
Adductor Canal Block On Pain Vs Epidural en Artroplastia de Cadera
Adductor Canal Block On Pain Vs Epidural en Artroplastia de Cadera
You might also like
- Orthopaedic Manual Physical Therapy - From Art To Evidence (PDFDrive) PDFDocument937 pagesOrthopaedic Manual Physical Therapy - From Art To Evidence (PDFDrive) PDFBestman Ojigini81% (16)
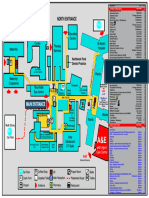
- Northwick Park Hospital Site MapDocument1 pageNorthwick Park Hospital Site MapHasaan KhanNo ratings yet
- Hospital List - HYderabadDocument45 pagesHospital List - HYderabadMuralidhar KannanNo ratings yet
- Suturas Atramat CatalogDocument173 pagesSuturas Atramat CatalogAlex Marquez de la VegaNo ratings yet
- The Erector Spinae Plane Block For Effective.9Document4 pagesThe Erector Spinae Plane Block For Effective.9Rully ZenNo ratings yet
- KJP 34 4 487Document14 pagesKJP 34 4 487Abante_gammaNo ratings yet
- Analgesia en PTRDocument7 pagesAnalgesia en PTRGuillermo Ferrer BalartNo ratings yet
- 2020 Article 74986Document8 pages2020 Article 74986Ivan DalitanNo ratings yet
- MedicineDocument10 pagesMedicineAngela OrozcoNo ratings yet
- Epi, Pcamfn, Femoral2015 InglesDocument7 pagesEpi, Pcamfn, Femoral2015 InglesAna Pamela Gallegos GuillenNo ratings yet
- Kikuchi M - QL3B For Postoperative RecoveryDocument7 pagesKikuchi M - QL3B For Postoperative Recoverywarmest.heavenNo ratings yet
- Article ComparisonOfIPACKAndPeriarticuDocument11 pagesArticle ComparisonOfIPACKAndPeriarticuRafly SuwandhiNo ratings yet
- Huang2021 Nyeri Post Opp TKRDocument6 pagesHuang2021 Nyeri Post Opp TKRRahmania Kannesia DahuriNo ratings yet
- The Effectiveness and Safety of General and Spinal Anesthesia On Systemic Inflammatory Response in Patients With Tumor-Type Total Knee ArthroplastyDocument6 pagesThe Effectiveness and Safety of General and Spinal Anesthesia On Systemic Inflammatory Response in Patients With Tumor-Type Total Knee Arthroplastyjean carlo ulloa velaNo ratings yet
- Miyazaki 2013Document6 pagesMiyazaki 2013Teja LaksanaNo ratings yet
- Comparison of The Effect of Intra-Articular, Periarticular, and Combined Injection of Analgesic On Pain Following Total Knee ArthroplastyDocument8 pagesComparison of The Effect of Intra-Articular, Periarticular, and Combined Injection of Analgesic On Pain Following Total Knee ArthroplastyFredivb1993hotmail.comNo ratings yet
- Analgesic Efficacy of Ultrasound-Guided Transversus Abdominis Plane Block in Patients Undergoing Laparoscopic AppendicectomyDocument9 pagesAnalgesic Efficacy of Ultrasound-Guided Transversus Abdominis Plane Block in Patients Undergoing Laparoscopic AppendicectomyIJAR JOURNALNo ratings yet
- 1 UsDocument7 pages1 UsJenny VibsNo ratings yet
- Transcaruncular Double Injection Technique For Peribulbar Anesthesia in Vitreoretinal SurgeryDocument5 pagesTranscaruncular Double Injection Technique For Peribulbar Anesthesia in Vitreoretinal SurgeryanxNo ratings yet
- International Journal of Anesthetics and Anesthesiology Ijaa 7 118Document7 pagesInternational Journal of Anesthetics and Anesthesiology Ijaa 7 118Ferdy RahadiyanNo ratings yet
