidence).
abdominal imaging should be performed for detection of nephro-
calcinosis or nephrolithiasis (weak recommendation; low-quality
evidence).
Indications and Outcomes of Intervention
Primary hyperparathyroidism causes site-specific reduction in
bone mineral density (BMD) and may predispose patients to fragil- Parathyroidectomy is the only definitive treatment of pHPT. Symp-
ity fractures.4 Dual-energy x-ray absorptiometry (DXA) examina- tomatic patients are expected to derive clear benefits from cura-
tion is appropriate for all patients with pHPT and should be per- tive parathyroidectomy, and patients considered to be asymptom-
formed to screen for clinically relevant skeletal manifestations.4 atic frequently report improvement in quality-of-life indexes.11-14
• Recommendation 1-5: Bone mineral density should be mea- Observation and pharmacologic therapy are less effective and less
sured at the lumbar spine, hip, and distal radius, preferably using cost-effective than surgery, even when the patient is considered
DXA (strong recommendation; high-quality evidence). asymptomatic.15 Long-term hypercalcemia should be avoided
In patients with pHPT attributable to a hereditary syndrome, the because of potential deleterious effects (eAppendix in the
timing and extent of parathyroidectomy are affected by the pres- Supplement).16-18 Referral to an experienced parathyroid surgeon
ence and specific type of mutation present (eAppendix in the is advised to determine whether the likelihood and benefits of cure
Supplement).9 outweigh the anticipated risks of the procedure.
• Recommendation 1-6: Genetic counseling should be performed • Recommendation 3-1: Parathyroidectomy is indicated, and is the
for patients younger than 40 years with pHPT and multigland preferred treatment, for all patients with symptomatic pHPT
disease (MGD) and considered for those with a family history or (strong recommendation; high-quality evidence).
syndromic manifestations (strong recommendation; low-quality • Recommendation 3-2: Parathyroidectomy is indicated when the
evidence). serum calcium level is greater than 1 mg/dL above normal, regard-
less of whether objective symptoms are present or absent (strong
recommendation; low-quality evidence).
After successful parathyroidectomy, the development of new
Epidemiology and Pathogenesis
kidney stones decreases markedly.19 Although renal insufficiency
The recognition of pHPT increased in the 1970s with automated rou- and nephrocalcinosis do not resolve, surgery may prevent a fur-
tine calcium testing, and prevalence continues to increase today. In- ther decline in the glomerular filtration rate (eAppendix in the
cidence appears to increase with age and is 2 to 3 times higher in Supplement).
women (eAppendix in the Supplement). Primary hyperparathyroid- • Recommendation 3-3: Parathyroidectomy is indicated for objec-
ism remains underdiagnosed and undertreated. tive evidence of renal involvement, including silent nephrolithia-
Safe and effective parathyroidectomy requires mastery of the sis on renal imaging, nephrocalcinosis, hypercalciuria (24-hour urine
anatomical and pathophysiologic features of pHPT (eAppendix in the calcium level >400 mg/dL) with increased stone risk, or impaired
Supplement). Autonomous PTH secretion may be attributable to hy- renal function (glomerular filtration rate <60 mL/min) (weak rec-
perfunction of 1 or more glands and is caused by 3 different patho- ommendation; low-quality evidence).
logic conditions: adenoma, hyperplasia, or carcinoma. The overall Primary hyperparathyroidism causes a decrease in BMD, most
frequency of MGD is 6% to 33% (eAppendix in the Supplement). pronounced at cortical bone sites, such as the distal third of the ra-
• Recommendation 2-1: Multigland disease affects approximately dius. Parathyroidectomy improves BMD and appears to reduce frac-
15% of patients with pHPT and should be routinely considered in ture rate, even for normal or osteopenic bone (eAppendix in the
preoperative planning (strong recommendation; moderate- Supplement).16
quality evidence). • Recommendation 3-4: Parathyroidectomy is indicated in pa-
Lithium-associated pHPT occurs in up to 15% of long-term us- tients with pHPT and osteoporosis, fragility fracture, or evidence
ers, with increased rates of MGD.10 Molecular alterations also affect of vertebral compression fracture on spine imaging (strong rec-
the pathophysiologic mechanisms and rates of MGD (eAppendix in ommendation; high-quality evidence).
the Supplement). Germline inactivating mutation of the MEN1 gene Patients 50 years or younger at diagnosis require prolonged
(OMIM 613733) causes multiple endocrine neoplasia type 1, and so- monitoring and compared with older patients have a higher inci-
matic events occur in sporadic tumors; germline activating muta- dence of progression (eAppendix in the Supplement).20
tions of the RET (OMIM 188550) proto-oncogene result in multiple • Recommendation 3-5: Parathyroidectomy is indicated when pHPT
endocrine neoplasia type 2; the somatic PRAD1 (OMIM 168461) re- is diagnosed at 50 years or younger regardless of whether objec-
arrangement upregulates cyclin D1 in sporadic adenomas; and in- tive or subjective features are present or absent (strong recom-
activating mutations of CDC73 (formerly HRPT2) (OMIM 607393) mendation; moderate-quality evidence).
jamasurgery.com (Reprinted) JAMA Surgery Published online August 10, 2016 E3
Copyright 2016 American Medical Association. All rights reserved.
Downloaded From: http://archsurg.jamanetwork.com/ by a University Health Network (UNH) User on 08/19/2016
Clinical Review & Education Special Communication AAES Guidelines for Primary Hyperparathyroidism Management
The preoperative diagnosis of PCA may be difficult. If PCA is sus- • Recommendation 3-12: Operative management is more effec-
pected, patients should be treated surgically because this is the only tive and cost-effective than long-term observation or pharmaco-
potentially curative treatment (eAppendix in the Supplement). logic therapy (strong recommendation; moderate-quality
• Recommendation 3-6: Parathyroidectomy is indicated when the evidence).
clinical or biochemical evidence is consistent with PCA (strong rec- Parathyroidectomy for pHPT is not recommended when the
ommendation; high-quality evidence). risks of surgery or anesthesia are outweighed by the anticipated ben-
Patients who choose not to undergo surgery should undergo efits of cure, as with severe or overriding medical illness (eAppen-
annual biochemical evaluation and periodic DXA. If the patient does dix in the Supplement). In patients who meet none of these indica-
not have the means or desire to adhere to a planned observation tions for surgical intervention, refuse surgery, or are considered
schedule, parathyroidectomy should be offered (eAppendix in the prohibitively high risk, medical intervention aimed at mitigating spe-
Supplement).14 cific sequelae should be used.2 For many patients, mild disease will
• Recommendation 3-7: Parathyroidectomy is the preferred treat- progress over time.24
ment for patients who are unable or unwilling to comply with
observation protocols (strong recommendation; low-quality
evidence).
Parathyroid Localization Modalities:
Patients with pHPT frequently have neurocognitive and neu-
ropsychiatric symptoms. With varying response patterns, 3 random- What Imaging to Perform and When
ized clinical trials demonstrated neurocognitive benefits of surgery Guiding Principles
vs observation.13,14,21
• Recommendation 3-8: Parathyroidectomy is recommended for 1. Imaging has no utility in confirming or excluding the diagnosis of
patients with neurocognitive and/or neuropsychiatric symptoms pHPT.
that are attributable to pHPT (strong recommendation; low- 2. Imaging results should not be used to select patients for surgi-
quality evidence). cal referral. Patients with negative imaging results remain can-
Patients with pHPT may have higher rates of myocardial infarc- didates for parathyroidectomy.
tion, hypertension, stroke, congestive heart failure, diabetes, and 3. There is marked regional variability in imaging accuracy. When
mortality (eAppendix in the Supplement). Observational studies in imaging with initially negative results is performed again at high-
mild pHPT have yielded conflicting data about the improvement of volume centers, the sensitivity of localization improves to as high
cardiac parameters after parathyroidectomy. It is prudent to weigh as 92%.25
the possibility of mitigating cardiovascular morbidity and mortality 4. Imaging is performed after deciding to proceed with parathy-
on a case-by-case basis. roidectomy and is performed for operative planning.
