Download as pdf or txt
You might also like
- Handbook Emergency Cardiovascular Care Healthcare Providers PDFDocument2 pagesHandbook Emergency Cardiovascular Care Healthcare Providers PDFnoble78650% (4)
- Chapter 13 and 16 Worksheet 46 QuestionsDocument7 pagesChapter 13 and 16 Worksheet 46 Questionsbilly100% (2)
- Bedside Ultrasound: Level 1 - Second EditionFrom EverandBedside Ultrasound: Level 1 - Second EditionRating: 5 out of 5 stars5/5 (1)
- Free NMCN Objective Questions Section B Professional ExamDocument5 pagesFree NMCN Objective Questions Section B Professional ExamMaryam Ib100% (15)
- 2020 AHA Guidelines For CPR & ECCDocument42 pages2020 AHA Guidelines For CPR & ECCArun100% (1)
- Capitol University College of Nursing RLE 6 List of Supervised Nursing ProceduresDocument9 pagesCapitol University College of Nursing RLE 6 List of Supervised Nursing Proceduresjizea05100% (3)
- ACLS Recerti Cation Exam Quiz: (/my-Account/)Document6 pagesACLS Recerti Cation Exam Quiz: (/my-Account/)andres novoaNo ratings yet
- Recent Final Frca Vascular Anaesthesia QuestionsDocument4 pagesRecent Final Frca Vascular Anaesthesia Questionslim sjNo ratings yet
- Anesthesiology Resident Manual of Procedures: A Step-by-Step GuideFrom EverandAnesthesiology Resident Manual of Procedures: A Step-by-Step GuideNo ratings yet
- Ontario - Schedule of Benefits 2021Document970 pagesOntario - Schedule of Benefits 2021Raj LoganathanNo ratings yet
- Field Apraisal Report Final 11Document10 pagesField Apraisal Report Final 11Raja100% (1)
- Thesis TopicsDocument7 pagesThesis TopicsShoyeb Khan100% (1)
- PICU Hospital Assessment Form State Life V3Document4 pagesPICU Hospital Assessment Form State Life V3Anwar Pervaiz PervaizNo ratings yet
- CCU Hospital Assessment Form State Life V2Document4 pagesCCU Hospital Assessment Form State Life V2Anwar Pervaiz PervaizNo ratings yet
- NicuDocument4 pagesNicuAnwar Pervaiz PervaizNo ratings yet
- WHO Surgical Safety Checklist: Ilocos Sur Provincial Hospital-Gabriela SilangDocument1 pageWHO Surgical Safety Checklist: Ilocos Sur Provincial Hospital-Gabriela SilangRyrey Abraham PacamanaNo ratings yet
- FPSC No: 55 Mcqs On Submission Deadline: 19 November 2013 12 NoonDocument4 pagesFPSC No: 55 Mcqs On Submission Deadline: 19 November 2013 12 Noonhassanmurtazashah33No ratings yet
- Deluxe & Above /others - Single Room A/C Sharing / Single Non A/c General Ward / Multi SharingDocument13 pagesDeluxe & Above /others - Single Room A/C Sharing / Single Non A/c General Ward / Multi SharingSanket SahareNo ratings yet
- Check List For SNCUDocument5 pagesCheck List For SNCUpriyahospitalNo ratings yet
- Clinical Service AreasDocument4 pagesClinical Service AreasR SheeNo ratings yet
- Tool For Situational Analysis To Assess Emergency and Essential Surgical CareDocument4 pagesTool For Situational Analysis To Assess Emergency and Essential Surgical CareGanashiam NadarasaNo ratings yet
- Level 4: Section A: Facility InformationDocument10 pagesLevel 4: Section A: Facility Informationpaul kioiNo ratings yet
- Cheklist Keamanan InsisiDocument1 pageCheklist Keamanan InsisiRiska AsafitriNo ratings yet
- Cotabato Regional and Medical Center Diagnostic Procedures Stat/Requested Done at Emergency RoomDocument1 pageCotabato Regional and Medical Center Diagnostic Procedures Stat/Requested Done at Emergency RoomSeychelle DucusinNo ratings yet
- Final Ob GynDocument4 pagesFinal Ob GynRaydoon SadeqNo ratings yet
- 7 Series (Radiology) : X-Ray Coding PointsDocument7 pages7 Series (Radiology) : X-Ray Coding PointsVijay UNo ratings yet
- Euroscore IiDocument5 pagesEuroscore IiYadira SantosNo ratings yet
- Final General SurgeryDocument3 pagesFinal General SurgeryRaydoon SadeqNo ratings yet
- Who Surgical Safety Checklist: Sign in Time Out Sign OutDocument1 pageWho Surgical Safety Checklist: Sign in Time Out Sign OutAllen Mark Galve MatutinaNo ratings yet
