Download as pdf or txt
You might also like
- Blood Donation PersuasiveDocument4 pagesBlood Donation PersuasiveGigi2000100% (2)
- Kelompok C PBL 2014Document30 pagesKelompok C PBL 2014Ulfi PutriadiNo ratings yet
- The Relationship Between Multimorbidity and Quality of Life On Acute Myocardial Infaction Patients Undergoing Percutaneous Coronary Intervention in Haji Adam Malik Hospital MedanDocument11 pagesThe Relationship Between Multimorbidity and Quality of Life On Acute Myocardial Infaction Patients Undergoing Percutaneous Coronary Intervention in Haji Adam Malik Hospital MedanInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Sumber 18 CABG LansiaDocument8 pagesSumber 18 CABG Lansiamarwan febrianNo ratings yet
- Hemodialysis Internal Jugular Vein Versus Subclavian Vein Catheters: Complications, Patients' Comfort, Tolerance and Cost-EffectivenessDocument5 pagesHemodialysis Internal Jugular Vein Versus Subclavian Vein Catheters: Complications, Patients' Comfort, Tolerance and Cost-EffectivenessYolanda IrawatiNo ratings yet
- Giovannetti (2019) - Cognition and Cerebral Infarction in Older Adults After Surgical Aortic Valve ReplacementDocument8 pagesGiovannetti (2019) - Cognition and Cerebral Infarction in Older Adults After Surgical Aortic Valve ReplacementVanessaNo ratings yet
- Keywords:-STS Score, MACE, CABGDocument6 pagesKeywords:-STS Score, MACE, CABGInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Ing 5Document11 pagesIng 5Farida MufidatiNo ratings yet
- Bhavanadhar 2018Document7 pagesBhavanadhar 2018Dr Suhail AkbarNo ratings yet
- Prediktor Kegagalan Intervensi Koroner Perkutan Pada Oklusi Total Di Pusat Jantung Nasional, IndonesiaDocument9 pagesPrediktor Kegagalan Intervensi Koroner Perkutan Pada Oklusi Total Di Pusat Jantung Nasional, IndonesiaNining AnjarwatiNo ratings yet
- Cathet Cardio Intervent - 2021 - Sattar - Outcomes of Intravascular Ultrasound Versus Optical Coherence Tomography GuidedDocument11 pagesCathet Cardio Intervent - 2021 - Sattar - Outcomes of Intravascular Ultrasound Versus Optical Coherence Tomography GuidedاسحاقNo ratings yet
- Effect of Frailty On Outcomes of EndovascularDocument8 pagesEffect of Frailty On Outcomes of EndovasculartuanNo ratings yet
- Malhotra 2Document2 pagesMalhotra 2José María Carrasco RuedaNo ratings yet
- 1 s2.0 S0914508719303648 MainDocument6 pages1 s2.0 S0914508719303648 MainMarina UlfaNo ratings yet
- JofIMAB 2019 25 2p2471 2475Document5 pagesJofIMAB 2019 25 2p2471 2475afriskha bulawanNo ratings yet
- TyG VascularagingDocument8 pagesTyG VascularagingSNo ratings yet
- AnotherDocument11 pagesAnotherTudor DumitrascuNo ratings yet
- 1 s2.0 S101673151630121X MainDocument8 pages1 s2.0 S101673151630121X Mainmisbah007No ratings yet
- Sri Jayadeva - IPEJDocument6 pagesSri Jayadeva - IPEJNeha Agarwal RastogiNo ratings yet
- DANAMIDocument8 pagesDANAMIMary CogolloNo ratings yet
- JCDD 08 00100 v2Document16 pagesJCDD 08 00100 v2Paulina ArteagaNo ratings yet
- Zhao 2020Document8 pagesZhao 2020Moom TakohNo ratings yet
- Dzudie 2020Document7 pagesDzudie 2020Andi Tiara S. AdamNo ratings yet
- J Jacc 2020 09 603Document12 pagesJ Jacc 2020 09 603Alejandro Alberto Garcia de la RochaNo ratings yet
- ICD For Primary Prophylaxis of Sudden Cardiac Death: An Indian PerspectiveDocument7 pagesICD For Primary Prophylaxis of Sudden Cardiac Death: An Indian Perspectivesameerray12No ratings yet
