Download as pdf or txt
You might also like
- The Unseen Side of Pregnancy: Non-Communicable Diseases and Maternal HealthDocument28 pagesThe Unseen Side of Pregnancy: Non-Communicable Diseases and Maternal HealthThe Wilson Center100% (2)
- Private Health Institutions LawDocument22 pagesPrivate Health Institutions LawShankar Sanyal100% (1)
- CPG On CsomDocument8 pagesCPG On CsomRobert Ross DulayNo ratings yet
- Nstemi PathoDocument2 pagesNstemi PathoSheana TmplNo ratings yet
- 101 Things I Wish I'd Known When I Started Using Hypnosis: Dabney EwinDocument17 pages101 Things I Wish I'd Known When I Started Using Hypnosis: Dabney EwinFilipeCarvalho100% (7)
- Preeclampsia An Obstetrician's Perspective - XackdDocument10 pagesPreeclampsia An Obstetrician's Perspective - XackdLiz Valentina Jordan MoyaNo ratings yet
- Early Pregnancy Cardio Metabolic Risk FactorsDocument11 pagesEarly Pregnancy Cardio Metabolic Risk FactorsPisces GurlNo ratings yet
- NIH Public Access: Pregnancy Complications and The Risk of Metabolic Syndrome For The OffspringDocument12 pagesNIH Public Access: Pregnancy Complications and The Risk of Metabolic Syndrome For The OffspringTika Renwarin Tua ElNo ratings yet
- Intl J Gynecology Obste - 2023 - Adam - Pregnancy As An Opportunity To Prevent Type 2 Diabetes Mellitus FIGO BestDocument12 pagesIntl J Gynecology Obste - 2023 - Adam - Pregnancy As An Opportunity To Prevent Type 2 Diabetes Mellitus FIGO BestDWI FAJAR MUTIARANo ratings yet
- Sari Paper EnglishDocument8 pagesSari Paper EnglishSariPuspitaNo ratings yet
- Dr. Dr. Nugrahanti - PITFM23 PDFDocument24 pagesDr. Dr. Nugrahanti - PITFM23 PDFDarameutia obgynNo ratings yet
- Febriyanti M. AdamDocument23 pagesFebriyanti M. AdamRinda UnoNo ratings yet
- 17 Epidemiology, Risk Factors, and Perinatal Outcomes ofDocument14 pages17 Epidemiology, Risk Factors, and Perinatal Outcomes ofromeeosbleedingNo ratings yet
- Jurnal KilkenyDocument11 pagesJurnal Kilkenynurrahmi auliaNo ratings yet
- Article 10.1111/tog.12600 PDFDocument8 pagesArticle 10.1111/tog.12600 PDFKeeranmayeeishraNo ratings yet
- Tseng Et Al 2022 Severe Maternal Morbidity in Pregnancies Complicated by Fetal Congenital Heart DiseaseDocument10 pagesTseng Et Al 2022 Severe Maternal Morbidity in Pregnancies Complicated by Fetal Congenital Heart DiseaseUMAE GINENo ratings yet
- Macrosomia Clinical Presentation History, Physical Examination, ComplicationsDocument1 pageMacrosomia Clinical Presentation History, Physical Examination, ComplicationsRizka AmeliaNo ratings yet
- Risks of Contraception and Pregnancy in Heart Disease: Sara Thorne, Anne Macgregor, Catherine Nelson-PiercyDocument6 pagesRisks of Contraception and Pregnancy in Heart Disease: Sara Thorne, Anne Macgregor, Catherine Nelson-PiercymazidampNo ratings yet
- Clinmed 17 3 251Document7 pagesClinmed 17 3 251nurulmhidayatNo ratings yet
- Dines 2020 ACKD Hypertensive Disorders of PregnancyDocument9 pagesDines 2020 ACKD Hypertensive Disorders of PregnancyBCR ABLNo ratings yet
- 1 s2.0 S2666668520300495 MainDocument7 pages1 s2.0 S2666668520300495 MainHadikagusti AdoraNo ratings yet
- Update On Medical Disorders in Pregnancy An Issue of Obstetrics and Gynecology Clinics The Clinics Internal MedicineDocument217 pagesUpdate On Medical Disorders in Pregnancy An Issue of Obstetrics and Gynecology Clinics The Clinics Internal Medicinemeriatmaja100% (1)
- Sibai Lancet Review PreeclampsiaDocument15 pagesSibai Lancet Review Preeclampsiaannoying_little_prankster9134No ratings yet
- Jurnal CohortDocument21 pagesJurnal CohortAstri Anindita UtomoNo ratings yet