- 1 s2.0 S2405857219300075 MainDocument8 pages1 s2.0 S2405857219300075 MainAhmed NooriNo ratings yet
- Looking For A Better Outcome After Total Knee Arthroplasty: Editorial IiDocument2 pagesLooking For A Better Outcome After Total Knee Arthroplasty: Editorial IiSatrio Bangun NegoroNo ratings yet
- A Change in Practice From Epidural To Intrathecal Morphine For Hepato Bilio SurgDocument7 pagesA Change in Practice From Epidural To Intrathecal Morphine For Hepato Bilio Surgvalerio.messinaNo ratings yet
- Research ArticleDocument10 pagesResearch ArticlethiaNo ratings yet
- Anasthesia 1Document7 pagesAnasthesia 1Rionald SitompulNo ratings yet
- Effect Observation of Electro Acupunctute AnesthesiaDocument7 pagesEffect Observation of Electro Acupunctute Anesthesiaadink mochammadNo ratings yet
- Auriculas AcupresurDocument6 pagesAuriculas AcupresurRahmania Kannesia DahuriNo ratings yet
- JURNAL2Document15 pagesJURNAL2RialNo ratings yet
- Journal of Orthopaedic Science: Original ArticleDocument9 pagesJournal of Orthopaedic Science: Original ArticleAdal ValenzuelaNo ratings yet
- Journal Reading 1Document6 pagesJournal Reading 1Mutivanya Inez MaharaniNo ratings yet
- JurnalDocument14 pagesJurnalYudha WahyuNo ratings yet
- Analgesic Effects and Adverse Reactions of LidocaiDocument6 pagesAnalgesic Effects and Adverse Reactions of Lidocaibrendastevany23No ratings yet
- Initial Experience Using Incisional Anesthetic Catheter in Abdominal Wall Ambulatory SurgeryDocument6 pagesInitial Experience Using Incisional Anesthetic Catheter in Abdominal Wall Ambulatory SurgeryilhamNo ratings yet
- Analysis Epidural Analgesia Intra Operative Cocktail Pain Management Knee Replacement TKRDocument7 pagesAnalysis Epidural Analgesia Intra Operative Cocktail Pain Management Knee Replacement TKRSSR-IIJLS JournalNo ratings yet
- Analysis Epidural Analgesia Intra Operative Cocktail Pain Management Knee Replacement TKRDocument7 pagesAnalysis Epidural Analgesia Intra Operative Cocktail Pain Management Knee Replacement TKRSSR-IIJLS JournalNo ratings yet
- 1 s2.0 S0883540320304605 MainDocument4 pages1 s2.0 S0883540320304605 MainSavNo ratings yet
- 1 s2.0 S0883540318311537 MainDocument6 pages1 s2.0 S0883540318311537 MainSavNo ratings yet
- Lee Et Al 2022 A Randomized Controlled Trial of Three Different Local Anesthetic Methods For Minor Hand SurgeryDocument9 pagesLee Et Al 2022 A Randomized Controlled Trial of Three Different Local Anesthetic Methods For Minor Hand SurgeryOscar Cayetano Herrera RodríguezNo ratings yet
- Evidence-Based Practice: Caring For A Patient Undergoing Total Knee ArthroplastyDocument5 pagesEvidence-Based Practice: Caring For A Patient Undergoing Total Knee ArthroplastyWawan HediyantoNo ratings yet
- Comparing Erector Spinae Plane Block With Serratus Anterio - 2020 - British JourDocument9 pagesComparing Erector Spinae Plane Block With Serratus Anterio - 2020 - British JourtasyadelizaNo ratings yet
- Post-Operative Clinical Outcomes in Patients With or Without The Use of Tourniquet in Total Knee Replacement SurgeryDocument3 pagesPost-Operative Clinical Outcomes in Patients With or Without The Use of Tourniquet in Total Knee Replacement SurgerymunazilatulchasanahNo ratings yet