- The Importance of Mean Platelet Volume To Lymphocyte Ratio in Predicting Atrial Fibrillation After Coronary Bypass OperationsDocument5 pagesThe Importance of Mean Platelet Volume To Lymphocyte Ratio in Predicting Atrial Fibrillation After Coronary Bypass OperationsM Ali AdrianNo ratings yet
- IJRR0012Document4 pagesIJRR0012Maximiliano xDNo ratings yet
- Cardiology Update 2017 The Third QuarterDocument4 pagesCardiology Update 2017 The Third QuarterAditya SutarNo ratings yet
- PCI or CABG, That Is The Question!: Jong Shin Woo, MD, and Weon Kim, MDDocument2 pagesPCI or CABG, That Is The Question!: Jong Shin Woo, MD, and Weon Kim, MDHeńřÿ ŁøĵæńNo ratings yet
- Cardiology Update 2017 PDFDocument4 pagesCardiology Update 2017 PDFFC Mekar AbadiNo ratings yet
- Early Discharge (Within 24 - 72 H) in Low-Risk AMI Patients Treated With PCI: Feasibility and Safety - Hajj StudyDocument7 pagesEarly Discharge (Within 24 - 72 H) in Low-Risk AMI Patients Treated With PCI: Feasibility and Safety - Hajj StudysarahNo ratings yet
- Journal Pre-Proof: Computer Methods and Programs in BiomedicineDocument23 pagesJournal Pre-Proof: Computer Methods and Programs in Biomedicinepuneet5246No ratings yet
- Nej Mo A 2300468Document10 pagesNej Mo A 2300468Eduarda GotoNo ratings yet
- 7 Stroke 2022Document5 pages7 Stroke 2022Vanesa Rubí CamposNo ratings yet
- Detection and Localization of Coronary Arterial Lesion With The Aid of Impedance Cardiography and Artificial Neural NetworkDocument8 pagesDetection and Localization of Coronary Arterial Lesion With The Aid of Impedance Cardiography and Artificial Neural Networksudipta201988No ratings yet
- International Journal of Cardiology: A B C K D A A e F G H I J ADocument9 pagesInternational Journal of Cardiology: A B C K D A A e F G H I J ASari ChaerunisahNo ratings yet
- J Interven Cardiol. 2017 1-7.: Presented By: Dr. Yusrina BR Saragih Supervisor: DR - Dr. Zulfikri Mukhtar, Sp. JP (K)Document24 pagesJ Interven Cardiol. 2017 1-7.: Presented By: Dr. Yusrina BR Saragih Supervisor: DR - Dr. Zulfikri Mukhtar, Sp. JP (K)Yusrina Njoes SaragihNo ratings yet
- Radial Artery Harvesting in Coronary Artery Bypass Grafting Surgery-Endoscopic or Open Method? A Meta-AnalysisDocument20 pagesRadial Artery Harvesting in Coronary Artery Bypass Grafting Surgery-Endoscopic or Open Method? A Meta-Analysisosve91No ratings yet
- 1 s2.0 S0735109719300956 MainDocument9 pages1 s2.0 S0735109719300956 MainAlberto PolimeniNo ratings yet
- Ivz035Document8 pagesIvz035BEATRIZ CUBILLONo ratings yet
- Jcen 22 2 78Document7 pagesJcen 22 2 78Aik NoeraNo ratings yet
- Randomized Trial of Stents Versus Bypass Surgery For Left Main Coronary Artery DiseaseDocument9 pagesRandomized Trial of Stents Versus Bypass Surgery For Left Main Coronary Artery DiseaseTommy WidjayaNo ratings yet
- Benefits and Risks of Prolonged Duration Dual - JurnalDocument11 pagesBenefits and Risks of Prolonged Duration Dual - JurnalVernika AngelinaNo ratings yet
- Setb 57 1 61 67 PDFDocument7 pagesSetb 57 1 61 67 PDFI Al WNo ratings yet
- Ischemic 19Document8 pagesIschemic 19Adina Alexandra CNo ratings yet
- ANGIOLOGIADocument13 pagesANGIOLOGIAAnnette ChavezNo ratings yet
- Treatments in Ischemic StrokeDocument18 pagesTreatments in Ischemic StrokeFercho MedNo ratings yet
- MidcabDocument7 pagesMidcabNs PadiludinNo ratings yet
- CardiologyDocument7 pagesCardiologyEmanuela SîrbuNo ratings yet
- SDH MMA EmbolDocument8 pagesSDH MMA EmbollokeshvdNo ratings yet
- Best Endovascular Versus Best Surgical Therapy in Patients With CLTI - American College of CardiologyDocument5 pagesBest Endovascular Versus Best Surgical Therapy in Patients With CLTI - American College of CardiologyvsurgeonkamranNo ratings yet
