Download as docx, pdf, or txt
You might also like
- DIY MAP Your Soul Plan Chart: T/DR Markus Van Der WesthuizenDocument14 pagesDIY MAP Your Soul Plan Chart: T/DR Markus Van Der WesthuizenValentin Mihai100% (4)
- Nurse in The National and Global Health Care Delivery SystemDocument9 pagesNurse in The National and Global Health Care Delivery Systemczeremar chanNo ratings yet
- PayU - Sales DeckDocument27 pagesPayU - Sales DeckaNANTNo ratings yet
- The Doctor Said Formula Would Help Me Health Sector Influences On Use of Infant Formula in Peri-Urban Lima, PeruDocument13 pagesThe Doctor Said Formula Would Help Me Health Sector Influences On Use of Infant Formula in Peri-Urban Lima, PeruNisarg PatelNo ratings yet
- Access Barriers of Infertility Services For Urban and Rural PatientsDocument9 pagesAccess Barriers of Infertility Services For Urban and Rural PatientssridewiNo ratings yet
- BD Study 2Document11 pagesBD Study 2Amra DujoneNo ratings yet
- Mental Health Impact On The Unmet Need For Family Planning and Fertility Rate in Rural Ethiopia: A Population-Based Cohort StudyDocument10 pagesMental Health Impact On The Unmet Need For Family Planning and Fertility Rate in Rural Ethiopia: A Population-Based Cohort Studydiya desaiNo ratings yet
- jcpp2613 PDFDocument22 pagesjcpp2613 PDFJorge Fernández BaluarteNo ratings yet
- Determinan Faktor JurnalDocument7 pagesDeterminan Faktor Jurnalhilan sasewaNo ratings yet
- Bab 2Document15 pagesBab 2Its4peopleNo ratings yet
- Ebb PDFDocument12 pagesEbb PDFMonica TanNo ratings yet
- Mansfield 2021Document17 pagesMansfield 2021Adam HafizNo ratings yet
- Riumallo Herl2019Document16 pagesRiumallo Herl2019Satria BuanaNo ratings yet
- Adol - Income y Salud MentalDocument11 pagesAdol - Income y Salud Mentalaaa hhhNo ratings yet
- 613 3577 1 PBDocument12 pages613 3577 1 PBArina DygaNo ratings yet
- Health & PlaceDocument10 pagesHealth & PlaceBeatriz Elena JaramilloNo ratings yet
- Stunting Inj Childhood An Overview of Global Burden, Trends, Determinants, and Driver of DeclinesDocument15 pagesStunting Inj Childhood An Overview of Global Burden, Trends, Determinants, and Driver of DeclinesMichimichi 78No ratings yet
- Knerr Gardner Cluver - Parenting Systematic ReviewDocument13 pagesKnerr Gardner Cluver - Parenting Systematic ReviewVinod K PillaiNo ratings yet
- Pgda WP 69Document19 pagesPgda WP 69tasya tazkia regita zahraNo ratings yet
- Written Public Health Ll. U2Document7 pagesWritten Public Health Ll. U2Adanigbo MagretNo ratings yet
- Bond 2021Document23 pagesBond 2021Cen GdNo ratings yet
- 1-5 CombineDocument72 pages1-5 CombineDan Agyemang NketiahNo ratings yet
- Trends in Socioeconomic Inequalities in Child Malnutrition in Vietnam: Findings From The Multiple Indicator Cluster Surveys, 2000 2011Document9 pagesTrends in Socioeconomic Inequalities in Child Malnutrition in Vietnam: Findings From The Multiple Indicator Cluster Surveys, 2000 2011Vu Duy KienNo ratings yet
- Ill-Health and Poverty A Literature Review On Health in Informal SettlementsDocument10 pagesIll-Health and Poverty A Literature Review On Health in Informal Settlementsc5m07hh9No ratings yet
- AJAN 25-2 Massey PDFDocument5 pagesAJAN 25-2 Massey PDFBOBNo ratings yet
- Strengthening Health Information Systems To Address Health Equity ChallengesDocument16 pagesStrengthening Health Information Systems To Address Health Equity ChallengesAhlidin S.No ratings yet
- 17.321.2687 Ni Komang Sri WahyuniDocument19 pages17.321.2687 Ni Komang Sri Wahyunigekayu sartikaNo ratings yet