• Recommendation 3-9: Parathyroidectomy may be offered to sur- 5. Parathyroid imaging is significantly less accurate for MGD.26
gical candidates with cardiovascular disease who might benefit 6. Recommendation 4-1: Patients who are candidates for parathy-
from mitigation of potential cardiovascular sequelae other than roidectomy should be referred to an expert clinician to decide
hypertension (weak recommendation; low-quality evidence). which imaging studies to perform based on their knowledge of
Observational studies16 suggest that several nontraditional regional imaging capabilities (strong recommendation; low-
quality evidence).
and/or newly studied symptoms improve after successful parathy-
7. Recommendation 4-2: Patients who are candidates for sur-
roidectomy, including muscle strength, functional capacity, gastro-
gery and have negative or discordant imaging results should still
esophageal reflux, sleep patterns, and fibromyalgia (eAppendix in
be referred to a parathyroid surgeon for evaluation (strong rec-
the Supplement).
ommendation; low-quality evidence).
• Recommendation 3-10a: The nontraditional symptoms of muscle
Cervical ultrasonography performed by an experienced parathy-
weakness, functional capacity, and abnormal sleep patterns should
roid sonographer is the least costly imaging modality and, when com-
be considered in the decision for parathyroidectomy (weak rec-
bined with sestamibi or 4-dimensional computed tomography, is the
ommendation; moderate-quality evidence).
most cost-effective strategy (eAppendix in the Supplement).26-28
• Recommendation 3-10b: The nontraditional features of gastro-
esophageal reflux and fibromyalgia symptoms may be considered Preoperative ultrasound-directed fine-needle aspiration biopsy of
in the decision for parathyroidectomy (insufficient evidence). parathyroid lesions is highly specific but is rarely necessary and can
The success rate for surgeons who perform fewer than 10 para- have undesirable consequences (eAppendix in the Supplement).
thyroidectomies per year is lower than for experienced surgeons • Recommendation 4-3: Cervical ultrasonography is recom-
(eAppendix in the Supplement). Volume of operations inversely cor- mended to localize parathyroid disease and assess for concomi-
relates with complications, cost, and length of stay.22 tant thyroid disease (strong recommendation; low-quality
evidence).
• Recommendation 3-11: Parathyroidectomy should be conducted
• Recommendation 4-4: Preoperative parathyroid fine-needle
by surgeons with adequate training and experience in pHPT man-
aspiration biopsy is not recommended except in unusual, difficult
agement (strong recommendation; moderate-quality evidence).
cases of pHPT and should not be performed if PCA is suspected
Although many pharmacologic agents have been used in an at-
(insufficient evidence).
tempt to reduce the serum calcium level or stabilize BMD, none have
Technetium Tc 99m sestamibi is the dominant radioisotope in
improved both (eAppendix in the Supplement). In formal cost-
parathyroid scintigraphy. Each sestamibi protocol (dual-phase, io-
effectiveness analyses, pharmacologic treatment is not optimal at
dine 131 subtraction, single-photon emission computed tomogra-
any life expectancy.15,23
E4 JAMA Surgery Published online August 10, 2016 (Reprinted) jamasurgery.com
Copyright 2016 American Medical Association. All rights reserved.
Downloaded From: http://archsurg.jamanetwork.com/ by a University Health Network (UNH) User on 08/19/2016
AAES Guidelines for Primary Hyperparathyroidism Management Special Communication Clinical Review & Education
phy) has individual strengths and weaknesses (eAppendix in the tions guided by IPM has been excellent, with cure rates as high as
Supplement). Sensitivity in MGD is poor. Combined ultrasonogra- 97% to 99% (eTable 3 in the Supplement).30 Focused operations
phy and sestamibi imaging increases localization accuracy and im- guided solely by imaging studies without IPM can miss MGD, with
proves sensitivity (eAppendix in the Supplement). Although tradi- failure rates that may be higher than accepted standards (eAppen-
tional computed tomography has little utility, the 4-dimensional dix in the Supplement). For initial image-guided surgery, positive
computed tomography protocol has emerged as a useful modality, imaging directs where to start exploration, and the results of intra-
although sensitivity in MGD is limited. operative PTH monitoring help to terminate it.
• Recommendation 4-5: An experienced clinician should help de- • Recommendation 6-1: When image-guided focused parathyroid-
termine which type of imaging to use based on knowledge of their ectomy is planned, IPM is suggested to avoid higher operative fail-
region’s imaging capabilities (strong recommendation; moderate- ure rates (strong recommendation; moderate-quality evidence).
quality evidence). The accuracy of IPM depends on the protocol used. Surgeons
• Recommendation 4-6: Magnetic resonance imaging and ve- should use a protocol that is practical, accurate, and reproducible
nous sampling can be considered in cases of subsequent opera- and be aware of potential sources of error (eAppendix in the Supple-
tion, difficult localization, or ionizing radiation contraindication ment). In addition, IPM is useful in differential jugular venous
(weak recommendation; low-quality evidence). sampling and ex vivo parathyroid aspiration (eAppendix in the
Supplement).
• Recommendation 6-2: Surgeons who use IPM should use a sam-
pling protocol that is reliable in the local environment and should
Preoperative Management be familiar with the interpretation of PTH decay dynamics (strong
recommendation; low-quality evidence).
A daily intake of 1000 to 1200 mg of calcium is recommended for
adults and appears appropriate for patients with pHPT as well. Di-
etary restriction of calcium is not advised in pHPT. Preoperative
vitamin D repletion is advised and should be performed carefully in Minimally Invasive Parathyroidectomy
patients with hypercalciuria (eAppendix in the Supplement).
Approximately 85% of patients with pHPT have a solitary ad-
• Recommendation 5-1: Most patients with pHPT should follow In-
enoma, the resection of which results in durable cure. Thus, sur-
stitute of Medicine guidelines for calcium intake (strong recom-
geons have adapted a variety of methods to streamline parathy-
mendation; moderate-quality evidence).
roidectomy and reduce the risk of complications, collectively termed
• Recommendation 5-2: Before parathyroidectomy, patients with
minimally invasive parathyroidectomy (MIP). All MIP techniques are
pHPT who are vitamin D deficient can safely begin vitamin D supple-
designed to limit dissection, hasten recovery, reduce postopera-
mentation (weak recommendation; low-quality evidence).
tive discomfort, and reduce incision length. These techniques typi-
Subjective assessment of voice quality is an essential compo-
cally require preoperative imaging and other adjuncts.
nent of preoperative examination. Additional objective evaluation
Regardless of MIP technique, specific strategies are advised to
is recommended for subjective changes, surgeon-identified abnor-
improve the likelihood of success (eAppendix in the Supplement),
malities, or any history of prior operations in which the vagus nerve
including selection by imaging results. Minimally invasive parathy-
or recurrent laryngeal nerve (RLN) was at risk (eAppendix in the
roidectomy can achieve cure in 97% to 99% of selected patients
Supplement).
when adjunctive IPM is used to confirm adequacy of resection (eAp-
• Recommendation 5-3: Preoperative voice evaluation should in-
pendix in the Supplement).31 During MIP, if IPM suggests residual hy-
clude specific inquiry about subjective voice changes, with addi-
persecreting tissue, conversion to bilateral exploration (BE) is war-
tional evaluation for significant voice changes or a history of prior
ranted and has equivalent cure rates to planned BE.
at-risk surgery (strong recommendation; low-quality evidence).