- Thoracic Surgery ManualDocument63 pagesThoracic Surgery ManualAhmed Abd El HamedNo ratings yet
- Emergency Radiology With QuizDocument115 pagesEmergency Radiology With QuizAndre PrawiradinataNo ratings yet
- Cardiology Department: Iccu and WardsDocument12 pagesCardiology Department: Iccu and WardsPooja100% (1)
- Abdomen X RayDocument4 pagesAbdomen X RaytimvrghsNo ratings yet
- TOACS Answer Key For CandidatesDocument30 pagesTOACS Answer Key For Candidatesaliakbar178No ratings yet
- Emergency Department Crowd ManagementDocument4 pagesEmergency Department Crowd ManagementPrabhat Kumar100% (1)
- Do We Still Need A Stethoscope - Stats For Top 10 Cardiac Tests - Roland SabbaghDocument45 pagesDo We Still Need A Stethoscope - Stats For Top 10 Cardiac Tests - Roland SabbaghJason WongNo ratings yet
- DA (SA) Past Papers - 2019 2nd SemesterDocument47 pagesDA (SA) Past Papers - 2019 2nd SemesterYudhika NaidooNo ratings yet
- Önemli ECLS Registry FormDocument9 pagesÖnemli ECLS Registry Formyowewe7363No ratings yet
- Clinic Establishment - REGISTRATION FORMDocument6 pagesClinic Establishment - REGISTRATION FORMPandiyanyadav arkNo ratings yet
- Spec Sheet Dharmais-FujiDocument36 pagesSpec Sheet Dharmais-FujiRendy Syauqy HasanNo ratings yet
- Train The Trainer ManualDocument57 pagesTrain The Trainer Manualtvm tbytNo ratings yet
- HIT PresentationDocument28 pagesHIT PresentationAyuni SallehNo ratings yet
- CHC ChecklistDocument63 pagesCHC Checklistvibha_bansalNo ratings yet
- Radiology Exercises 08022013Document3 pagesRadiology Exercises 08022013anishrove2No ratings yet
- Competition Scenario TemplateDocument2 pagesCompetition Scenario TemplatePCHANFANNo ratings yet
- DA (SA) Past Papers - 2018 2nd SemesterDocument46 pagesDA (SA) Past Papers - 2018 2nd SemesterYudhika NaidooNo ratings yet
- FCA (SA) - Part - II - Past - Papers 7Document29 pagesFCA (SA) - Part - II - Past - Papers 7matentenNo ratings yet
- 2011 Appendix A UpdatesDocument65 pages2011 Appendix A UpdatesfaithNo ratings yet
- Medical Terminology: Abbreviations WorksheetDocument6 pagesMedical Terminology: Abbreviations WorksheetMuliani Indah SariNo ratings yet
- Hsin10542 25 06 2014Document136 pagesHsin10542 25 06 2014Anil KumarNo ratings yet
- WHOSurgical Safety Checklist TemplateDocument2 pagesWHOSurgical Safety Checklist Templateraj1969No ratings yet
- Apical Four Chamber Echocardiogram ViewDocument6 pagesApical Four Chamber Echocardiogram ViewMaria EdelNo ratings yet
- ACLS Management in Covid-19 & AHA 2020-Yudi ElyasDocument64 pagesACLS Management in Covid-19 & AHA 2020-Yudi ElyasayatullahNo ratings yet
- AF Catheter AblationDocument37 pagesAF Catheter AblationSnehal JayaramNo ratings yet
- NCM 118 Rle Exam PrelimDocument6 pagesNCM 118 Rle Exam Prelimsncmanguiat.2202276.chasnNo ratings yet
- ABC Versus CAB For Cardiopulmonary ResuscitationDocument16 pagesABC Versus CAB For Cardiopulmonary Resuscitationaldo199No ratings yet
- Soal Ujian EBM PraktekDocument6 pagesSoal Ujian EBM Praktekbobbyrianto2210No ratings yet
- ICU Service Assessment Tool EditedDocument16 pagesICU Service Assessment Tool EditedAshu AberaNo ratings yet
- Facility Details ENTRY PDF FORM PDFDocument3 pagesFacility Details ENTRY PDF FORM PDFdydmho gajwelNo ratings yet
- Online Appendix B2 (Pleural Disease) - Pleural Effusion Image Guided or Non Image GuidedDocument7 pagesOnline Appendix B2 (Pleural Disease) - Pleural Effusion Image Guided or Non Image Guided4wntsgj69pNo ratings yet
- Standardized Methods For Measuring Diagnostic X-Ray ExposuresDocument26 pagesStandardized Methods For Measuring Diagnostic X-Ray Exposuresmohadese EstajiNo ratings yet
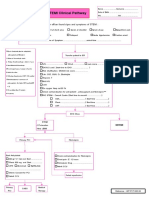
- STEMI Clinical PathwayDocument1 pageSTEMI Clinical PathwayKanoknun PisitpatcaragulNo ratings yet
- Adult Cardiopulmonary PracticeDocument41 pagesAdult Cardiopulmonary PracticeDinda RadetaNo ratings yet
- Cardiothoracic SurgeryDocument2 pagesCardiothoracic Surgeryc3145848No ratings yet