- SSM - Population Health: Muhammad Fikru Rizal, Eddy Van DoorslaerDocument10 pagesSSM - Population Health: Muhammad Fikru Rizal, Eddy Van DoorslaerRamadhan Dwi PrasetyoNo ratings yet
- Thesis RRL REFERENCEDocument3 pagesThesis RRL REFERENCEMAY ANN ROSE CASERNo ratings yet
- Individual Correlates of Sleep Among Childbearing Women CanadaDocument13 pagesIndividual Correlates of Sleep Among Childbearing Women Canadachristiancraig1987No ratings yet
- Grant ProposalDocument34 pagesGrant Proposalapi-547026973No ratings yet
- Critical Analysis of Health Inequalities ReportDocument14 pagesCritical Analysis of Health Inequalities ReportDamie OjoNo ratings yet
- Hosseinpoor 2011Document7 pagesHosseinpoor 2011PHC WuyanNo ratings yet
- The Impact of Living With Klinefelter Syndrome: A Qualitative Exploration of Adolescents and AdultsDocument10 pagesThe Impact of Living With Klinefelter Syndrome: A Qualitative Exploration of Adolescents and AdultsصادقNo ratings yet
- OpftdDocument18 pagesOpftdgyztantika patadunganNo ratings yet
- Cross SectionalDocument10 pagesCross Sectionaldzakiyatul fahmiNo ratings yet
- HIV AIDS Research Papers 2008 2009Document5 pagesHIV AIDS Research Papers 2008 2009Sneha NagvekarNo ratings yet
- Puberty Blockers For Children Can They ConsentDocument25 pagesPuberty Blockers For Children Can They Consentnina.konekoNo ratings yet
- Essential Childhood Immunization in 43 Low - and Middle-Income Countries - Analysis of Spatial Trends and Socioeconomic Inequalities in Vaccine Coverage - PLOS MedicineDocument13 pagesEssential Childhood Immunization in 43 Low - and Middle-Income Countries - Analysis of Spatial Trends and Socioeconomic Inequalities in Vaccine Coverage - PLOS MedicineIhsan Ullah HimmatNo ratings yet
- Critical Caring Theory and Public Health Nursing Advocacy For Comprehensive Sexual Health EducationDocument7 pagesCritical Caring Theory and Public Health Nursing Advocacy For Comprehensive Sexual Health EducationCurico MysecretgardenNo ratings yet
- Family Support or Social Support? The Role of Clan Culture: Chuanchuan ZhangDocument21 pagesFamily Support or Social Support? The Role of Clan Culture: Chuanchuan ZhangArianeNo ratings yet
- Jawad Et Al - 2021 - Implications of Armed Conflict For Maternal and Child HealthDocument18 pagesJawad Et Al - 2021 - Implications of Armed Conflict For Maternal and Child HealthIvan OliveiraNo ratings yet
- Socio-Economic Determinants of Maternal Healthcare Behaviour Evidence From PakistanDocument24 pagesSocio-Economic Determinants of Maternal Healthcare Behaviour Evidence From PakistanTuba MustafaNo ratings yet
- Literature Review On Infant Mortality RateDocument4 pagesLiterature Review On Infant Mortality Rateaflsjfmwh100% (1)
- Agwaga Flobel Chap 1Document25 pagesAgwaga Flobel Chap 1davidtitangohNo ratings yet
- 1 PBDocument16 pages1 PBYoya LoyaNo ratings yet
- VasavanSharangi Assign1Document4 pagesVasavanSharangi Assign1sharangiivNo ratings yet
- Literature Review On StillbirthDocument6 pagesLiterature Review On Stillbirthaflsvagfb100% (1)
- Article Ghanien - Food-Se - Nut - Weaizereyesus2017Document20 pagesArticle Ghanien - Food-Se - Nut - Weaizereyesus2017Mbebou MidassNo ratings yet
- Östlin - Paying Attention To GenderDocument6 pagesÖstlin - Paying Attention To GendermariaconstanzavasqueNo ratings yet
- JosephDocument4 pagesJosephAtom GutomNo ratings yet