• Recommendation 7-1: Defined as a focused dissection, MIP is ide-
Hypercalcemic crisis is defined by a rapid-onset, albumin-
ally used in patients who appear clinically and by imaging to have
corrected serum calcium level greater than 14 mg/dL and signs or
a single parathyroid adenoma. It is not routinely recommended in
symptoms of multiorgan dysfunction.29 Intravenous fluid resusci-
patients with known or suspected high risk of MGD (strong rec-
tation and pharmacologic management are used to stabilize pa-
ommendation; high-quality evidence).
tients before expeditious parathyroidectomy. The presence of PCA
• Recommendation 7-2: Ex vivo PTH aspiration or frozen section
should be considered (eAppendix in the Supplement).
analysis may be used to confirm the resection of parathyroid tis-
Recommendation 5-4: Patients with pHPT who present with hy- sue (weak recommendation; low-quality evidence).
percalcemic crisis should be medically managed, followed by para- • Recommendation 7-3: During MIP, the discovery of MGD, the in-
thyroidectomy (strong recommendation; low-quality evidence). ability to identify an abnormal gland, or the failure to achieve an
appropriate IPM decrease should prompt conversion to BE (strong
recommendation; high-quality evidence).
Intraoperative PTH Monitoring
Intraoperative PTH monitoring (IPM) provides real-time assess-
Bilateral Exploration
ment of parathyroid function and has a major effect on focused op-
erations when the surgeon removes an image-identified abnormal In BE, all parathyroid glands should be identified and compared to
gland without additional dissection. The success of focused opera- deduce the presence of a single adenoma or MGD. Bilateral explo-
jamasurgery.com (Reprinted) JAMA Surgery Published online August 10, 2016 E5
Copyright 2016 American Medical Association. All rights reserved.
Downloaded From: http://archsurg.jamanetwork.com/ by a University Health Network (UNH) User on 08/19/2016
Clinical Review & Education Special Communication AAES Guidelines for Primary Hyperparathyroidism Management
• Recommendation 9-2: In multiple endocrine neoplasia type
Figure 1. Anatomical Relationships of Eutopic and Ectopic
Parathyroid Glands 2A–associated pHPT, resection of only visibly enlarged glands
is recommended (weak recommendation; low-quality evidence).
Surgical Adjuncts
The most widely used surgical adjunct is IPM. Other adjuncts
(eAppendix in the Supplement) can assist with confirmation of
resected parathyroid tissue (frozen section analysis, ex vivo para-
thyroid aspiration), gland visualization (methylene blue, near
infrared fluorescence or infrared spectroscopy), and gland local-
ization (intraoperative ultrasonography, bilateral jugular venous
sampling, or γ-probe guidance). Monitoring of the RLN is used
less often in parathyroid than thyroid surgery but may play a role
in subsequent operation. Adjuncts cannot replace judgment and
experience.
Concurrent Thyroidectomy
In patients with pHPT, concomitant thyroid disease is frequent
(12%-67%) (eAppendix in the Supplement). Concurrent thyroidec-
tomy may be performed for thyroid disease that requires resec-
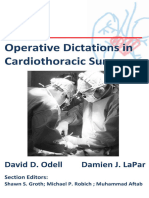
ration has long-term success rates greater than 95% and low com- tion, suspicion of PCA, removal of an abnormal intrathyroidal para-
plication rates.22,32 Familiarity with parathyroid anatomy, the loca- thyroid gland, or improved access.
tions of eutopic (normal position) and ectopic glands (Figure 1), and • Recommendation 11-1: Patients undergoing parathyroidectomy
the appearance of normal and abnormal glands (eAppendix in the should have preoperative thyroid evaluation because of the high
Supplement) is essential. rate of concomitant disease, which may require thyroid resection
• Recommendation 8-1: Bilateral exploration provides a time- (strong recommendation; moderate-quality evidence).
tested standard of efficacy and safety in the definitive treatment Compared with intraoperative thyroid examination, preopera-
of pHPT (strong recommendation; high-quality evidence). tive ultrasonography is more sensitive and specific for clinically sig-
• Recommendation 8-2: Planned BE is the preferred operative strat- nificant thyroid disease and is associated with a 5-fold lower rate of
egy in situations of discordant or nonlocalizing preoperative thyroid resection.33 Preoperative identification of thyroid disease
imaging, when there is a high suspicion of MGD, when IPM is not may facilitate performance of the most appropriate index opera-
available, or at the discretion of the surgeon (strong recommen- tion, reduce complications, and avoid future reoperation (eAppen-
dation; moderate-quality evidence). dix in the Supplement).
• Recommendation 8-3: Bilateral exploration is defined by a stan- • Recommendation 11-2: In patients with concomitant pHPT and
dard technique in which all parathyroid glands are identified with thyroid disease that requires resection, thyroid resection should
exploration of expected and, if necessary, ectopic cervical loca- be performed at the time of parathyroidectomy (strong recom-
tions (strong recommendation; moderate-quality evidence). mendation; moderate-quality evidence).
• Recommendation 8-4: In lithium-induced pHPT, the surgical • Recommendation 11-3: Evaluation for concomitant thyroid dis-
approach may be BE or MIP guided by imaging and IPM (weak rec- ease in patients undergoing parathyroidectomy for pHPT should
ommendation; low-quality evidence). follow evidence-based guidelines (strong recommendation; high-
quality evidence).
• Recommendation 11-4: The indications for thyroidectomy for con-
comitant thyroid disease during parathyroidectomy for pHPT are
Familial pHPT
the same as those for patients with isolated thyroid disease and
In patients with a genetic predisposition for pHPT (eAppendix in the should follow evidence-based guidelines (strong recommenda-
Supplement), the high likelihood of MGD and recurrent hypercal- tion; high-quality evidence).
cemia necessitate a distinctive surgical approach with the goals of
achieving eucalcemia for as long as possible, avoiding hypoparathy-
roidism, and facilitating potential subsequent operation for recur-
Parathyroid Carcinoma
rence. Lifelong follow-up is critical.
• Recommendation 9-1: In patients with multiple endocrine neo- Parathyroid cancer accounts for approximately 1% of all cases of
plasia type 1–associated pHPT, subtotal parathyroidectomy is pHPT and typically presents with very high PTH and calcium levels
recommended as the index operation (strong recommendation; (eTable 4 in Supplement).34 Parathyroidectomy is the only cura-
moderate-quality evidence). tive treatment for PCA.
E6 JAMA Surgery Published online August 10, 2016 (Reprinted) jamasurgery.com
Copyright 2016 American Medical Association. All rights reserved.
Downloaded From: http://archsurg.jamanetwork.com/ by a University Health Network (UNH) User on 08/19/2016
AAES Guidelines for Primary Hyperparathyroidism Management Special Communication Clinical Review & Education
• Recommendation 12-1: The diagnosis of PCA should be consid- • Recommendation 14-3: Short-term calcium and/or vitamin D
ered in patients with pHPT with markedly elevated PTH levels supplementation for prophylaxis against hypocalcemia should be
and severe hypercalcemia (strong recommendation; low-quality considered after parathyroidectomy (weak recommendation; low-
evidence). quality evidence).
• Recommendation 12-2: With intraoperative suspicion of parathy- Outpatient parathyroidectomy can be performed in selected
roid carcinoma, complete resection avoiding capsular disruption patients. An overnight stay may be appropriate for patients under-
improves the likelihood of cure and may require en bloc resection going subsequent operation, extensive exploration, or subtotal para-
of adherent tissues (strong recommendation; low-quality thyroidectomy or those with profound vitamin D deficiency, social
evidence). issues, or expected nonadherence.
• Recommendation 12-3: Prophylactic central or lateral neck dis- • Recommendation 14-4: Outpatient parathyroid surgery can be
section should not be performed for parathyroid carcinoma considered in selected patients (weak recommendation; low-
(insufficient evidence). quality evidence).