- AggarwalDocument7 pagesAggarwalSuryaNo ratings yet
- s12872 019 1096 1Document9 pagess12872 019 1096 1sarahNo ratings yet
- Joacp 38 208 PDFDocument7 pagesJoacp 38 208 PDFTan AwiNo ratings yet
- Intracerebral Hemorrhage An Update On Diagnosis and TreatmentDocument17 pagesIntracerebral Hemorrhage An Update On Diagnosis and TreatmentizzaayudiaNo ratings yet
- 4 - 01-03-07 - J Neurosurg 2007 - Decompressive Hemicraniectomy in Malignant MCA InfarctionDocument7 pages4 - 01-03-07 - J Neurosurg 2007 - Decompressive Hemicraniectomy in Malignant MCA InfarctionThiago Scharth MontenegroNo ratings yet
- Safety of Middle Meningeal Artery Embolization For Treatment of Subdural Hematoma - A Nationwide Propensity Score Matched AnalysisDocument10 pagesSafety of Middle Meningeal Artery Embolization For Treatment of Subdural Hematoma - A Nationwide Propensity Score Matched AnalysisJUANNo ratings yet
- Artigo EcmoDocument19 pagesArtigo EcmoGustavo TeixeiraNo ratings yet
- Article - Surgical Management of Infective Endocarditis - Early Predictors of Short-Term Morbidity and MortalityDocument6 pagesArticle - Surgical Management of Infective Endocarditis - Early Predictors of Short-Term Morbidity and Mortalityfluid_man_brazilNo ratings yet
- Acute Stroke Intervention: The Heart of The Matter: SciencedirectDocument2 pagesAcute Stroke Intervention: The Heart of The Matter: SciencedirectMarianaPlataNo ratings yet
- 10 36516-Jocass 1276127-3055931Document5 pages10 36516-Jocass 1276127-3055931yyyyx842No ratings yet
- Computed-Tomography a Powerful Tool for Diagnosis of Pediatric and Adult Congenital Heart Disease: Methodology and Interpretation GuideFrom EverandComputed-Tomography a Powerful Tool for Diagnosis of Pediatric and Adult Congenital Heart Disease: Methodology and Interpretation GuideNo ratings yet
- Aziz Thesis 2019Document125 pagesAziz Thesis 2019Aditya SutarNo ratings yet
- JPractCardiovascSci2161-1500016 041000Document3 pagesJPractCardiovascSci2161-1500016 041000Aditya SutarNo ratings yet
- Efficient Technology of Basalt Fiber-Reinforced CoDocument6 pagesEfficient Technology of Basalt Fiber-Reinforced CoAditya SutarNo ratings yet
- Mygov 9999999991589398782Document2 pagesMygov 9999999991589398782Aditya SutarNo ratings yet
- Predicting Concrete Corrosion of SewersDocument32 pagesPredicting Concrete Corrosion of SewersAditya SutarNo ratings yet
- Heart Failure Guidelines For India Update 2017Document6 pagesHeart Failure Guidelines For India Update 2017Aditya SutarNo ratings yet
- Anesthesia Management of Radiofrequency Ablation IDocument3 pagesAnesthesia Management of Radiofrequency Ablation IAditya SutarNo ratings yet
- CSI Cardiac Prevent 2015Document2 pagesCSI Cardiac Prevent 2015Aditya SutarNo ratings yet
- GT Unit 2Document14 pagesGT Unit 2Aditya SutarNo ratings yet
- IHS Report NikhilDocument10 pagesIHS Report NikhilAditya SutarNo ratings yet
- Hydralic MachinesDocument18 pagesHydralic MachinesAditya SutarNo ratings yet
- Clinical PathwaysDocument16 pagesClinical Pathwaysmonir61100% (1)
- Aci Parenteral Nutrition PBDocument72 pagesAci Parenteral Nutrition PBNilesh Chaudhari100% (1)
- Improving Outpatient Clinic Operations: An Exploratory Case StudyDocument6 pagesImproving Outpatient Clinic Operations: An Exploratory Case Studynurul fatma diyanaNo ratings yet
- MediCard List of Accredited Providers Aug 2022Document156 pagesMediCard List of Accredited Providers Aug 2022Ellie HarmonieNo ratings yet
