Download as pdf or txt
You might also like
- Instant Download Ebook PDF Fundamentals of Abnormal Psychology 9th Edition PDF ScribdDocument47 pagesInstant Download Ebook PDF Fundamentals of Abnormal Psychology 9th Edition PDF Scribdjohn.aki332100% (46)
- 981-0602 Onan MDKUB MDKWB Spec E-J Install Manual (2-2010)Document65 pages981-0602 Onan MDKUB MDKWB Spec E-J Install Manual (2-2010)pepa 007No ratings yet
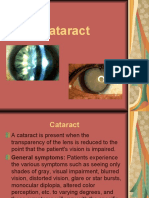
- Cataract PPT FinalDocument37 pagesCataract PPT FinalSibi John91% (23)
- Case Presentation On Peptic UlcerDocument62 pagesCase Presentation On Peptic UlcerRebekah Ann Puno95% (22)
- CataractDocument45 pagesCataractAmit Martin100% (3)
- CataractDocument50 pagesCataractApoorva Agrawal100% (3)
- Lens DiseaseDocument80 pagesLens Disease39 Akshit SetiaNo ratings yet
- Senile Cataract: DR SyedDocument28 pagesSenile Cataract: DR SyedShahzada KhanNo ratings yet
- Cataract: Antony Halim I4061162030Document50 pagesCataract: Antony Halim I4061162030Gilang PramanayudhaNo ratings yet
- Jewel June Gutierrez N-31 Rosejel Mae Lagura Senile Cataract IDocument4 pagesJewel June Gutierrez N-31 Rosejel Mae Lagura Senile Cataract IJewel GutierrezNo ratings yet
- Sree Teja-OphthalmologyDocument56 pagesSree Teja-OphthalmologysanjuNo ratings yet
- Ophthalmology - Diseases of VitreousDocument5 pagesOphthalmology - Diseases of VitreousjbtcmdtjjvNo ratings yet
- Terminology: Nuclear Sclerotic CataractsDocument4 pagesTerminology: Nuclear Sclerotic CataractsBenjamin NgNo ratings yet
- Сataract 09Document32 pagesСataract 09somebody_maNo ratings yet
- Dr. Md. Yeamli Khan: Mbbs (Dhaka) Do (Du) Fcps (Ophth)Document50 pagesDr. Md. Yeamli Khan: Mbbs (Dhaka) Do (Du) Fcps (Ophth)Kawshik SahaNo ratings yet
- Cataract: By: Reci Maulita I11110032Document74 pagesCataract: By: Reci Maulita I11110032Reci MaulitaNo ratings yet
- Peroperative Complications of Cataract Surgery: Jaidev Vishwa 3 Year Supplementary Roll No 11Document23 pagesPeroperative Complications of Cataract Surgery: Jaidev Vishwa 3 Year Supplementary Roll No 11jaidev vishwaNo ratings yet
- Adult Cataract: Cortical or Soft CataractDocument6 pagesAdult Cataract: Cortical or Soft CataractJohn Christopher LucesNo ratings yet
- KatarakDocument28 pagesKatarakBimo Nugroho SaktiNo ratings yet
- Ophthalmology - RetinaDocument15 pagesOphthalmology - RetinajbtcmdtjjvNo ratings yet
- Course 7 I, IIDocument17 pagesCourse 7 I, IItaliya. shvetzNo ratings yet
- Corneal DiseasesDocument55 pagesCorneal DiseasesShally GuptaNo ratings yet
- UNIVERSITY OF MEDICAL SCIENCES"REZONANCA"-Halil Ajvazi/Ophthalmology/Prishtina/Republic of KosovaDocument98 pagesUNIVERSITY OF MEDICAL SCIENCES"REZONANCA"-Halil Ajvazi/Ophthalmology/Prishtina/Republic of KosovaHALIL Z.AJVAZI100% (1)
- Senile Cataract (Age-Related Cataract) : Practice Essentials, Background, PathophysiologyDocument6 pagesSenile Cataract (Age-Related Cataract) : Practice Essentials, Background, PathophysiologyadliahghaisaniNo ratings yet
- PSSS-Mata Tenang Visus Turun PerlahanDocument48 pagesPSSS-Mata Tenang Visus Turun PerlahanYesi 'faiqa Putir100% (1)
- Katara KDocument4 pagesKatara KAmirah Jihan AfryNo ratings yet
- Ophthalmology Neuro OphthalmologyDocument7 pagesOphthalmology Neuro OphthalmologyjbtcmdtjjvNo ratings yet
