Download as pdf or txt
You might also like
- Huawei ICT Competition 2019-2020 Preliminary Examination Outline - PAkDocument5 pagesHuawei ICT Competition 2019-2020 Preliminary Examination Outline - PAkHamad KhanNo ratings yet
- Ojo 2021092215172319Document10 pagesOjo 2021092215172319Saffa AzharaaniNo ratings yet
- Bone Health ECHO: Telementoring To Improve Osteoporosis CareDocument3 pagesBone Health ECHO: Telementoring To Improve Osteoporosis CareSapitriNo ratings yet
- Research Article: Epidemiology of Maxillofacial Fractures at A Teaching Hospital in Malaysia: A Retrospective StudyDocument11 pagesResearch Article: Epidemiology of Maxillofacial Fractures at A Teaching Hospital in Malaysia: A Retrospective Studydr_nadheemNo ratings yet
- Incidence of Mandibular FractureDocument7 pagesIncidence of Mandibular FractureZaher ShNo ratings yet
- Australian - 2008 - Maxillofacial Trauma in Major Trauma PatientsDocument6 pagesAustralian - 2008 - Maxillofacial Trauma in Major Trauma Patientsووويويويةءتؤوبةين للاNo ratings yet
- 2016 Article 89Document20 pages2016 Article 89soylahijadeunvampiroNo ratings yet
- 2022 Article 795Document8 pages2022 Article 795Juan David Hernández CifuentesNo ratings yet
- Non-Medial Infectious Orbital Cellulitis: Etiology, Causative Organisms, Radiologic Findings, Management and ComplicationsDocument11 pagesNon-Medial Infectious Orbital Cellulitis: Etiology, Causative Organisms, Radiologic Findings, Management and ComplicationsPutri Sari DewiNo ratings yet
- Trauma Pattern in A Level I East-European Trauma Center: July 2015Document5 pagesTrauma Pattern in A Level I East-European Trauma Center: July 2015Andreea SlabuNo ratings yet
- An Injury Profile of Maxillofacial Trauma in Yaounde An Observational Study in CameroonDocument9 pagesAn Injury Profile of Maxillofacial Trauma in Yaounde An Observational Study in CameroonAthenaeum Scientific PublishersNo ratings yet
- Quantitative Diagnosis of Rotator Cuff Tears Based On Sonographic Pattern RecognitionDocument13 pagesQuantitative Diagnosis of Rotator Cuff Tears Based On Sonographic Pattern RecognitionJuwita Valen RamadhanniaNo ratings yet
- (19330693 - Journal of Neurosurgery) Estimating The Global Incidence of Traumatic Brain InjuryDocument18 pages(19330693 - Journal of Neurosurgery) Estimating The Global Incidence of Traumatic Brain InjuryIqra AlghifarihNo ratings yet
- Biomarkers of (Osteo) Arthritis: EditorialDocument6 pagesBiomarkers of (Osteo) Arthritis: EditorialeliasNo ratings yet
- Proximal Humerus Fractures Epidemiology and TrendsDocument5 pagesProximal Humerus Fractures Epidemiology and TrendsHelena Sofia Fonseca Paiva De Sousa TelesNo ratings yet
- Epidemiologia de Lesiones de Punta de Dedo en Hospital de PEMEXDocument14 pagesEpidemiologia de Lesiones de Punta de Dedo en Hospital de PEMEXOscar Cayetano Herrera RodríguezNo ratings yet
- Diagnostics 12 01289Document15 pagesDiagnostics 12 01289Sushmica BaquiranNo ratings yet
- Journal of Orthopaedic Diseases and TraumatologyDocument5 pagesJournal of Orthopaedic Diseases and TraumatologySantosh KumarNo ratings yet
- Devendra 2020Document10 pagesDevendra 2020andiNo ratings yet
- CASE-STUDYDocument19 pagesCASE-STUDYRovic Selga TrisinioNo ratings yet