- Austin Journal of Musculoskeletal DisordersDocument4 pagesAustin Journal of Musculoskeletal DisordersAustin Publishing GroupNo ratings yet
- e507d2a9-15d1-4ffe-96d4-dccb4188b121Document12 pagese507d2a9-15d1-4ffe-96d4-dccb4188b121Julio AltamiranoNo ratings yet
- Does The Amount of Opioid Consumption Really MatteDocument3 pagesDoes The Amount of Opioid Consumption Really MatteEmira HyseniNo ratings yet
- Jurnal 3 - Husnul AridhaDocument9 pagesJurnal 3 - Husnul AridhaHusnul AridhaNo ratings yet
- Kumar S.Document4 pagesKumar S.Van DaoNo ratings yet
- Jurnal Total Knee ArthroplastyDocument9 pagesJurnal Total Knee ArthroplastykiranaNo ratings yet
- Arthroplasty Today: Original ResearchDocument8 pagesArthroplasty Today: Original ResearchAndhi Riawan Eko WiikramatunggadewaNo ratings yet
- TAP Paper PublishedDocument8 pagesTAP Paper PublishedMotaz AbusabaaNo ratings yet
- Effects of Intraoperative Epidural Anesthesia During Hepatectomy On Intraoperative and Post-Operative Patient OutcomesDocument8 pagesEffects of Intraoperative Epidural Anesthesia During Hepatectomy On Intraoperative and Post-Operative Patient OutcomesAfniNo ratings yet
- ESP Vs QL BlockDocument10 pagesESP Vs QL BlockArdhana Surya AjiNo ratings yet
- Effect of Pulsed Electromagnetic Field Therapy in PatientsDocument7 pagesEffect of Pulsed Electromagnetic Field Therapy in PatientsNicolau IucifNo ratings yet
- Original ArticleDocument8 pagesOriginal ArticleCelina Castañeda MartinezNo ratings yet
- Kim 2018Document10 pagesKim 2018alonsoNo ratings yet
- Spinal vs. General Anesthesia For Percutaneous Nephrolithotomy: A Prospective Randomized TrialDocument5 pagesSpinal vs. General Anesthesia For Percutaneous Nephrolithotomy: A Prospective Randomized TrialDella Puspita SariNo ratings yet
- Gusti Muhammad Edy Muttaqin I4A012067 Pembimbing: Dr. Andri L. Tobing, SP - AnDocument25 pagesGusti Muhammad Edy Muttaqin I4A012067 Pembimbing: Dr. Andri L. Tobing, SP - AnBellato MauNo ratings yet
- 19 - Capítulo 4.2 - 2-Zhang e Colaboradores 2022Document13 pages19 - Capítulo 4.2 - 2-Zhang e Colaboradores 2022CharleneNo ratings yet
- Paraplegia After Open Surgical Repair Versus ThoraDocument8 pagesParaplegia After Open Surgical Repair Versus ThoraOLIVERA MOLLINEDO CAMILA ZESIANo ratings yet
- Compartement SyndromeDocument6 pagesCompartement SyndromeAnna ApsariNo ratings yet
- JMSH 2022 343Document8 pagesJMSH 2022 343jamooonNo ratings yet
- Dolor Postop, Ligamentos Cruzados, AmbulatorioDocument7 pagesDolor Postop, Ligamentos Cruzados, AmbulatorioChurrunchaNo ratings yet
- Journal 5Document8 pagesJournal 5Nydia OngaliaNo ratings yet
- Journal Reading AnestesiDocument4 pagesJournal Reading AnestesiVania RNo ratings yet
- EVALUATION OF THE INFLUENCE OF TWO DIFFERENT SYSTEMS OF ANALGESIA AND THE NASOGASTRIC TUBE ON THE INCIDENCE OF POSTOPERATIVE NAUSEA AND VOMITING IN CARDIAC SURGERYFrom EverandEVALUATION OF THE INFLUENCE OF TWO DIFFERENT SYSTEMS OF ANALGESIA AND THE NASOGASTRIC TUBE ON THE INCIDENCE OF POSTOPERATIVE NAUSEA AND VOMITING IN CARDIAC SURGERYNo ratings yet