- Chapter 10. DoneDocument42 pagesChapter 10. DoneAndi Ayu LestariNo ratings yet
- Document From Sham301994Document128 pagesDocument From Sham301994sham301994No ratings yet
- Cataract: BY: Huda Hamdan Rubaalsheyab Maramalanbar AbeerhussainDocument59 pagesCataract: BY: Huda Hamdan Rubaalsheyab Maramalanbar AbeerhussainaliNo ratings yet
- Cataract - Dr. Nameera TabassumDocument12 pagesCataract - Dr. Nameera TabassumDR.NAMEERA TABASSUMNo ratings yet
- Ophthalmology - Diseases of Sclera and Uveal TractDocument15 pagesOphthalmology - Diseases of Sclera and Uveal TractjbtcmdtjjvNo ratings yet
- CataractDocument63 pagesCataractMutti KakarNo ratings yet
- Pearls in PPCDocument5 pagesPearls in PPCRajinder Kumar BassanNo ratings yet
- Bo 402 (32301721022)Document8 pagesBo 402 (32301721022)AvinabaNo ratings yet
- Diskusi Topik - Ali Mustagi - Mata Normal Visus Turun PerlahanDocument73 pagesDiskusi Topik - Ali Mustagi - Mata Normal Visus Turun PerlahanalimustagialgiNo ratings yet
- 2b.lens and CataractDocument3 pages2b.lens and CataractNayan MaharjanNo ratings yet
- Cataracts: ClassificationDocument9 pagesCataracts: ClassificationRafay ChacharNo ratings yet
- Cataract: Done by Mo3taz Abu Rabiah A7mad LubaniDocument46 pagesCataract: Done by Mo3taz Abu Rabiah A7mad LubaniMaxwell C Jay KafwaniNo ratings yet
- Cataract ReportDocument59 pagesCataract ReportRuDy RaviNo ratings yet
- Management of CataractDocument25 pagesManagement of Cataractapi-3742497No ratings yet
- Lens For Undergraduate 2022 Part 2Document64 pagesLens For Undergraduate 2022 Part 2Abdelmonem HamedNo ratings yet
- Cataract: Done by Jony MallikDocument46 pagesCataract: Done by Jony MallikAlfa Suryani ArdliNo ratings yet
- Eor CataractDocument3 pagesEor CataractDaneva ReyesNo ratings yet
- 00 Opthalmology - 111519Document54 pages00 Opthalmology - 111519Davis MasuguNo ratings yet
- Chronic Visual LossDocument7 pagesChronic Visual LossJim Jose AntonyNo ratings yet
- GlaucomaDocument24 pagesGlaucomaRakeshNo ratings yet
- Ophthalmology: Anatomy of The LensDocument35 pagesOphthalmology: Anatomy of The Lensمحمد عبدالوهاب ابراهيم الطباطبائيNo ratings yet
- Ectatic ConditionsDocument11 pagesEctatic ConditionsShuvashishSunuwarNo ratings yet
- 7 Lens and Cataract 1Document57 pages7 Lens and Cataract 1Devi Melissa RiupassaNo ratings yet
- Ocular EmergenciesDocument26 pagesOcular EmergenciesYukianesa100% (1)
- Disorders of The LensDocument117 pagesDisorders of The LensLavanya MadabushiNo ratings yet
- Senile CataractDocument56 pagesSenile Cataractamraayman21No ratings yet
- CATARACTDocument39 pagesCATARACTpullboy1No ratings yet
- Presentation 2Document57 pagesPresentation 2medhanit anjuloNo ratings yet
- Seminar On Optic AtrophyDocument50 pagesSeminar On Optic Atrophygmc,bhopal100% (1)
- Mata Tenang Visus Turun MendadakDocument74 pagesMata Tenang Visus Turun MendadakYeni AnggrainiNo ratings yet
- Common Ocular EmergenciesDocument33 pagesCommon Ocular EmergenciesMaimoona AimanNo ratings yet
- Glaucoma 2 Lecture PACG MBBS BY Prof Munim SuriDocument28 pagesGlaucoma 2 Lecture PACG MBBS BY Prof Munim SuriMunim SuriNo ratings yet
- Cataract NotesDocument4 pagesCataract NotesJeremy LauNo ratings yet
- Pemicu 1 PENGINDRAAN C2Document113 pagesPemicu 1 PENGINDRAAN C2CcNo ratings yet