• Recommendation 12-4: The histologic diagnosis of PCA relies on The assessment of cure and complications (prolonged hypopara-
identification of unequivocal angioinvasion and can be assisted thyroidism, permanent RLN paralysis) requires evaluation for at least
by biomarkers (strong recommendation; moderate-quality 6 months. Longitudinal testing should include calcium, PTH, and
evidence). 25-hydroxyvitamin D levels. Achieving normal vitamin D levels post-
• Recommendation 12-5: Adjuvant external beam radiotherapy operatively will help absorption of calcium and normalization of PTH
should not be routinely performed after surgical resection of PCA levels and may improve BMD (eAppendix in the Supplement).
and is reserved as a palliative option (strong recommendation; low- • Recommendation 14-5: After apparently successful parathyroid-
quality evidence). ectomy, calcium intake should follow the Institute of Medicine
• Recommendation 12-6: Patients with functional PCA should Dietary Reference Intakes (strong recommendation; moderate-
undergo regular surveillance by testing serum calcium and PTH quality evidence).
levels (strong recommendation; low-quality evidence). • Recommendation 14-6: Patients who are vitamin D deficient
should receive vitamin D supplementation after apparently suc-
cessful parathyroidectomy (strong recommendation; moderate-
quality evidence).
Autotransplantation and Cryopreservation
• Recommendation 14-7: At 6 months, surgeons individually or in
Autotransplantation is the most reliable method to preserve func- conjunction with the multidisciplinary care team should assess post-
tion when a gland cannot be kept viable on its vascular pedicle. The parathyroidectomy patients for cure and evidence of long-term
arterial perfusion of parathyroid glands that have been manipu- complications (strong recommendation; low-quality evidence).
lated but are left in situ should be assessed. All efforts should be made
to preserve the maximal amount of normal parathyroid tissue and
to treat each parathyroid gland as carefully as if it were the last
Cure and Failure
(eAppendix in the Supplement).
• Recommendation 13-1: Immediate autotransplantation is recom- The goal of parathyroidectomy is cure. Cure rates for parathyroid-
mended for normal parathyroid glands that appear devascular- ectomy in sporadic pHPT should approach 95% to 99%. Although
ized (strong recommendation; low-quality evidence). there is no role for routine PTH measurement in the normocalce-
mic patient in the immediate postoperative period, failure to nor-
malize PTH levels at 6 months or longer can signify early operative
failure. In normocalcemic pHPT, the PTH level must also normalize
Immediate Postoperative Care
to indicate cure. In patients with inherited forms of pHPT, a differ-
Although a common finding, especially in vitamin D–deficient pa- ent end point of care pertains (eAppendix in the Supplement).
tients or those with malabsorption for any reason (eg, celiac dis- • Recommendation 15-1a: Cure after parathyroidectomy is
ease or prior bariatric surgery), symptomatic hypocalcemia is typi- defined as the reestablishment of normal calcium homeostasis
cally transient and managed as an outpatient.32,35,36 Patients lasting a minimum of 6 months (strong recommendation;
undergoing BE have significantly higher rates of mild and severe high-quality evidence).
hypocalcemic symptoms.37,38 The reported rates of moderate • Recommendation 15-1b: Patients with normocalcemic pHPT who
postoperative hypocalcemia range from 5% to 47%.39 After initial have persistently elevated PTH levels after parathyroidectomy
parathyroid surgery, permanent hypoparathyroidism is rare should be evaluated and treated for causes of secondary HPT and,
(0%-3.6%).32,35-37 if none are present, monitored for recurrent disease (strong rec-
• Recommendation 14-1: The operative note should detail ommendation; low-quality evidence).
the findings and events of parathyroidectomy (insufficient • Recommendation 15-2: Surgeons should choose an operative ap-
evidence). proach that in their hands carries a high cure rate, low-risk profile,
• Recommendation 14-2: After parathyroidectomy, patients should and cost comparable to other available techniques (strong recom-
be observed in a monitored setting for the development of cervi- mendation; low-quality evidence).
cal hematoma. Evidence of compressive hematoma after parathy- • Recommendation 15-3: In normocalcemic pHPT, the definition of
roidectomy should prompt emergency decompression (strong cure must include normal calcium and PTH levels more than
recommendation; low-quality evidence). 6 months after surgery (insufficient evidence).
jamasurgery.com (Reprinted) JAMA Surgery Published online August 10, 2016 E7
Copyright 2016 American Medical Association. All rights reserved.
Downloaded From: http://archsurg.jamanetwork.com/ by a University Health Network (UNH) User on 08/19/2016
Clinical Review & Education Special Communication AAES Guidelines for Primary Hyperparathyroidism Management
Figure 2. Algorithm for the Evaluation and Management of Persistent or Recurrent Primary
Hyperparathyroidism (pHPT)
Patient with suspected persistent
or recurrent pHPT
Confirmation of diagnosis
No
Continue routine follow-up
Review previous images, operative
reports, pathologic test results, and
vocal cord function examination results
Meets criteria for subsequent operation
No Continue routine follow-up and
nonoperative management
Patient is an operative candidate
Does not localize
Does not localize
Noninvasive imaging studies Consider invasive imaging
Localizes
Subsequent parathyroidectomy
(IPM suggested)
IPM indicates intraoperative
parathyroid hormone monitoring.
Operative failure remains the most common complication of • Recommendation 16-2: Patients with transient hypoparathyroid-
parathyroidectomy. Failure may be predicted by an incomplete de- ism after surgery should be treated with calcium and, if neces-
crease in IPM levels or kinetic analysis. Diagnosis of failure requires sary, calcitriol supplements, which should be weaned as toler-
discontinuation of calcium use and a stepwise evaluation (eAppen- ated. Patients with prolonged hypoparathyroidism may be
dix in the Supplement). Surgeons should be cognizant of their fail- considered for recombinant PTH therapy (weak recommenda-
ure rates. tion; low-quality evidence).
• Recommendation 15-4: Persistent pHPT should be defined as a
failure to achieve normocalcemia within 6 months of parathyroid-
ectomy. Recurrent pHPT is defined by recurrence of hypercalce-
mia after a normocalcemic interval at more than 6 months Subsequent Operation
after parathyroidectomy (strong recommendation; high-quality Reoperative parathyroidectomy is defined as any prior cervical op-
evidence). eration that placed the RLN at risk. In persistent or recurrent pHPT,
subsequent operation is often recommended to achieve biochemi-
cal cure. Because cure rates are lower (82%-98%) (eAppendix in the
Management of Other Complications Supplement) and risks are higher, many surgeons use stricter indi-
cations for subsequent operation than for initial surgery.41,42 A care-
Laryngeal reinnervation does not restore normal vocal fold move- ful data evaluation, assessment for surgical indications beyond the
ment, but it may improve voice strength, reduce the risk of aspira- biochemical diagnosis, and positive imaging results are essential; this
tion, and decrease the need for postoperative vocal cord medial- algorithm is detailed in Figure 2. Intraoperative PTH monitoring and
ization and injections. other adjuncts are often used.
• Recommendation 16-1: When RLN transection is recognized dur-
ing parathyroidectomy, a reinnervation procedure should be at- • Recommendation 17-1: The evaluation of persistent or recurrent
tempted (strong recommendation; low-quality evidence). pHPT should include confirmation of biochemical diagnosis, as-
The symptoms of postoperative hypoparathyroidism include sessment of indications for surgery, review of prior records if avail-
perioral numbness and fingertip paresthesias, which can also oc- able, and evaluation of RLN function (strong recommendation;
cur in euparathyroid bone hunger or transient hypoparathyroidism low-quality evidence).
(eAppendix in the Supplement). Severe postoperative hypocalce- • Recommendation 17-2: Patients with persistent or recurrent pHPT
mia is rare. Patients may require temporary postoperative calcium should be evaluated by an experienced parathyroid surgeon be-
administration and calcitriol to avoid such symptoms (eAppendix in fore the decision to proceed with surgery or nonoperative man-
the Supplement). In contrast, prolonged hypoparathyroidism is agement (strong recommendation; low-quality evidence).
a chronic condition of such diminished parathyroid function that • Recommendation 17-3: Intraoperative PTH monitoring should be
ongoing calcium and calcitriol treatment is required for 6 to considered in patients undergoing reoperative parathyroidec-
12 months.40 tomy for pHPT (strong recommendation; low-quality evidence).