- Surgical Techniques CageDocument14 pagesSurgical Techniques CageJulian VargasNo ratings yet
- Dr. Philip Kelton Suspension by Texas Medical BoardDocument5 pagesDr. Philip Kelton Suspension by Texas Medical BoardJasonTrahanNo ratings yet
- Definition of Damage Control OrthopaedicsDocument2 pagesDefinition of Damage Control OrthopaedicsHerryanto Agustriadi100% (1)
- NCP On Feeding The Baby With Cleft Palate 2Document2 pagesNCP On Feeding The Baby With Cleft Palate 2Anna LaritaNo ratings yet
- Lect 8 - Internal Fixation - IIDocument21 pagesLect 8 - Internal Fixation - IIAnkit LakshyaNo ratings yet
- General Clerking in Orthopaedics House Officers Workshop MalaysiaDocument10 pagesGeneral Clerking in Orthopaedics House Officers Workshop MalaysiaUzair MuhdNo ratings yet
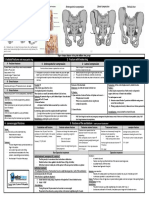
- Fracturte of Pelvis PDFDocument2 pagesFracturte of Pelvis PDFYogi drNo ratings yet
- The Radiology Specialty Is Constantly ChangingDocument3 pagesThe Radiology Specialty Is Constantly ChangingLiora SochenNo ratings yet
- Emergency Medical Care Libro CAp 1Document19 pagesEmergency Medical Care Libro CAp 1Angel ArreolaNo ratings yet
- Brochure NZOACON 2023Document4 pagesBrochure NZOACON 2023chaitanyaNo ratings yet
- Rehabilitation of A Post-Surgical Patella Fracture: Case ReportDocument4 pagesRehabilitation of A Post-Surgical Patella Fracture: Case ReportasmaNo ratings yet
- Designed, Tested and Trusted by or Professionals.: Surgical GownsDocument8 pagesDesigned, Tested and Trusted by or Professionals.: Surgical GownsMatthew CuaNo ratings yet
- Special Test Shoulder JointDocument3 pagesSpecial Test Shoulder JointTasya Azzahra FitrianiNo ratings yet
- Invite Aiims4Document1 pageInvite Aiims4srisaravananNo ratings yet
- Cmdcas Scecim Accep Cert13485 Gd207-EngDocument23 pagesCmdcas Scecim Accep Cert13485 Gd207-Engsudar1477No ratings yet
- The Healthcare WorkforceDocument44 pagesThe Healthcare Workforcewelcome martinNo ratings yet
- Jurnal Ortho 12Document4 pagesJurnal Ortho 12Santika IndahsariNo ratings yet
- POC - Review NotesDocument9 pagesPOC - Review NotesSTEFFI GABRIELLE GOLEZNo ratings yet
- Medical Device Turnkey Project Consultant Presented by Operon Startegist, PuneDocument10 pagesMedical Device Turnkey Project Consultant Presented by Operon Startegist, PuneLili SopiandiNo ratings yet
- Anatomi Sinus Paranasalis PDFDocument214 pagesAnatomi Sinus Paranasalis PDFYerni Karnita100% (1)
- Tutoplast Product Catalog (Taureon)Document12 pagesTutoplast Product Catalog (Taureon)NNMSANo ratings yet
- The Denture Frame Analysis: An Additional Diagnostic ToolDocument9 pagesThe Denture Frame Analysis: An Additional Diagnostic ToolMirek SzNo ratings yet
- Lecture 1 TF BiomechanicsDocument63 pagesLecture 1 TF BiomechanicsAlfred JacksonNo ratings yet
- Group 2 CastDocument3 pagesGroup 2 CastMary Rose AguilarNo ratings yet
- Implant Esthetics: Review ArticleDocument6 pagesImplant Esthetics: Review ArticleSahana RangarajanNo ratings yet