- Lymphatic System: Presented byDocument55 pagesLymphatic System: Presented bySHAIK SHABEENA100% (1)
- 1 s2.0 S1475491615000764 MainDocument8 pages1 s2.0 S1475491615000764 MainaishaNo ratings yet
- Biocompatability of Dental Materials.Document93 pagesBiocompatability of Dental Materials.vadlamudi chakradhar100% (2)
- This Audio Is Used For The Transcriber Test at GoTranscriptDocument3 pagesThis Audio Is Used For The Transcriber Test at GoTranscriptMJ HashmiNo ratings yet
- Ethics in Social Research 2 (Postgraduate) PDFDocument28 pagesEthics in Social Research 2 (Postgraduate) PDFshidaNo ratings yet
- Let's Make The City Clean and FreshDocument17 pagesLet's Make The City Clean and FreshliaNo ratings yet
- Introduction To Internal Medicine - PPTMDocument30 pagesIntroduction To Internal Medicine - PPTMAddyNo ratings yet
- Nutritiona L Disorders: Paulette Benjamin-Chin MD Diplomate, Philippine Pediatric SocietyDocument102 pagesNutritiona L Disorders: Paulette Benjamin-Chin MD Diplomate, Philippine Pediatric SocietygailNo ratings yet
- Failures in FPDDocument30 pagesFailures in FPDMayank Aggarwal100% (1)
- Pe Grade9 QTR1 Module1Document37 pagesPe Grade9 QTR1 Module1Jp DiolaNo ratings yet
- General Form No 86 Health ExaminationDocument1 pageGeneral Form No 86 Health ExaminationIvy Chezka HallegadoNo ratings yet
- LincolnWeld 860 FluxDocument25 pagesLincolnWeld 860 FluxPubcrawlNo ratings yet
- Before You Proceed : Crisis ManagementDocument15 pagesBefore You Proceed : Crisis ManagementHarvey T. Dato-on100% (1)
- Product Name: New Zealand Data Sheet Apo-PrednisoneDocument13 pagesProduct Name: New Zealand Data Sheet Apo-PrednisonedomNo ratings yet
- Soal PAS Bhs Inggris (9) ganjil..MAMAS.SDocument3 pagesSoal PAS Bhs Inggris (9) ganjil..MAMAS.SAmsenoNo ratings yet
- 412 Lecture 1 3 Introduction To PathogenesisDocument49 pages412 Lecture 1 3 Introduction To PathogenesisAnik Saha Toni 1912619643No ratings yet
- Examen Comprension Ingles MedicoDocument16 pagesExamen Comprension Ingles MedicoBM BonillaNo ratings yet
- Anti-Thyroid DrugsDocument60 pagesAnti-Thyroid DrugsApurba Sarker Apu100% (1)
- Affections of HornDocument28 pagesAffections of HornNaveen BasudeNo ratings yet
- Stanford Ortho CurriculumDocument13 pagesStanford Ortho CurriculumGyörgy FabianNo ratings yet
- Patient-Reported Outcome Measures For Angioedema: A Literature ReviewDocument5 pagesPatient-Reported Outcome Measures For Angioedema: A Literature Review7dsp7xvs8dNo ratings yet
- ABG ExamplesDocument31 pagesABG ExamplesKEROLOS MAHROUSNo ratings yet
- NCP Ortho WardDocument2 pagesNCP Ortho WardAira MaeNo ratings yet
- Cordyceps Militaris Enhances Cell-Mediated Immunity in Healthy Korean MenDocument9 pagesCordyceps Militaris Enhances Cell-Mediated Immunity in Healthy Korean MenNhung Nguyễn Thị HồngNo ratings yet
- Antinuclear Antibodies: When To Test and How To Interpret FindingsDocument4 pagesAntinuclear Antibodies: When To Test and How To Interpret FindingsFariz NurNo ratings yet
- Relationship Between Body Image and Self EsteemDocument36 pagesRelationship Between Body Image and Self EsteemHuzaifah Bin Saeed85% (20)
- Phimosisparaphimosiscircumcision 221122055651 b84b84c6Document65 pagesPhimosisparaphimosiscircumcision 221122055651 b84b84c6Prashant KumarNo ratings yet