- Association Between Nutrient Intake and Female Infertility A Study Based On NHANES DatabaseDocument11 pagesAssociation Between Nutrient Intake and Female Infertility A Study Based On NHANES DatabaseReena SapruNo ratings yet
- Attachment 1 PDFDocument5 pagesAttachment 1 PDFAninditta PutriNo ratings yet
- JURNAL International Journal of Humanities and Social Science InventionDocument15 pagesJURNAL International Journal of Humanities and Social Science InventionyarmimiNo ratings yet
- Soc 1Document14 pagesSoc 1api-577249675No ratings yet
- Causes of Inequality in HealthDocument20 pagesCauses of Inequality in HealthLisaNo ratings yet
- Children and Youth Services Review: Anthony G OmezDocument11 pagesChildren and Youth Services Review: Anthony G OmezNadia Cenat CenutNo ratings yet
- Negative Maternal Outcomes Whites Vs BlacksDocument14 pagesNegative Maternal Outcomes Whites Vs Blacksapi-679552755No ratings yet
- "You Don't Trust A Government Vaccine" - Narratives of Institutional Trust and Influenza Vaccination Among African American and White AdultsDocument8 pages"You Don't Trust A Government Vaccine" - Narratives of Institutional Trust and Influenza Vaccination Among African American and White AdultsSuha BabaNo ratings yet
- Hearing LossDocument10 pagesHearing LossAndreaNo ratings yet
- Jvad 025Document39 pagesJvad 025oakpacificNo ratings yet
- Cook, C. E., & Décary, S. (2020) - Higher Order Thinking About Differential Diagnosis. Brazilian Journal of Physical Therapy, 24 (1), 1-7Document1 pageCook, C. E., & Décary, S. (2020) - Higher Order Thinking About Differential Diagnosis. Brazilian Journal of Physical Therapy, 24 (1), 1-7Yaumil FauziahNo ratings yet
- 1 s2.0 S0213911121002776 MainDocument3 pages1 s2.0 S0213911121002776 MainYaumil FauziahNo ratings yet
- 1 s2.0 S0946672X21001668 MainDocument5 pages1 s2.0 S0946672X21001668 MainYaumil FauziahNo ratings yet
- 1 LefletDocument12 pages1 LefletYaumil FauziahNo ratings yet
- EJCM - Volume 36 - Issue 1 - Pages 45-60-1Document16 pagesEJCM - Volume 36 - Issue 1 - Pages 45-60-1Yaumil FauziahNo ratings yet
- Islam2018 Article RiskFactorsOfStuntingAmongChilDocument13 pagesIslam2018 Article RiskFactorsOfStuntingAmongChilYaumil FauziahNo ratings yet
- English Policy Paper StuntingDocument82 pagesEnglish Policy Paper StuntingYaumil FauziahNo ratings yet
- Ijerph 18 07644Document8 pagesIjerph 18 07644Yaumil FauziahNo ratings yet
- Gibson - Erika - 201911 - MSC - ThesisDocument78 pagesGibson - Erika - 201911 - MSC - ThesisYaumil FauziahNo ratings yet
- 30.D18 788 Winny Yohana Indonesia-3-1Document4 pages30.D18 788 Winny Yohana Indonesia-3-1Yaumil FauziahNo ratings yet
- 25-Article Text-177-2-10-20211231Document7 pages25-Article Text-177-2-10-20211231Yaumil FauziahNo ratings yet
- 10 1108 - JHR 05 2019 0095Document9 pages10 1108 - JHR 05 2019 0095Yaumil FauziahNo ratings yet
- 30 +JANH+V4N1+ce2+16-22Document8 pages30 +JANH+V4N1+ce2+16-22Yaumil FauziahNo ratings yet
- Bogin - Reply Stunting Is Not A Synonym of Malnutrition20191025 - BBDocument4 pagesBogin - Reply Stunting Is Not A Synonym of Malnutrition20191025 - BBYaumil FauziahNo ratings yet
- s12889 020 08869 1Document87 pagess12889 020 08869 1Yaumil FauziahNo ratings yet
- Underweigh Wasting and Stunting in LMICs JIDR RevisedDocument21 pagesUnderweigh Wasting and Stunting in LMICs JIDR RevisedYaumil FauziahNo ratings yet
- Journal Pone 0264010Document15 pagesJournal Pone 0264010Yaumil FauziahNo ratings yet
- DANCE PPT For RizalDocument40 pagesDANCE PPT For RizalAngelica perezNo ratings yet