E8 JAMA Surgery Published online August 10, 2016 (Reprinted) jamasurgery.com
Copyright 2016 American Medical Association. All rights reserved.
Downloaded From: http://archsurg.jamanetwork.com/ by a University Health Network (UNH) User on 08/19/2016
AAES Guidelines for Primary Hyperparathyroidism Management Special Communication Clinical Review & Education
definitive treatment of pHPT. These evidence-based guidelines
Conclusions provide a broad-based approach to the clinical spectrum of pHPT
and, although they do not represent the only acceptable
Because the surgical treatment of pHPT has undergone extensive approach, serve as a sound template for the effective surgical
change in the last 2 decades, the AAES determined the need to management of pHPT to achieve cure as safely and efficiently as
develop evidence-based clinical guidelines to enhance the safe, possible.
ARTICLE INFORMATION 5. Qaseem A, Snow V, Owens DK, Shekelle P; 19. Mollerup CL, Vestergaard P, Frøkjaer VG,
Accepted for Publication: May 19, 2016. Clinical Guidelines Committee of the American Mosekilde L, Christiansen P, Blichert-Toft M. Risk of
College of Physicians. The development of clinical renal stone events in primary hyperparathyroidism
Published Online: August 10, 2016. practice guidelines and guidance statements of the before and after parathyroid surgery: controlled
doi:10.1001/jamasurg.2016.2310. American College of Physicians: summary of retrospective follow up study. BMJ. 2002;325
Author Affiliations: Department of Surgery, methods. Ann Intern Med. 2010;153(3):194-199. (7368):807.
University Hospitals/Case Medical Center, 6. Bilezikian JP, Silverberg SJ. Normocalcemic 20. Silverberg SJ, Brown I, Bilezikian JP. Age as
Cleveland, Ohio (Wilhelm); Department of Surgery, primary hyperparathyroidism. Arq Bras Endocrinol a criterion for surgery in primary hyperparathy-
Medical College of Wisconsin, Milwaukee (Wang); Metabol. 2010;54(2):106-109. roidism. Am J Med. 2002;113(8):681-684.
Department of Surgery, Brigham and Women’s
Hospital, Boston, Massachusetts (Ruan); 7. Evans DB, Rich TA, Cote GJ. Surgical 21. Rao DS, Phillips ER, Divine GW, Talpos GB.
Department of Surgery, Columbia University management of familial hyperparathyroidism. Randomized controlled clinical trial of surgery
College of Physicians and Surgeons, New York, Ann Surg Oncol. 2007;14(5):1525-1527. versus no surgery in patients with mild
New York (Lee); Department of Pathology, 8. Stålberg P, Carling T. Familial parathyroid asymptomatic primary hyperparathyroidism. J Clin
University of Toronto, Toronto, Ontario, Canada tumors: diagnosis and management. World J Surg. Endocrinol Metab. 2004;89(11):5415-5422.
(Asa); Department of Surgery, University of 2009;33(11):2234-2243. 22. Abdulla AG, Ituarte PH, Harari A, Wu JX,
California San Francisco Medical Center, San 9. Thakker RV, Newey PJ, Walls GV, et al; Endocrine Yeh MW. Trends in the frequency and quality of
Francisco (Duh); Department of Surgery, Boston Society. Clinical practice guidelines for multiple parathyroid surgery: analysis of 17,082 cases over
University, Boston, Massachusetts (Doherty); endocrine neoplasia type 1 (MEN1). J Clin Endocrinol 10 years. Ann Surg. 2015;261(4):746-750.
Instituto Nacional de Ciencias Médicas y Nutrición Metab. 2012;97(9):2990-3011. 23. Zanocco K, Sturgeon C. How should age
Salvador Zubirán, Mexico City, Mexico (Herrera); at diagnosis impact treatment strategy in
Department of Surgery, University of Calgary, 10. Awad SS, Miskulin J, Thompson N. Parathyroid
adenomas versus four-gland hyperplasia as the asymptomatic primary hyperparathyroidism?
Calgary, Alberta, Canada (Pasieka); Department of a cost-effectiveness analysis. Surgery. 2008;144(2):
Surgery, MD Anderson Cancer Center, Houston, cause of primary hyperparathyroidism in patients
with prolonged lithium therapy. World J Surg. 2003; 290-298.
Texas (Perrier); Department of Medicine, Columbia
University College of Physicians and Surgeons, 27(4):486-488. 24. Rubin MR, Bilezikian JP, McMahon DJ, et al.
New York, New York (Silverberg); Department of 11. Pasieka JL, Parsons L, Jones J. The long-term The natural history of primary hyperparathyroidism
Surgery, Vanderbilt University Medical Center, benefit of parathyroidectomy in primary with or without parathyroid surgery after 15 years.
Nashville, Tennessee (Solórzano); Department of hyperparathyroidism: a 10-year prospective J Clin Endocrinol Metab. 2008;93(9):3462-3470.
Surgery, Northwestern University, Chicago, Illinois surgical outcome study. Surgery. 2009;146(6): 25. Rodgers SE, Hunter GJ, Hamberg LM, et al.
(Sturgeon); Department of Radiology, University 1006-1013. Improved preoperative planning for directed
of Pittsburgh, Pittsburgh, Pennsylvania (Tublin); 12. Pasieka JL, Parsons LL. Prospective surgical parathyroidectomy with 4-dimensional computed
Department of Surgery, Yale University, New outcome study of relief of symptoms following tomography. Surgery. 2006;140(6):932-940.
Haven, Connecticut (Udelsman); Department of surgery in patients with primary hyperparathy- 26. Solorzano CC, Carneiro-Pla D. Minimizing cost
Surgery, University of Pittsburgh, Pittsburgh, roidism. World J Surg. 1998;22(6):513-518. and maximizing success in the preoperative
Pennsylvania (Carty). localization strategy for primary hyperparathy-
13. Sheldon DG, Lee FT, Neil NJ, Ryan JA Jr. Surgical
Conflict of Interest Disclosures: None reported. treatment of hyperparathyroidism improves roidism. Surg Clin North Am. 2014;94(3):587-605.
Additional Information: Dr Carty is the chair of the health-related quality of life. Arch Surg. 2002;137 27. Lubitz CC, Hunter GJ, Hamberg LM, et al.
AAES Parathyroidectomy Guidelines Writing Group. (9):1022-1026. Accuracy of 4-dimensional computed tomography
14. Ambrogini E, Cetani F, Cianferotti L, et al. in poorly localized patients with primary
REFERENCES Surgery or surveillance for mild asymptomatic hyperparathyroidism. Surgery. 2010;148(6):
1. Bilezikian JP, Brandi ML, Eastell R, et al. primary hyperparathyroidism: a prospective, 1129-1137.
Guidelines for the management of asymptomatic randomized clinical trial. J Clin Endocrinol Metab. 28. Wang TS, Cheung K, Farrokhyar F, Roman SA,
primary hyperparathyroidism: summary statement 2007;92(8):3114-3121. Sosa JA. Would scan, but which scan? a cost-utility
from the Fourth International Workshop. J Clin 15. Zanocco K, Angelos P, Sturgeon C. analysis to optimize preoperative imaging for
Endocrinol Metab. 2014;99(10):3561-3569. Cost-effectiveness analysis of parathyroidectomy primary hyperparathyroidism. Surgery. 2011;150(6):
2. Marcocci C, Bollerslev J, Khan AA, Shoback DM. for asymptomatic primary hyperparathyroidism. 1286-1294.
Medical management of primary hyperparathy- Surgery. 2006;140(6):874-881. 29. Starker LF, Björklund P, Theoharis C,
roidism: proceedings of the fourth International 16. Vestergaard P, Mosekilde L. Cohort study on Long WD III, Carling T, Udelsman R. Clinical
Workshop on the Management of Asymptomatic effects of parathyroid surgery on multiple and histopathological characteristics of
Primary Hyperparathyroidism. J Clin Endocrinol outcomes in primary hyperparathyroidism. BMJ. hyperparathyroidism-induced hypercalcemic
Metab. 2014;99(10):3607-3618. 2003;327(7414):530-534. crisis. World J Surg. 2011;35(2):331-335.