- Bali 2011Document4 pagesBali 2011ashkisaragiNo ratings yet
- Sciencedirect: Prevalence and Etiology of Midfacial Fractures: A Study of 799 CasesDocument6 pagesSciencedirect: Prevalence and Etiology of Midfacial Fractures: A Study of 799 CasesSuci NourmalizaNo ratings yet
- 12 Padmanabha EtalDocument4 pages12 Padmanabha EtaleditorijmrhsNo ratings yet
- Prevalence and Distribution of Odontogenic Cysts and Tumors in North Indian Population A Database Study With Systematic ReviewDocument14 pagesPrevalence and Distribution of Odontogenic Cysts and Tumors in North Indian Population A Database Study With Systematic ReviewVaishnega S.ANo ratings yet
- The Management of Diabetic Foot in The EmergencyDocument7 pagesThe Management of Diabetic Foot in The EmergencyIJAR JOURNALNo ratings yet
- 1 s2.0 S1078588424001151 Main - 2Document10 pages1 s2.0 S1078588424001151 Main - 2kouame2907No ratings yet
- 1 s2.0 S1040842822001093 MainDocument10 pages1 s2.0 S1040842822001093 Maindaniel Montaño gomezNo ratings yet
- Clinical and Demographic Study On Open Fractures Caused by Motorcycle Traffic AccidentsDocument5 pagesClinical and Demographic Study On Open Fractures Caused by Motorcycle Traffic Accidentsocta dikhoNo ratings yet
- Optimising Prevention of Surgical Wound Complications: Detection, Diagnosis, Surveillance and PredictionDocument28 pagesOptimising Prevention of Surgical Wound Complications: Detection, Diagnosis, Surveillance and PredictionAngel PerezNo ratings yet
- Duodeno-Pancreatic and Extrahepatic Biliary Tree Trauma - WSES-AAST Guidelines Open AccessDocument23 pagesDuodeno-Pancreatic and Extrahepatic Biliary Tree Trauma - WSES-AAST Guidelines Open AccessDiego Andres VasquezNo ratings yet
- Applsci 11 08481 v2Document23 pagesApplsci 11 08481 v2LaurentNo ratings yet
- A Prospective Descriptive Study of Trauma Registry in Netaji Subhash Chandra Bose Medical College, JabalpurDocument9 pagesA Prospective Descriptive Study of Trauma Registry in Netaji Subhash Chandra Bose Medical College, JabalpurIJAR JOURNALNo ratings yet
- Con Favre Ux 2018Document29 pagesCon Favre Ux 2018dianpayanganNo ratings yet
- Jgo 27 E1Document10 pagesJgo 27 E1Angga Witra NandaNo ratings yet
- JofIMAB2013vol19b2p282 285 PDFDocument4 pagesJofIMAB2013vol19b2p282 285 PDFAlung Padang SiraitNo ratings yet
- The Literature Review of Ollier DiseaseDocument8 pagesThe Literature Review of Ollier DiseaseCassNo ratings yet
- Nihms976360 PDFDocument17 pagesNihms976360 PDFyenny handayani sihiteNo ratings yet
- Pattern of Maxillofacial Fractures A 5-Year Analysis of 8,818 PatientsDocument5 pagesPattern of Maxillofacial Fractures A 5-Year Analysis of 8,818 Patients6hd6mnrzw2No ratings yet
- Assessment of Fracture Risk and Its Application To Screening For Postmenopausal Osteoporosis Synopsis of A WHO ReportDocument14 pagesAssessment of Fracture Risk and Its Application To Screening For Postmenopausal Osteoporosis Synopsis of A WHO ReportKhủngLongSiêuNguyHiểmNo ratings yet
- Epidemiology and Patho-Anatomical Pattern of 2,011 Humeral Fractures: Data From The Swedish Fracture RegisterDocument10 pagesEpidemiology and Patho-Anatomical Pattern of 2,011 Humeral Fractures: Data From The Swedish Fracture RegisterGabriel GolesteanuNo ratings yet
- Antibiotics 11 00568Document8 pagesAntibiotics 11 00568Vincia PaulNo ratings yet