- EPANET in QGIS Framework: The QEPANET PluginDocument5 pagesEPANET in QGIS Framework: The QEPANET PluginAleksandar PetrovićNo ratings yet
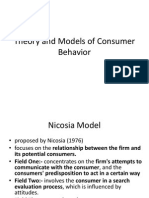
- Theory and Models of Consumer BehaviorDocument28 pagesTheory and Models of Consumer BehaviorNK ShresthaNo ratings yet
- Case Study 1Document7 pagesCase Study 1harishma hsNo ratings yet
- TTL - Lesson Plan - Harvey - IbeDocument12 pagesTTL - Lesson Plan - Harvey - IbeHarvey Kurt IbeNo ratings yet
- Look At, See or Watch - English Grammar Today - Cambridge Dictionary PDFDocument220 pagesLook At, See or Watch - English Grammar Today - Cambridge Dictionary PDFMadhur BhutraNo ratings yet
- Social Media and Political Communication in India: An Analysis of 2017 Legislative Assembly Elections in Himachal PradeshDocument7 pagesSocial Media and Political Communication in India: An Analysis of 2017 Legislative Assembly Elections in Himachal PradeshEditor IJTSRDNo ratings yet
- Art 20199983Document3 pagesArt 20199983Devaki SubasriNo ratings yet
- Admission Form Eleven Class Mar 2016Document3 pagesAdmission Form Eleven Class Mar 2016Aaqib AliNo ratings yet
- Self Affirmation ScaleDocument19 pagesSelf Affirmation ScaleQonitah Arya SulthanahNo ratings yet
- Visual Representation of Metaphor SF ApproachDocument17 pagesVisual Representation of Metaphor SF ApproachramNo ratings yet
- HR Policies ProjectDocument70 pagesHR Policies ProjectrmburraNo ratings yet
- Module 4 - Ignition Systems - QSK60GDocument18 pagesModule 4 - Ignition Systems - QSK60GMuhammad Ishfaq100% (1)
- NIOS Painting Chapter 4Document9 pagesNIOS Painting Chapter 4Samuel ThomasNo ratings yet
- GT Gold Corp.: Release Date: 25 June 2020Document12 pagesGT Gold Corp.: Release Date: 25 June 2020anon analyticsNo ratings yet
- ICGSE Y8 Maths Progression Test Mid-Year (Chapter1-11)Document10 pagesICGSE Y8 Maths Progression Test Mid-Year (Chapter1-11)YAP LEE KHIMNo ratings yet
- PURELL® Hand Sanitizer Gel: Safety Data SheetDocument14 pagesPURELL® Hand Sanitizer Gel: Safety Data SheetOmid BeygiNo ratings yet
- Vocabulary and Picture Prompts For Language Teaching Book 2 PDFDocument72 pagesVocabulary and Picture Prompts For Language Teaching Book 2 PDFmartinan100% (1)
- A Project Report-1 - 231020 - 204422Document59 pagesA Project Report-1 - 231020 - 204422Ankit Sharma 028No ratings yet
- English Trial 2017 SBP P1+P2 (Answer Scheme)Document14 pagesEnglish Trial 2017 SBP P1+P2 (Answer Scheme)Tan Zhen Xin100% (1)
- Tesla Manufacturing Plant in Canada AnnouncementDocument1 pageTesla Manufacturing Plant in Canada AnnouncementMaria MeranoNo ratings yet
- People vs. Subingsubing G.R. Nos. 104942-43 November 25, 1993Document13 pagesPeople vs. Subingsubing G.R. Nos. 104942-43 November 25, 1993Felix Leonard NovicioNo ratings yet
- Withdrawal Symptoms in The Golden TriangleDocument100 pagesWithdrawal Symptoms in The Golden TrianglePugh JuttaNo ratings yet
- Business Continuity Planning ChecklistDocument2 pagesBusiness Continuity Planning ChecklistShawn AmeliNo ratings yet
- Universiti Tunku Abdul Rahman: UEME1323 StaticsDocument26 pagesUniversiti Tunku Abdul Rahman: UEME1323 StaticsshintanNo ratings yet
- Setting MikrotikDocument10 pagesSetting MikrotikLambace KecciNo ratings yet
- Mike Millmore - CHP 7. Strategic Human Resource Planning The Weakest LinkDocument40 pagesMike Millmore - CHP 7. Strategic Human Resource Planning The Weakest LinkAndyHNo ratings yet
- (PRINTED NA) 2019chess Club ReportDocument6 pages(PRINTED NA) 2019chess Club ReportDarhil BroniolaNo ratings yet