3. Eastell R, Brandi ML, Costa AG, D’Amour P, 17. Rolighed L, Amstrup AK, Jakobsen NF, et al. 30. Irvin GL III, Carneiro DM, Solorzano CC.
Shoback DM, Thakker RV. Diagnosis of Muscle function is impaired in patients with Progress in the operative management of sporadic
asymptomatic primary hyperparathyroidism: “asymptomatic” primary hyperparathyroidism. primary hyperparathyroidism over 34 years.
proceedings of the Fourth International Workshop. World J Surg. 2014;38(3):549-557. Ann Surg. 2004;239(5):704-708.
J Clin Endocrinol Metab. 2014;99(10):3570-3579. 31. McCoy KL, Chen NH, Armstrong MJ, et al.
18. Reiher AE, Mazeh H, Schaefer S, Gould J,
4. Silverberg SJ, Clarke BL, Peacock M, et al. Chen H, Sippel RS. Symptoms of gastroesophageal The small abnormal parathyroid gland is
Current issues in the presentation of asymptomatic reflux disease improve after parathyroidectomy. increasingly common and heralds operative
primary hyperparathyroidism: proceedings of the Surgery. 2012;152(6):1232-1237. complexity. World J Surg. 2014;38(6):
Fourth International Workshop. J Clin Endocrinol 1274-1281.
Metab. 2014;99(10):3580-3594.
jamasurgery.com (Reprinted) JAMA Surgery Published online August 10, 2016 E9
Copyright 2016 American Medical Association. All rights reserved.
Downloaded From: http://archsurg.jamanetwork.com/ by a University Health Network (UNH) User on 08/19/2016
Clinical Review & Education Special Communication AAES Guidelines for Primary Hyperparathyroidism Management
32. Allendorf J, DiGorgi M, Spanknebel K, symptoms of postoperative hypocalcemia and 40. Stack BC Jr, Bimston DN, Bodenner DL, et al.
Inabnet W, Chabot J, Logerfo P. 1112 consecutive secondary hyperparathyroidism after minimally American Association of Clinical Endocrinologists
bilateral neck explorations for primary invasive parathyroidectomy. Surgery. 2005;138(6): and American College of Endocrinology Disease
hyperparathyroidism. World J Surg. 2007;31(11): 1018-1025. state clinical review: postoperative
2075-2080. 37. Bergenfelz A, Lindblom P, Tibblin S, hypoparathyroidism—definitions and management.
33. Milas M, Mensah A, Alghoul M, et al. The impact Westerdahl J. Unilateral versus bilateral neck Endocr Pract. 2015;21(6):674-685.
of office neck ultrasonography on reducing exploration for primary hyperparathyroidism: 41. Karakas E, Müller HH, Schlosshauer T,
unnecessary thyroid surgery in patients undergoing a prospective randomized controlled trial. Ann Surg. Rothmund M, Bartsch DK. Reoperations for primary
parathyroidectomy. Thyroid. 2005;15(9): 2002;236(5):543-551. hyperparathyroidism: improvement of outcome
1055-1059. 38. Roman SA, Sosa JA, Pietrzak RH, et al. over two decades. Langenbecks Arch Surg. 2013;
34. van Heerden JA, Weiland LH, ReMine WH, The effects of serum calcium and parathyroid 398(1):99-106.
Walls JT, Purnell DC. Cancer of the parathyroid hormone changes on psychological and cognitive 42. Weber CJ, Sewell CW, McGarity WC.
glands. Arch Surg. 1979;114(4):475-480. function in patients undergoing parathyroidectomy Persistent and recurrent sporadic primary
35. Udelsman R, Åkerström G, Biagini C, et al. for primary hyperparathyroidism. Ann Surg. 2011; hyperparathyroidism: histopathology,
The surgical management of asymptomatic primary 253(1):131-137. complications, and results of reoperation. Surgery.
hyperparathyroidism: proceedings of the Fourth 39. Mittendorf EA, Merlino JI, McHenry CR. 1994;116(6):991-998.
International Workshop. J Clin Endocrinol Metab. Post-parathyroidectomy hypocalcemia: incidence,
2014;99(10):3595-3606. risk factors, and management. Am Surg. 2004;70
36. Stewart ZA, Blackford A, Somervell H, et al. (2):114-119.
25-hydroxyvitamin D deficiency is a risk factor for
E10 JAMA Surgery Published online August 10, 2016 (Reprinted) jamasurgery.com
Copyright 2016 American Medical Association. All rights reserved.
DownloadedViewFrom:
publicationhttp://archsurg.jamanetwork.com/
stats by a University Health Network (UNH) User on 08/19/2016
You might also like
- The Psychiatric Interview - Daniel CarlatDocument473 pagesThe Psychiatric Interview - Daniel CarlatAntonio L Yang94% (31)
- Blumgart's Surgery of The Liver, Biliary Tract, and Pancreas 6ed 2017 2vols 2401pag PDFDocument2,401 pagesBlumgart's Surgery of The Liver, Biliary Tract, and Pancreas 6ed 2017 2vols 2401pag PDFLucia Maria De Castro Mendes94% (32)
- Cardiothoracic Operative DictationDocument345 pagesCardiothoracic Operative DictationRheechaNo ratings yet
- APEA 3P Question Bank With AnswersDocument10 pagesAPEA 3P Question Bank With AnswersOleg Knaz100% (1)
- Hair Transplant Surgery and Platelet Rich Plasma: Evidence-Based EssentialsFrom EverandHair Transplant Surgery and Platelet Rich Plasma: Evidence-Based EssentialsLinda N. LeeNo ratings yet
- Color Atlas of Differential Diagnosis in Exfoliative and Aspiration Cytopathology 2nd EditionDocument1,035 pagesColor Atlas of Differential Diagnosis in Exfoliative and Aspiration Cytopathology 2nd Editiontalha riaz100% (2)
- Pulmonology Step2 CKDocument22 pagesPulmonology Step2 CKsarwat86% (7)
- Case Study (Aub)Document16 pagesCase Study (Aub)Lucila Lugo0% (2)
- Adams and Victor's Principles of Neurology, 9th EditionDocument171 pagesAdams and Victor's Principles of Neurology, 9th EditionAlvyna LaksitaNo ratings yet
- Guia para HiperparatirodiismoDocument10 pagesGuia para HiperparatirodiismoOskar MartinezNo ratings yet
- ProgramRequirements SAGEDocument16 pagesProgramRequirements SAGEJuan José Ruiz CastilloNo ratings yet
- GuidelineonValve-RegurgAssessment JASE2019Document46 pagesGuidelineonValve-RegurgAssessment JASE2019MAX ANTHONY SALAMANCA HILASACANo ratings yet
- 03 Na CB GuidelinesDocument152 pages03 Na CB GuidelinesPutri Zahra ArdiyanitaNo ratings yet
- Guideline 2017 Autologous Breast ReconstructionDocument14 pagesGuideline 2017 Autologous Breast ReconstructionPedroAngelToribioOrbegozoNo ratings yet
- Postoperative Calcium Management in Same Day Discharge Thyroid and Parathyroid SurgeryDocument7 pagesPostoperative Calcium Management in Same Day Discharge Thyroid and Parathyroid Surgeryimran qaziNo ratings yet
- 10.1177 2192568217701914Document14 pages10.1177 2192568217701914richardson.gabrielNo ratings yet
- Journal of Ajog PDFDocument13 pagesJournal of Ajog PDFBima MahardhikaNo ratings yet