- PIIS2468024922013584Document16 pagesPIIS2468024922013584Annette ChavezNo ratings yet
- Jurnal Abrupsio PlasentaDocument13 pagesJurnal Abrupsio Plasentaperussi pranadiptaNo ratings yet
- AbruptionDocument13 pagesAbruptionMauricio Lopez MejiaNo ratings yet
- Leslie V FarlandDocument10 pagesLeslie V FarlandtiaranindyNo ratings yet
- Medicina 59 01139Document10 pagesMedicina 59 01139ade lydia br.siregarNo ratings yet
- JWH 2020 8860Document8 pagesJWH 2020 8860Armelia ShafiraNo ratings yet
- Fasceite Necrosante em GravidastegravidezDocument12 pagesFasceite Necrosante em GravidastegravidezMarcelly EirasNo ratings yet
- Prakonsepsi 3Document10 pagesPrakonsepsi 3Isna WatiNo ratings yet
- A Review of The Pathophysiology and Management of Diabetes in PregnancyDocument13 pagesA Review of The Pathophysiology and Management of Diabetes in Pregnancyfelipe_duran_scribdNo ratings yet
- Smith 2015 Epigenetic and Developmental Influences On The Risk of Obesity, Diabetes and MsDocument8 pagesSmith 2015 Epigenetic and Developmental Influences On The Risk of Obesity, Diabetes and MsPaul SimononNo ratings yet
- Preeclampsia and DiabetesDocument16 pagesPreeclampsia and DiabetesJesslynBernadetteNo ratings yet
- Comprehensive Evaluation of Pregnancy Complications at A Tertiary Care Teaching HospitalDocument9 pagesComprehensive Evaluation of Pregnancy Complications at A Tertiary Care Teaching HospitalIJAR JOURNALNo ratings yet
- Effect - of - Fetal - and - Child - Health Hypertention Cardiovask Risk KidneyDocument12 pagesEffect - of - Fetal - and - Child - Health Hypertention Cardiovask Risk KidneyNia Prajnya SyailendraNo ratings yet
- AbruptionDocument13 pagesAbruptionAnghelo Aldair Velásquez CarrilloNo ratings yet
- Maternal Obesity 2Document13 pagesMaternal Obesity 2lalimdNo ratings yet
- Fetal Origin of Adult Disease: New HorizonsDocument5 pagesFetal Origin of Adult Disease: New HorizonsHervi LaksariNo ratings yet
- Jcem 1664Document9 pagesJcem 1664R. WadlowNo ratings yet
- De Boo Barker HypothesisDocument11 pagesDe Boo Barker HypothesisIamJmlingconNo ratings yet
- Cystic Fibrosis and PregnancyDocument2 pagesCystic Fibrosis and Pregnancyscience world publishingNo ratings yet
- Endocrine Disorders During Pregnancy 2006Document223 pagesEndocrine Disorders During Pregnancy 2006STEPHANIE TALILAHNo ratings yet
- Repub 103040-OaDocument8 pagesRepub 103040-OaEmma Lyn SantosNo ratings yet
- Early Predictors For Hypertensive Disorders of Pregnancy in Developing CountriesDocument12 pagesEarly Predictors For Hypertensive Disorders of Pregnancy in Developing CountriesBayna Lestari LubisNo ratings yet
- Knowledge of Preeclampsia and Its Associated FactoDocument5 pagesKnowledge of Preeclampsia and Its Associated FactoarreyemilieneNo ratings yet
- Acog Practice Bulletin: Pregnancy and Heart DiseaseDocument37 pagesAcog Practice Bulletin: Pregnancy and Heart Diseasereham mohamedNo ratings yet
- GimikDocument9 pagesGimikNanda PuspitaNo ratings yet
- Recent Advances in The Prevention and Screening of PreeclampsiaDocument17 pagesRecent Advances in The Prevention and Screening of PreeclampsialacrymosamyNo ratings yet
- New Aspects in The Pathophysiology of Preeclampsia: Clinical ScienceDocument27 pagesNew Aspects in The Pathophysiology of Preeclampsia: Clinical Sciencenaumee100% (2)
- Hypertensive Disorders of Pregnancy: Case Definitions & Guidelines For Data Collection, Analysis, and Presentation of Immunization Safety DataDocument8 pagesHypertensive Disorders of Pregnancy: Case Definitions & Guidelines For Data Collection, Analysis, and Presentation of Immunization Safety DataRachmad SammuliaNo ratings yet