- An Experience With Dome Osteotomy. Final Copy (123224)Document8 pagesAn Experience With Dome Osteotomy. Final Copy (123224)Arsalan BukhariNo ratings yet























































































Download as pdf or txt
You might also like
- Orthopaedic Manual Physical Therapy - From Art To Evidence (PDFDrive) PDFDocument937 pagesOrthopaedic Manual Physical Therapy - From Art To Evidence (PDFDrive) PDFBestman Ojigini81% (16)
- Northwick Park Hospital Site MapDocument1 pageNorthwick Park Hospital Site MapHasaan KhanNo ratings yet
- Hospital List - HYderabadDocument45 pagesHospital List - HYderabadMuralidhar KannanNo ratings yet
- Suturas Atramat CatalogDocument173 pagesSuturas Atramat CatalogAlex Marquez de la VegaNo ratings yet
- The Erector Spinae Plane Block For Effective.9Document4 pagesThe Erector Spinae Plane Block For Effective.9Rully ZenNo ratings yet
- KJP 34 4 487Document14 pagesKJP 34 4 487Abante_gammaNo ratings yet
- Analgesia en PTRDocument7 pagesAnalgesia en PTRGuillermo Ferrer BalartNo ratings yet
- 2020 Article 74986Document8 pages2020 Article 74986Ivan DalitanNo ratings yet
- MedicineDocument10 pagesMedicineAngela OrozcoNo ratings yet
- Epi, Pcamfn, Femoral2015 InglesDocument7 pagesEpi, Pcamfn, Femoral2015 InglesAna Pamela Gallegos GuillenNo ratings yet
- Kikuchi M - QL3B For Postoperative RecoveryDocument7 pagesKikuchi M - QL3B For Postoperative Recoverywarmest.heavenNo ratings yet
- Article ComparisonOfIPACKAndPeriarticuDocument11 pagesArticle ComparisonOfIPACKAndPeriarticuRafly SuwandhiNo ratings yet
- Huang2021 Nyeri Post Opp TKRDocument6 pagesHuang2021 Nyeri Post Opp TKRRahmania Kannesia DahuriNo ratings yet
- The Effectiveness and Safety of General and Spinal Anesthesia On Systemic Inflammatory Response in Patients With Tumor-Type Total Knee ArthroplastyDocument6 pagesThe Effectiveness and Safety of General and Spinal Anesthesia On Systemic Inflammatory Response in Patients With Tumor-Type Total Knee Arthroplastyjean carlo ulloa velaNo ratings yet
- Miyazaki 2013Document6 pagesMiyazaki 2013Teja LaksanaNo ratings yet
- Comparison of The Effect of Intra-Articular, Periarticular, and Combined Injection of Analgesic On Pain Following Total Knee ArthroplastyDocument8 pagesComparison of The Effect of Intra-Articular, Periarticular, and Combined Injection of Analgesic On Pain Following Total Knee ArthroplastyFredivb1993hotmail.comNo ratings yet
- Analgesic Efficacy of Ultrasound-Guided Transversus Abdominis Plane Block in Patients Undergoing Laparoscopic AppendicectomyDocument9 pagesAnalgesic Efficacy of Ultrasound-Guided Transversus Abdominis Plane Block in Patients Undergoing Laparoscopic AppendicectomyIJAR JOURNALNo ratings yet
- 1 UsDocument7 pages1 UsJenny VibsNo ratings yet
- Transcaruncular Double Injection Technique For Peribulbar Anesthesia in Vitreoretinal SurgeryDocument5 pagesTranscaruncular Double Injection Technique For Peribulbar Anesthesia in Vitreoretinal SurgeryanxNo ratings yet
- International Journal of Anesthetics and Anesthesiology Ijaa 7 118Document7 pagesInternational Journal of Anesthetics and Anesthesiology Ijaa 7 118Ferdy RahadiyanNo ratings yet