- Phlebology The Journal of Venous Disease 2016 MeissnerDocument8 pagesPhlebology The Journal of Venous Disease 2016 MeissnerPidchayathanakorn PaemikaNo ratings yet
- Frozen Section Library Gynecologic Pathology Intraoperative Consultation 2012 PGDocument253 pagesFrozen Section Library Gynecologic Pathology Intraoperative Consultation 2012 PGOlteanu Dragos-Nicolae100% (2)
- Distinguishing Reference Intervals and Clinical Decision Limits - A Review by The IFCC Committee On Reference Intervals and Decision LimitsDocument14 pagesDistinguishing Reference Intervals and Clinical Decision Limits - A Review by The IFCC Committee On Reference Intervals and Decision LimitsEmerson Ceras DávilaNo ratings yet
- Asccp 2006 Consensus GuidelinesDocument10 pagesAsccp 2006 Consensus GuidelinesDiana Lopera CastrillonNo ratings yet
- Hiperplasia EndometrialDocument12 pagesHiperplasia EndometrialJulián LópezNo ratings yet
- 11 Optimizing The Management 1598065529Document12 pages11 Optimizing The Management 1598065529César ArveláezNo ratings yet
- A Feasibility Study of EMFerlotinibmethotrexate5-fDocument2 pagesA Feasibility Study of EMFerlotinibmethotrexate5-fcgchaithanyaNo ratings yet
- Bile FistulaeDocument10 pagesBile FistulaesidehustlemrayNo ratings yet
- Awareness of The Association Between Obesity and PDocument5 pagesAwareness of The Association Between Obesity and PAditi RajputNo ratings yet
- pOSTOPERATIVE HYPOPARATHYROIDISM MANAGEMENTDocument12 pagespOSTOPERATIVE HYPOPARATHYROIDISM MANAGEMENTimran qaziNo ratings yet
- Oral Oncology: Mark K. Wax, James AzziDocument4 pagesOral Oncology: Mark K. Wax, James Azzicr89omfNo ratings yet
- Management of Fungal Infections in MCS and Cardiothoracic Organ Transplant Recipients: ISHLT Monograph Series (Volume 12)From EverandManagement of Fungal Infections in MCS and Cardiothoracic Organ Transplant Recipients: ISHLT Monograph Series (Volume 12)No ratings yet
- Hemorragia Tubo DigestivoDocument23 pagesHemorragia Tubo DigestivoNadia DeschampsNo ratings yet
- Woltering's New BookDocument265 pagesWoltering's New Bookapi-3775442No ratings yet
- Enfermedad Trofoblastica PDFDocument16 pagesEnfermedad Trofoblastica PDFGLORIA ANDREA ORJUELA FLOREZNo ratings yet
- Criterios Enfermedad Trofoblastica GestacionalDocument16 pagesCriterios Enfermedad Trofoblastica GestacionalKarina A. FloresNo ratings yet
- Dilemmas in ERCP: A Clinical CasebookFrom EverandDilemmas in ERCP: A Clinical CasebookDaniel K. MulladyNo ratings yet
- Viewcontent CgiDocument9 pagesViewcontent CgiBisakha DeyNo ratings yet
- Shunkwiler Et Al-2017-Journal of Clinical ApheresisDocument10 pagesShunkwiler Et Al-2017-Journal of Clinical ApheresisVenkata Sreekanth SampathNo ratings yet
- Guideline No. 392-Classification and Management of Endometrial HyperplasiDocument12 pagesGuideline No. 392-Classification and Management of Endometrial HyperplasiMagic_OverNo ratings yet
- Guidelines For The ApproMpriate Use of Bedside General and Cardiac Ultrasonography in The Evaluation of Critically Ill Patients-Part I. General Ultrasonography. Crit Care Med 2015Document24 pagesGuidelines For The ApproMpriate Use of Bedside General and Cardiac Ultrasonography in The Evaluation of Critically Ill Patients-Part I. General Ultrasonography. Crit Care Med 2015Andre ChavezNo ratings yet
- Imaging of Oncologic Emergencies What Every RadiolDocument23 pagesImaging of Oncologic Emergencies What Every RadiolJean Brando Torres GuerreroNo ratings yet
- Laryngoscope Investig Oto - 2021 - Goyal - Head and Neck Cancer Survivorship Consensus Statement From The American Head andDocument23 pagesLaryngoscope Investig Oto - 2021 - Goyal - Head and Neck Cancer Survivorship Consensus Statement From The American Head andEulalia JuanNo ratings yet
- ChouetalAPSASAASRAGuidelinesforManagementofPostoperativePain JofPain Feb 2016Document28 pagesChouetalAPSASAASRAGuidelinesforManagementofPostoperativePain JofPain Feb 2016nijad jabrNo ratings yet
- Clinical Practice Guideline: Benign Paroxysmal Positional Vertigo (Update)Document48 pagesClinical Practice Guideline: Benign Paroxysmal Positional Vertigo (Update)winnerfromparisNo ratings yet
- 2017 ACR Appropriateness Criteria Renal TrasplantDocument10 pages2017 ACR Appropriateness Criteria Renal TrasplantLiliana TorresNo ratings yet
- The Effects of Preoperative Embolization On Carotid Body Paraganglioma Surgery: A Systematic Review and Meta-AnalysisDocument8 pagesThe Effects of Preoperative Embolization On Carotid Body Paraganglioma Surgery: A Systematic Review and Meta-AnalysisNicolás HenaoNo ratings yet
- Fitzgerald 2020 American College of Rheumatology GDocument18 pagesFitzgerald 2020 American College of Rheumatology Gbc9j4n98djNo ratings yet
- Cheson (IWG) Criteria JCO 2007Document8 pagesCheson (IWG) Criteria JCO 2007atina putriNo ratings yet
- Jurnal Adenomiosis Dan MiomaDocument8 pagesJurnal Adenomiosis Dan Miomaperussi pranadiptaNo ratings yet
- What Exactly Is Patient SafetyDocument19 pagesWhat Exactly Is Patient Safetybe a doctor for you Medical studentNo ratings yet
- Innovations in Modern Endocrine SurgeryFrom EverandInnovations in Modern Endocrine SurgeryMichael C. SingerNo ratings yet
- ACR 2023 Lung RADSDocument16 pagesACR 2023 Lung RADSHaiNmNo ratings yet
- Atlas of Gynecologic Cytopathology With Histopathologic Correlations Full Chapter PDFDocument44 pagesAtlas of Gynecologic Cytopathology With Histopathologic Correlations Full Chapter PDFbaloshholber100% (8)
- SRS Radiation Therapy For Brain Metastases ASTRO GUIDELINES GONDI 22Document18 pagesSRS Radiation Therapy For Brain Metastases ASTRO GUIDELINES GONDI 22Pablo Castro PenaNo ratings yet
- Pi Is 0894731723005333Document62 pagesPi Is 0894731723005333ВалентинаNo ratings yet
- Treatment of Benign Prostatic Hyperplasia: Modern Alternative to Transurethral Resection of the ProstateFrom EverandTreatment of Benign Prostatic Hyperplasia: Modern Alternative to Transurethral Resection of the ProstateBilal ChughtaiNo ratings yet
- Tsao 2015Document26 pagesTsao 2015Ivan InkovNo ratings yet
- Livro Cirurgia Blumgarts Surgery of The Liver Biliary Tract and Pancreas William R Jarnagin Et Al Eds 6th Ed 2017Document2,402 pagesLivro Cirurgia Blumgarts Surgery of The Liver Biliary Tract and Pancreas William R Jarnagin Et Al Eds 6th Ed 2017lucasfacci100% (4)
- Morrison 2016Document22 pagesMorrison 2016Breno Mendes CardosoNo ratings yet