- Declaration of Past Employment JIMENODocument1 pageDeclaration of Past Employment JIMENOjimeno.hazielNo ratings yet
- Maxillofacial Defects and Their Classification: A Review.: ArticleDocument7 pagesMaxillofacial Defects and Their Classification: A Review.: ArticleVivek ShankarNo ratings yet
- Interpretation: LPL - Lpl-Rohini (National Reference Lab) Sector - 18, Block - E Rohini DELHI 110085Document4 pagesInterpretation: LPL - Lpl-Rohini (National Reference Lab) Sector - 18, Block - E Rohini DELHI 110085Paras JainNo ratings yet
- Asm Course Speaker NotesDocument15 pagesAsm Course Speaker NotesJesse RobertNo ratings yet
- ESMO 2022 EGFR Mutant Non-Small-Cell Lung Cancer 20Document1 pageESMO 2022 EGFR Mutant Non-Small-Cell Lung Cancer 20EDWIN WIJAYANo ratings yet
- EmbolizacionDocument8 pagesEmbolizacionnatalia.gallinoNo ratings yet
- Warts 1Document25 pagesWarts 1Dr Narendra KumarNo ratings yet
- Mini Seminar Kelompok Jiwa MalaysiaDocument19 pagesMini Seminar Kelompok Jiwa MalaysiaMIRDAT HITIYAUTNo ratings yet
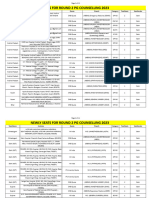
- Newly Seats For Round 2 PG Counselling 2023Document11 pagesNewly Seats For Round 2 PG Counselling 2023Manoj KumarNo ratings yet
- NF6 Unit3Document46 pagesNF6 Unit3กิ่งกาญจน์ มูลโมกข์No ratings yet
- Chronic Constipation: Harvard Medical SchoolDocument7 pagesChronic Constipation: Harvard Medical SchoolrhymenNo ratings yet
- Intrapartum AssesmentDocument71 pagesIntrapartum AssesmentHusain ChherawalaNo ratings yet
- Cerebral Palsy: Nature Reviews Disease Primers January 2016Document25 pagesCerebral Palsy: Nature Reviews Disease Primers January 2016Eduardo RodriguezNo ratings yet
- Beta Glucan For Children American Journal of Immunology 2013Document5 pagesBeta Glucan For Children American Journal of Immunology 2013MariaMaria2014No ratings yet
- Govt. College of Nursing Somajiguda Hyderabad Toddler Assessment ToolDocument18 pagesGovt. College of Nursing Somajiguda Hyderabad Toddler Assessment ToolAnnapurna DangetiNo ratings yet
- List of Dermatology Differential Diagnosis and Signs in DermatologyDocument54 pagesList of Dermatology Differential Diagnosis and Signs in DermatologyAhmadq76No ratings yet
- Anesthesiologists Compliance With Institutional Hand Hygiene PoliciesDocument8 pagesAnesthesiologists Compliance With Institutional Hand Hygiene PoliciesChristi MilanNo ratings yet
- (Ebook PDF) Julien'S Primer of Drug Action: A Comprehensive Guide To The Actions, Uses, and Side Effects of Psychoactive Drugs 14Th EditioDocument42 pages(Ebook PDF) Julien'S Primer of Drug Action: A Comprehensive Guide To The Actions, Uses, and Side Effects of Psychoactive Drugs 14Th Editiocandace.binegar878100% (42)
- Health 10 MODULEDocument26 pagesHealth 10 MODULEarmand bayoranNo ratings yet
- Web Non Subsidized Imported and Locally Manufactured Under LicenseDocument80 pagesWeb Non Subsidized Imported and Locally Manufactured Under LicenseA GhNo ratings yet
- Space Occupying Lesions SOL of The Brain - ClinicaDocument9 pagesSpace Occupying Lesions SOL of The Brain - ClinicaRandi Alan TriadiNo ratings yet
- Kirk Polka Student Generated Personal Project RubricDocument1 pageKirk Polka Student Generated Personal Project RubricKirk PolkaNo ratings yet
- C3iMagazine Pandemic Ebook RBMStudio2020Document6 pagesC3iMagazine Pandemic Ebook RBMStudio2020Wilson CrunchNo ratings yet
- 9 - Andrew O' Connor PDFDocument3 pages9 - Andrew O' Connor PDFJesa FormaranNo ratings yet