- 1 s2.0 S2405857219300075 MainDocument8 pages1 s2.0 S2405857219300075 MainAhmed NooriNo ratings yet
- Looking For A Better Outcome After Total Knee Arthroplasty: Editorial IiDocument2 pagesLooking For A Better Outcome After Total Knee Arthroplasty: Editorial IiSatrio Bangun NegoroNo ratings yet
- A Change in Practice From Epidural To Intrathecal Morphine For Hepato Bilio SurgDocument7 pagesA Change in Practice From Epidural To Intrathecal Morphine For Hepato Bilio Surgvalerio.messinaNo ratings yet
- Research ArticleDocument10 pagesResearch ArticlethiaNo ratings yet
- Anasthesia 1Document7 pagesAnasthesia 1Rionald SitompulNo ratings yet
- Effect Observation of Electro Acupunctute AnesthesiaDocument7 pagesEffect Observation of Electro Acupunctute Anesthesiaadink mochammadNo ratings yet
- Auriculas AcupresurDocument6 pagesAuriculas AcupresurRahmania Kannesia DahuriNo ratings yet
- JURNAL2Document15 pagesJURNAL2RialNo ratings yet
- Journal of Orthopaedic Science: Original ArticleDocument9 pagesJournal of Orthopaedic Science: Original ArticleAdal ValenzuelaNo ratings yet
- Journal Reading 1Document6 pagesJournal Reading 1Mutivanya Inez MaharaniNo ratings yet
- JurnalDocument14 pagesJurnalYudha WahyuNo ratings yet
- Analgesic Effects and Adverse Reactions of LidocaiDocument6 pagesAnalgesic Effects and Adverse Reactions of Lidocaibrendastevany23No ratings yet
- Initial Experience Using Incisional Anesthetic Catheter in Abdominal Wall Ambulatory SurgeryDocument6 pagesInitial Experience Using Incisional Anesthetic Catheter in Abdominal Wall Ambulatory SurgeryilhamNo ratings yet
- Analysis Epidural Analgesia Intra Operative Cocktail Pain Management Knee Replacement TKRDocument7 pagesAnalysis Epidural Analgesia Intra Operative Cocktail Pain Management Knee Replacement TKRSSR-IIJLS JournalNo ratings yet
- Analysis Epidural Analgesia Intra Operative Cocktail Pain Management Knee Replacement TKRDocument7 pagesAnalysis Epidural Analgesia Intra Operative Cocktail Pain Management Knee Replacement TKRSSR-IIJLS JournalNo ratings yet
- 1 s2.0 S0883540320304605 MainDocument4 pages1 s2.0 S0883540320304605 MainSavNo ratings yet
- 1 s2.0 S0883540318311537 MainDocument6 pages1 s2.0 S0883540318311537 MainSavNo ratings yet
- Lee Et Al 2022 A Randomized Controlled Trial of Three Different Local Anesthetic Methods For Minor Hand SurgeryDocument9 pagesLee Et Al 2022 A Randomized Controlled Trial of Three Different Local Anesthetic Methods For Minor Hand SurgeryOscar Cayetano Herrera RodríguezNo ratings yet
- Evidence-Based Practice: Caring For A Patient Undergoing Total Knee ArthroplastyDocument5 pagesEvidence-Based Practice: Caring For A Patient Undergoing Total Knee ArthroplastyWawan HediyantoNo ratings yet
- Comparing Erector Spinae Plane Block With Serratus Anterio - 2020 - British JourDocument9 pagesComparing Erector Spinae Plane Block With Serratus Anterio - 2020 - British JourtasyadelizaNo ratings yet
- Post-Operative Clinical Outcomes in Patients With or Without The Use of Tourniquet in Total Knee Replacement SurgeryDocument3 pagesPost-Operative Clinical Outcomes in Patients With or Without The Use of Tourniquet in Total Knee Replacement SurgerymunazilatulchasanahNo ratings yet