- Pediatrics: Rheumatology Will Roll Up To Pediatrics: General Pediatrics: Urology Will Roll Up To UrologyDocument47 pagesPediatrics: Rheumatology Will Roll Up To Pediatrics: General Pediatrics: Urology Will Roll Up To UrologydasbosiNo ratings yet
- Day Care AnesthesiaDocument68 pagesDay Care AnesthesiaSri Sruthi PichikaNo ratings yet
- Doctor Data For Pune Location 5Document8 pagesDoctor Data For Pune Location 5sadiq shaikhNo ratings yet
- Regional Anesthesia in CattleDocument33 pagesRegional Anesthesia in CattleBibek SutradharNo ratings yet
- World Health Organization Surgical Safety ChecklistDocument9 pagesWorld Health Organization Surgical Safety Checklistprisselya anisaNo ratings yet
- Abg Interpretation Practice TestDocument3 pagesAbg Interpretation Practice TestPatty RomeroNo ratings yet
- Best Orthopedic Specialist Surgeon Clinic & Doctor in MumbaiDocument40 pagesBest Orthopedic Specialist Surgeon Clinic & Doctor in Mumbaipranjal kodkaniNo ratings yet
- 'Single Bougie and Double Tube Technique'-A Novel Technique in Unanticipated Difficult Nasal IntubationDocument1 page'Single Bougie and Double Tube Technique'-A Novel Technique in Unanticipated Difficult Nasal IntubationRavikiran SuryanarayanamurthyNo ratings yet
- Laporan Operasi: Operation ReportDocument3 pagesLaporan Operasi: Operation ReportaininNo ratings yet
- Nursing Clinical Case Study AnalysisDocument5 pagesNursing Clinical Case Study Analysisapi-664257988No ratings yet
- C135221004 - Alfitra HalilDocument20 pagesC135221004 - Alfitra HalilIhsanul Ma'arifNo ratings yet
- Management of The Difficult Airway in The Pediatric PatientDocument11 pagesManagement of The Difficult Airway in The Pediatric PatientDaniel GallegoNo ratings yet
- ACLS Skills ChecklistDocument2 pagesACLS Skills ChecklistabdullahNo ratings yet
- Communication Report: Submitted By: Muhammad Daniyal Khan Hafiza Wajiha HamidDocument9 pagesCommunication Report: Submitted By: Muhammad Daniyal Khan Hafiza Wajiha HamidUmme SumaiyaNo ratings yet
- Fuhrman and Zimmermans Pediatric Critical Care 6Th Edition Jerry J Zimmerman Full ChapterDocument67 pagesFuhrman and Zimmermans Pediatric Critical Care 6Th Edition Jerry J Zimmerman Full Chaptertimothy.daniels842100% (9)
- Akupunktur: Trigger Points and Classical Acupuncture PointsDocument6 pagesAkupunktur: Trigger Points and Classical Acupuncture PointspedroNo ratings yet
- ONE Capnography: Small, Simple, More EffectiveDocument4 pagesONE Capnography: Small, Simple, More Effectiveleopa78No ratings yet
- FUNDA - Conceptual & Theoretical Models of NursingDocument7 pagesFUNDA - Conceptual & Theoretical Models of NursingRICVANNo ratings yet
- Racheal Ntubation: Dan F. CaseyDocument8 pagesRacheal Ntubation: Dan F. CaseychotimahNo ratings yet
- How To Pass The Edaic Andrey Varvinskiy Full ChapterDocument67 pagesHow To Pass The Edaic Andrey Varvinskiy Full Chaptercathleen.jaynes584100% (12)
- 295 QsDocument3 pages295 Qsujangketul62No ratings yet
- Test Bank For Building A Medical Vocabulary 7th Edition Leonard DownloadDocument20 pagesTest Bank For Building A Medical Vocabulary 7th Edition Leonard DownloadMarquis Dixon100% (39)
- Employees Compensation and State Insurance Fund HandoutDocument19 pagesEmployees Compensation and State Insurance Fund HandoutDanice Go GanNo ratings yet
- Adult Cardiac Arrest Circular Algorithm: Monitor CPR QualityDocument1 pageAdult Cardiac Arrest Circular Algorithm: Monitor CPR QualityChris LeeNo ratings yet
- Anesthesia For Ruptured Globe Repair - American Academy of OphthalmologyDocument2 pagesAnesthesia For Ruptured Globe Repair - American Academy of OphthalmologyAlejandro N. Fonseca GrandaNo ratings yet
- ps09 2010 Guidelines On Sedation and or Analgesia For Diagnostic and Interventional Medical Dental or Surgical ProceduresDocument16 pagesps09 2010 Guidelines On Sedation and or Analgesia For Diagnostic and Interventional Medical Dental or Surgical ProceduresJane KoNo ratings yet