- Asco GCSF 2015Document16 pagesAsco GCSF 2015Alvy SyukrieNo ratings yet
- Chron I SubduralDocument9 pagesChron I Subduralelton fidelisNo ratings yet
- Otolaryngol - Head Neck Surg - 2014 - Al Khatib - Severe Vitamin D DeficiencyDocument8 pagesOtolaryngol - Head Neck Surg - 2014 - Al Khatib - Severe Vitamin D Deficiencyrohillak692No ratings yet
- Algoritma Dalam Penanganan TraumaDocument69 pagesAlgoritma Dalam Penanganan TraumaZulhida YuniNo ratings yet
- Rectal Cancer: International Perspectives on Multimodality ManagementFrom EverandRectal Cancer: International Perspectives on Multimodality ManagementBrian G. CzitoNo ratings yet
- Genomic Instability in Human Cancer: Molecular Insights and Opportunities For Therapeutic Attack and Prevention Through Diet and NutritionDocument21 pagesGenomic Instability in Human Cancer: Molecular Insights and Opportunities For Therapeutic Attack and Prevention Through Diet and NutritionedNo ratings yet
- 10.1016@S0140 67361932317 7Document11 pages10.1016@S0140 67361932317 7DaviSalmissonNo ratings yet
- ACR Appropriateness Criteria Palpable Abdominal MassSuspected NeoplasmDocument8 pagesACR Appropriateness Criteria Palpable Abdominal MassSuspected NeoplasmAgustinaNo ratings yet
- 1 s2.0 S0002838X21000885Document2 pages1 s2.0 S0002838X21000885henry hernandezNo ratings yet
- Dgab 512Document23 pagesDgab 512henry hernandezNo ratings yet
- References: Hyperthyroidism Due To Graves-Basedow Disease in A Woman Refractory To Thyroid HormonesDocument3 pagesReferences: Hyperthyroidism Due To Graves-Basedow Disease in A Woman Refractory To Thyroid Hormoneshenry hernandezNo ratings yet
- Fendo 11 00648Document29 pagesFendo 11 00648henry hernandezNo ratings yet
- Fendo 10 00766Document12 pagesFendo 10 00766henry hernandezNo ratings yet
- Alm 41 6 521Document11 pagesAlm 41 6 521henry hernandezNo ratings yet
- 2020 Article 623Document11 pages2020 Article 623henry hernandezNo ratings yet
- Management of Diabetes and Hyperglycemia in Hospitalized Patients Endotext NCBI BookshelfDocument21 pagesManagement of Diabetes and Hyperglycemia in Hospitalized Patients Endotext NCBI Bookshelfhenry hernandezNo ratings yet
- 1 PBDocument4 pages1 PBhenry hernandezNo ratings yet
- Therapeutics: Donal P Mclornan, Janet E Pope, Jason Gotlib, Claire N HarrisonDocument14 pagesTherapeutics: Donal P Mclornan, Janet E Pope, Jason Gotlib, Claire N Harrisonhenry hernandezNo ratings yet
- Genetic Determinants of Inherited Susceptibility To Hypercholesterolemia - A Comprehensive Literature ReviewDocument23 pagesGenetic Determinants of Inherited Susceptibility To Hypercholesterolemia - A Comprehensive Literature Reviewhenry hernandezNo ratings yet
- REWIND TrialDocument10 pagesREWIND Trialhenry hernandezNo ratings yet
- Management of Hyperglycemia and Enteral Nutrition in The Hospitalized PatientDocument8 pagesManagement of Hyperglycemia and Enteral Nutrition in The Hospitalized Patienthenry hernandezNo ratings yet
- LKPD - Recount Text 2Document2 pagesLKPD - Recount Text 2Sabian KalifiNo ratings yet
- Transtracheal Jet Ventilation: Learning ObjectivesDocument5 pagesTranstracheal Jet Ventilation: Learning ObjectivesRicardoNo ratings yet
- Oral Pathology Review List For NDEB With PicsDocument75 pagesOral Pathology Review List For NDEB With PicsBookwyrm AddictNo ratings yet
- Effect of Swedish Massage and Hot Mud With Calotropis Gigantea Application Among Knee Joint Osteoarthritis Cases-A Randomized Control TrialDocument5 pagesEffect of Swedish Massage and Hot Mud With Calotropis Gigantea Application Among Knee Joint Osteoarthritis Cases-A Randomized Control TrialIJAR JOURNALNo ratings yet
- Clinical Aspects of IVHDocument11 pagesClinical Aspects of IVHsteffiwpNo ratings yet
- Thoracic Outlet Syndrome Exercises IIDocument2 pagesThoracic Outlet Syndrome Exercises IIRiaz KhanNo ratings yet
- Basic Sciences QN PaperDocument29 pagesBasic Sciences QN PapermanorasmanthewNo ratings yet
- 6 - Immune Deficiency Diseases 2Document8 pages6 - Immune Deficiency Diseases 2Belle Galao GepteNo ratings yet
- TeamCare DentalDocument8 pagesTeamCare DentalHector FloydNo ratings yet
- Hemorrhoids, ParaproctitisDocument56 pagesHemorrhoids, ParaproctitisСандагсүрэн СандагдоржNo ratings yet
- Nhs Covid Pass - Vaccinated: Covid-19 Vaccine Astrazeneca Covid-19 Vaccine AstrazenecaDocument1 pageNhs Covid Pass - Vaccinated: Covid-19 Vaccine Astrazeneca Covid-19 Vaccine AstrazenecaSuzanne MurphyNo ratings yet
- MRI and CT Insufficiency Fractures of Pelvis and Proximal FemurDocument17 pagesMRI and CT Insufficiency Fractures of Pelvis and Proximal FemureosfieldNo ratings yet
- Migraine Treatment Guidelines (2019) PDFDocument2 pagesMigraine Treatment Guidelines (2019) PDFveerrajuNo ratings yet
- Effect of Single-Dose Antibiotic Prophylaxis Versus Conventional Antibiotic Therapy in Surgery A Randomized Controlled Trial in A Public Teaching HospitalDocument5 pagesEffect of Single-Dose Antibiotic Prophylaxis Versus Conventional Antibiotic Therapy in Surgery A Randomized Controlled Trial in A Public Teaching HospitalكنNo ratings yet
- EXPERTS AGAINST LOCKDOWN - Open Letter To An Taoiseach and Minister For HealthDocument6 pagesEXPERTS AGAINST LOCKDOWN - Open Letter To An Taoiseach and Minister For HealthPeterNo ratings yet
- PRM - Ma5 BookletDocument25 pagesPRM - Ma5 BookletVan LabasanoNo ratings yet
- Pharma S03 SBR01 Le1Document15 pagesPharma S03 SBR01 Le1sky vallartaNo ratings yet
- Infection Control in Burns PatietnsDocument41 pagesInfection Control in Burns Patietnstummalapalli venkateswara raoNo ratings yet
- Brochure v2Document2 pagesBrochure v2Keiran LeeNo ratings yet
- Instructions For Completing The CMS 1500 Claim FormDocument6 pagesInstructions For Completing The CMS 1500 Claim FormHarry CanabaNo ratings yet
- Medication and Treatment Sheet: Mariano Marcos Memorial Hospital and Medical CenterDocument4 pagesMedication and Treatment Sheet: Mariano Marcos Memorial Hospital and Medical CenterWyn AgustinNo ratings yet
- CestodesDocument4 pagesCestodesmrcveight100% (1)
- VheeeeDocument50 pagesVheeeeKathlene GamitNo ratings yet
- NCERT Exemplar Solution Class 8 Science Chapter 10 1Document12 pagesNCERT Exemplar Solution Class 8 Science Chapter 10 1Priyanka NegiNo ratings yet
- Fasting EnemaDocument108 pagesFasting Enemavskliris1100% (2)