- Austin Journal of Musculoskeletal DisordersDocument4 pagesAustin Journal of Musculoskeletal DisordersAustin Publishing GroupNo ratings yet
- e507d2a9-15d1-4ffe-96d4-dccb4188b121Document12 pagese507d2a9-15d1-4ffe-96d4-dccb4188b121Julio AltamiranoNo ratings yet
- Does The Amount of Opioid Consumption Really MatteDocument3 pagesDoes The Amount of Opioid Consumption Really MatteEmira HyseniNo ratings yet
- Jurnal 3 - Husnul AridhaDocument9 pagesJurnal 3 - Husnul AridhaHusnul AridhaNo ratings yet
- Kumar S.Document4 pagesKumar S.Van DaoNo ratings yet
- Jurnal Total Knee ArthroplastyDocument9 pagesJurnal Total Knee ArthroplastykiranaNo ratings yet
- Arthroplasty Today: Original ResearchDocument8 pagesArthroplasty Today: Original ResearchAndhi Riawan Eko WiikramatunggadewaNo ratings yet
- TAP Paper PublishedDocument8 pagesTAP Paper PublishedMotaz AbusabaaNo ratings yet
- Effects of Intraoperative Epidural Anesthesia During Hepatectomy On Intraoperative and Post-Operative Patient OutcomesDocument8 pagesEffects of Intraoperative Epidural Anesthesia During Hepatectomy On Intraoperative and Post-Operative Patient OutcomesAfniNo ratings yet
- ESP Vs QL BlockDocument10 pagesESP Vs QL BlockArdhana Surya AjiNo ratings yet
- Effect of Pulsed Electromagnetic Field Therapy in PatientsDocument7 pagesEffect of Pulsed Electromagnetic Field Therapy in PatientsNicolau IucifNo ratings yet
- Original ArticleDocument8 pagesOriginal ArticleCelina Castañeda MartinezNo ratings yet
- Kim 2018Document10 pagesKim 2018alonsoNo ratings yet
- Spinal vs. General Anesthesia For Percutaneous Nephrolithotomy: A Prospective Randomized TrialDocument5 pagesSpinal vs. General Anesthesia For Percutaneous Nephrolithotomy: A Prospective Randomized TrialDella Puspita SariNo ratings yet
- Gusti Muhammad Edy Muttaqin I4A012067 Pembimbing: Dr. Andri L. Tobing, SP - AnDocument25 pagesGusti Muhammad Edy Muttaqin I4A012067 Pembimbing: Dr. Andri L. Tobing, SP - AnBellato MauNo ratings yet
- 19 - Capítulo 4.2 - 2-Zhang e Colaboradores 2022Document13 pages19 - Capítulo 4.2 - 2-Zhang e Colaboradores 2022CharleneNo ratings yet
- Paraplegia After Open Surgical Repair Versus ThoraDocument8 pagesParaplegia After Open Surgical Repair Versus ThoraOLIVERA MOLLINEDO CAMILA ZESIANo ratings yet
- Compartement SyndromeDocument6 pagesCompartement SyndromeAnna ApsariNo ratings yet
- JMSH 2022 343Document8 pagesJMSH 2022 343jamooonNo ratings yet
- Dolor Postop, Ligamentos Cruzados, AmbulatorioDocument7 pagesDolor Postop, Ligamentos Cruzados, AmbulatorioChurrunchaNo ratings yet
- Journal 5Document8 pagesJournal 5Nydia OngaliaNo ratings yet
- Journal Reading AnestesiDocument4 pagesJournal Reading AnestesiVania RNo ratings yet
- EVALUATION OF THE INFLUENCE OF TWO DIFFERENT SYSTEMS OF ANALGESIA AND THE NASOGASTRIC TUBE ON THE INCIDENCE OF POSTOPERATIVE NAUSEA AND VOMITING IN CARDIAC SURGERYFrom EverandEVALUATION OF THE INFLUENCE OF TWO DIFFERENT SYSTEMS OF ANALGESIA AND THE NASOGASTRIC TUBE ON THE INCIDENCE OF POSTOPERATIVE NAUSEA AND VOMITING IN CARDIAC SURGERYNo ratings yet