- Management of Preexisting Diabetes in Pregnancy 2019Document9 pagesManagement of Preexisting Diabetes in Pregnancy 2019Residentes GinecologíaNo ratings yet
- PREECLAMPSIADocument6 pagesPREECLAMPSIAMichelle ArenasNo ratings yet
- Prevalence of Preeclampsia and The Associated Risk Factors Among Pregnant Women in BangladeshDocument10 pagesPrevalence of Preeclampsia and The Associated Risk Factors Among Pregnant Women in BangladeshNanda Puspita SariNo ratings yet
- DM 22Document13 pagesDM 22hospital civilNo ratings yet
- Jurnal 4Document5 pagesJurnal 4Amalia Dwi AryantiNo ratings yet
- Eclampsia A Review On Risk Factors, Management and OutcomeDocument3 pagesEclampsia A Review On Risk Factors, Management and OutcomeKIU PUBLICATION AND EXTENSIONNo ratings yet
- Diabetes in PregnancyDocument15 pagesDiabetes in PregnancyRazi MaulanaNo ratings yet
- Gestational Diabetes Risk Factors and Long-Term Consequences For Both Mother and Offspring: A Literature ReviewDocument27 pagesGestational Diabetes Risk Factors and Long-Term Consequences For Both Mother and Offspring: A Literature ReviewBala ChandiranNo ratings yet
- Acta Obstet Gynecol Scand - 2011 - STJERNHOLM - Changed Indications For Cesarean SectionsDocument5 pagesActa Obstet Gynecol Scand - 2011 - STJERNHOLM - Changed Indications For Cesarean SectionsAli QuwarahNo ratings yet
- FIGO (International Federation Obstetrics and Gynecology) Pre-Eclampsia 2019Document58 pagesFIGO (International Federation Obstetrics and Gynecology) Pre-Eclampsia 2019Haykal Estu BhismoroNo ratings yet
- Impact of Polycystic Ovary, Metabolic Syndrome and Obesity on Women Health: Volume 8: Frontiers in Gynecological EndocrinologyFrom EverandImpact of Polycystic Ovary, Metabolic Syndrome and Obesity on Women Health: Volume 8: Frontiers in Gynecological EndocrinologyNo ratings yet
- Obstetric and Gynecologic Nephrology: Women’s Health Issues in the Patient With Kidney DiseaseFrom EverandObstetric and Gynecologic Nephrology: Women’s Health Issues in the Patient With Kidney DiseaseMala SachdevaNo ratings yet
- Virus Replication: John Goulding, Imperial College London, UKDocument1 pageVirus Replication: John Goulding, Imperial College London, UKnawal asmadiNo ratings yet
- European Journal of Obstetrics & Gynecology and Reproductive BiologyDocument6 pagesEuropean Journal of Obstetrics & Gynecology and Reproductive Biologynawal asmadiNo ratings yet
- Primary Evaluation and Acute Management of Vertigo.17Document5 pagesPrimary Evaluation and Acute Management of Vertigo.17nawal asmadiNo ratings yet
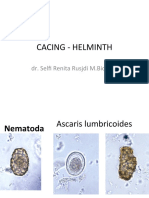
- Helminth - PictureDocument17 pagesHelminth - Picturenawal asmadiNo ratings yet
- Acute Appendicitis: by Avit SuchitraDocument33 pagesAcute Appendicitis: by Avit Suchitranawal asmadiNo ratings yet
- Praktikum Patologi Anatomi: Blok 2.1 Minggu 1 Jejas Sel & InflamasiDocument25 pagesPraktikum Patologi Anatomi: Blok 2.1 Minggu 1 Jejas Sel & Inflamasinawal asmadiNo ratings yet
- Abnormalities in The Digestive SystemDocument2 pagesAbnormalities in The Digestive Systemnawal asmadiNo ratings yet
- 2.4.4.3D Reye's Syndrome - Dr. SaptinoDocument48 pages2.4.4.3D Reye's Syndrome - Dr. Saptinonawal asmadiNo ratings yet
- Healthy LifestyleDocument3 pagesHealthy Lifestylenawal asmadiNo ratings yet
- Oral Tumor / Cancer: Wirsma Arif Harahap Head Neck and Breast Oncology Consultant Andalas Medical School PadangDocument55 pagesOral Tumor / Cancer: Wirsma Arif Harahap Head Neck and Breast Oncology Consultant Andalas Medical School Padangnawal asmadiNo ratings yet
- Tumor Saluran Cerna AtasDocument85 pagesTumor Saluran Cerna Atasnawal asmadiNo ratings yet
- Calculation of Metabolic RateDocument6 pagesCalculation of Metabolic Ratenawal asmadiNo ratings yet
- Diabtes Melitus Pada Anak (DM Tipe 1)Document51 pagesDiabtes Melitus Pada Anak (DM Tipe 1)nawal asmadiNo ratings yet
- Periop PhinmaaugustDocument221 pagesPeriop PhinmaaugustEna RodasNo ratings yet
- 8 Kao EpilepsyManagementDocument50 pages8 Kao EpilepsyManagementYipno Wanhar El MawardiNo ratings yet
- ELECTROLYTESDocument8 pagesELECTROLYTESvarshith gandlaNo ratings yet
- 05) CVA With Left Hemiparesis With Hypertension With HyperlipidemiaDocument23 pages05) CVA With Left Hemiparesis With Hypertension With HyperlipidemiaMohammed ShoaibNo ratings yet
- Oral Pathology Key PointsDocument4 pagesOral Pathology Key PointsRohit Bansal100% (1)
- Rubella IgG OrgeniumDocument6 pagesRubella IgG OrgeniumS MNo ratings yet
- Hope 1Document3 pagesHope 1Hasmine Lara RiveroNo ratings yet
- Resume - Hamid Kermani MoakharDocument2 pagesResume - Hamid Kermani Moakharmohammadrezahajian12191No ratings yet
- Case PresentationDocument19 pagesCase PresentationIbad Ur RehmanNo ratings yet
- HISTORY TAKING AND PE OF CARDIAC PATIENTS. Original.Document69 pagesHISTORY TAKING AND PE OF CARDIAC PATIENTS. Original.api-3858544No ratings yet
- Unit 7 Trauma and Triage: Kelompok 5: Agus Widayanti Mika Apriyanti Yudi Yuda SaputraDocument17 pagesUnit 7 Trauma and Triage: Kelompok 5: Agus Widayanti Mika Apriyanti Yudi Yuda SaputraZulkarnainNo ratings yet
- Long Quiz Geron LecDocument3 pagesLong Quiz Geron LecDarwin QuirimitNo ratings yet
- Buku Daftar Kode, Simbol, Tanda Dan Singkatan RSUD Dr. Soetomo Surabaya - 2018Document1 pageBuku Daftar Kode, Simbol, Tanda Dan Singkatan RSUD Dr. Soetomo Surabaya - 2018Agus HartonoNo ratings yet
- TESLA Stym - EN (English)Document6 pagesTESLA Stym - EN (English)Tatjana KecmanNo ratings yet
- UntitledDocument8 pagesUntitledAman KhanNo ratings yet
- Probiotics, Prebiotics and Synbiotics - A ReviewDocument12 pagesProbiotics, Prebiotics and Synbiotics - A ReviewluthfikhairulNo ratings yet
- Necrotizing FasciitisDocument7 pagesNecrotizing FasciitisjoycefrancielleNo ratings yet
- A Family Nursing Care Plan OnDocument4 pagesA Family Nursing Care Plan OnAnge MinguitoNo ratings yet
- IPCR July Dec 2020 FINAL Na KaauDocument7 pagesIPCR July Dec 2020 FINAL Na KaauCristina MelloriaNo ratings yet
- Journal Reading - Allergic Rhinitis - Safira AmaliaDocument34 pagesJournal Reading - Allergic Rhinitis - Safira AmaliasafiraNo ratings yet
- Delayed Ejaculation & Anorgasmia: Emmanuele A. JanniniDocument52 pagesDelayed Ejaculation & Anorgasmia: Emmanuele A. JanniniMahmoud Zedan100% (1)
- HSD Sept22 Clin Chem Saqs Essay and Case Studies Exam PapersDocument10 pagesHSD Sept22 Clin Chem Saqs Essay and Case Studies Exam PapersYusuph MipawaNo ratings yet
- Role of Dental AssistantsDocument11 pagesRole of Dental AssistantsJasmine Rey Quinto100% (1)
- Case Study - Manifestations of Obsessive-Compulsive Disorder in Young ChildrenDocument12 pagesCase Study - Manifestations of Obsessive-Compulsive Disorder in Young Childrenapi-251092359No ratings yet
- Staph Aureus in CatDocument18 pagesStaph Aureus in CatM.Aleem khanNo ratings yet
- Acfroga7p2r6i0cws Szu9k Breyv2tzvrof9ppbo2drurhrvlklv RK Pxoneirjj2xy3whbr7zxjorsqy0yzbmphv1g5d2ttklcngz6k0vdyy6yvgpgqd9jnffjcn0 Dnbjldqgiursd8k0zwaDocument65 pagesAcfroga7p2r6i0cws Szu9k Breyv2tzvrof9ppbo2drurhrvlklv RK Pxoneirjj2xy3whbr7zxjorsqy0yzbmphv1g5d2ttklcngz6k0vdyy6yvgpgqd9jnffjcn0 Dnbjldqgiursd8k0zwagames networkNo ratings yet