- Surgical Techniques CageDocument14 pagesSurgical Techniques CageJulian VargasNo ratings yet
- Dr. Philip Kelton Suspension by Texas Medical BoardDocument5 pagesDr. Philip Kelton Suspension by Texas Medical BoardJasonTrahanNo ratings yet
- Definition of Damage Control OrthopaedicsDocument2 pagesDefinition of Damage Control OrthopaedicsHerryanto Agustriadi100% (1)
- NCP On Feeding The Baby With Cleft Palate 2Document2 pagesNCP On Feeding The Baby With Cleft Palate 2Anna LaritaNo ratings yet
- Lect 8 - Internal Fixation - IIDocument21 pagesLect 8 - Internal Fixation - IIAnkit LakshyaNo ratings yet
- General Clerking in Orthopaedics House Officers Workshop MalaysiaDocument10 pagesGeneral Clerking in Orthopaedics House Officers Workshop MalaysiaUzair MuhdNo ratings yet
- Fracturte of Pelvis PDFDocument2 pagesFracturte of Pelvis PDFYogi drNo ratings yet
- The Radiology Specialty Is Constantly ChangingDocument3 pagesThe Radiology Specialty Is Constantly ChangingLiora SochenNo ratings yet
- Emergency Medical Care Libro CAp 1Document19 pagesEmergency Medical Care Libro CAp 1Angel ArreolaNo ratings yet
- Brochure NZOACON 2023Document4 pagesBrochure NZOACON 2023chaitanyaNo ratings yet
- Rehabilitation of A Post-Surgical Patella Fracture: Case ReportDocument4 pagesRehabilitation of A Post-Surgical Patella Fracture: Case ReportasmaNo ratings yet
- Designed, Tested and Trusted by or Professionals.: Surgical GownsDocument8 pagesDesigned, Tested and Trusted by or Professionals.: Surgical GownsMatthew CuaNo ratings yet
- Special Test Shoulder JointDocument3 pagesSpecial Test Shoulder JointTasya Azzahra FitrianiNo ratings yet
- Invite Aiims4Document1 pageInvite Aiims4srisaravananNo ratings yet
- Cmdcas Scecim Accep Cert13485 Gd207-EngDocument23 pagesCmdcas Scecim Accep Cert13485 Gd207-Engsudar1477No ratings yet
- The Healthcare WorkforceDocument44 pagesThe Healthcare Workforcewelcome martinNo ratings yet
- Jurnal Ortho 12Document4 pagesJurnal Ortho 12Santika IndahsariNo ratings yet
- POC - Review NotesDocument9 pagesPOC - Review NotesSTEFFI GABRIELLE GOLEZNo ratings yet
- Medical Device Turnkey Project Consultant Presented by Operon Startegist, PuneDocument10 pagesMedical Device Turnkey Project Consultant Presented by Operon Startegist, PuneLili SopiandiNo ratings yet
- Anatomi Sinus Paranasalis PDFDocument214 pagesAnatomi Sinus Paranasalis PDFYerni Karnita100% (1)
- Tutoplast Product Catalog (Taureon)Document12 pagesTutoplast Product Catalog (Taureon)NNMSANo ratings yet
- The Denture Frame Analysis: An Additional Diagnostic ToolDocument9 pagesThe Denture Frame Analysis: An Additional Diagnostic ToolMirek SzNo ratings yet
- Lecture 1 TF BiomechanicsDocument63 pagesLecture 1 TF BiomechanicsAlfred JacksonNo ratings yet
- Group 2 CastDocument3 pagesGroup 2 CastMary Rose AguilarNo ratings yet
- Implant Esthetics: Review ArticleDocument6 pagesImplant Esthetics: Review ArticleSahana RangarajanNo ratings yet
- An Experience With Dome Osteotomy. Final Copy (123224)Document8 pagesAn Experience With Dome Osteotomy. Final Copy (123224)Arsalan BukhariNo ratings yet