- Artículo 3Document9 pagesArtículo 3JuanNo ratings yet
- APJCP Volume 17 Issue 9 Pages 4335-4340Document6 pagesAPJCP Volume 17 Issue 9 Pages 4335-4340putriNo ratings yet
- Katsuura 2016Document6 pagesKatsuura 2016Wahyu InsanNo ratings yet
- Jurnal Ulkus KorneaDocument10 pagesJurnal Ulkus KorneaPutri Dery CahyaniNo ratings yet
- Metsemakers2017 1Document16 pagesMetsemakers2017 1Cris JiménezNo ratings yet
- Ess20 BPS Ssi Wuk FinalDocument18 pagesEss20 BPS Ssi Wuk FinaldynararakelNo ratings yet
- JPM 11 00110Document12 pagesJPM 11 00110Johnny CshNo ratings yet
- Acute Nursing Care of The Older Adult With Fragility Hip Fracture: An International Perspective (Part 2)Document26 pagesAcute Nursing Care of The Older Adult With Fragility Hip Fracture: An International Perspective (Part 2)spring flowerNo ratings yet
- Describing Pediatric Fractures in The Era of ICD-10Document15 pagesDescribing Pediatric Fractures in The Era of ICD-10Alessio CasaleNo ratings yet
- Lancent BrainDocument62 pagesLancent BrainAdriana SerratoNo ratings yet
- Fracture HealingDocument6 pagesFracture Healingpunct_org3256No ratings yet
- Clinical Presentation, Management, and Prognosis of Pseudogout in Joint Arthroplasty: A Retrospective Cohort StudyDocument7 pagesClinical Presentation, Management, and Prognosis of Pseudogout in Joint Arthroplasty: A Retrospective Cohort StudyPutri Aswariyah RamliNo ratings yet
- International Journal of GerontologyDocument5 pagesInternational Journal of Gerontologydawn moonNo ratings yet
- The Apsic Guidelines FOR The Prevention of Surgical Site InfectionsDocument55 pagesThe Apsic Guidelines FOR The Prevention of Surgical Site InfectionsFaozan FikriNo ratings yet
- Working Version - Palau Policy BriefDocument17 pagesWorking Version - Palau Policy BriefJoseph DreyNo ratings yet
- SaudiJOralSci313-2968904 081449Document9 pagesSaudiJOralSci313-2968904 081449EnochDomprehNo ratings yet
- Articulo 4Document11 pagesArticulo 4Alan SublimeNo ratings yet
- Association of The Dominant Hand and Needle Stick Injuries For Healthcare Workers in TaiwanDocument5 pagesAssociation of The Dominant Hand and Needle Stick Injuries For Healthcare Workers in TaiwanmochkurniawanNo ratings yet
- Incidence and Risk Factors For Surgical Site Infection Following Elective Foot and Ankle Surgery: A Retrospective StudyDocument8 pagesIncidence and Risk Factors For Surgical Site Infection Following Elective Foot and Ankle Surgery: A Retrospective StudyFrancisco Castillo VázquezNo ratings yet
- Diagnostic Problems in Tumors of Head and Neck: Selected TopicsFrom EverandDiagnostic Problems in Tumors of Head and Neck: Selected TopicsRating: 5 out of 5 stars5/5 (1)
- RJZ 269Document3 pagesRJZ 269Saffa AzharaaniNo ratings yet
- 20 +ok+ (11) +Jose+Mandei+146-156+doiDocument11 pages20 +ok+ (11) +Jose+Mandei+146-156+doiSaffa AzharaaniNo ratings yet
- Ojo 2021092215172319Document10 pagesOjo 2021092215172319Saffa AzharaaniNo ratings yet
- Changes Metabolic Parameters Body Weight Prediabetes JCP 23m14786Document15 pagesChanges Metabolic Parameters Body Weight Prediabetes JCP 23m14786Saffa AzharaaniNo ratings yet
- JIG Vol 1 No 4 Oktober 2023 Hal 10-15Document6 pagesJIG Vol 1 No 4 Oktober 2023 Hal 10-15Saffa AzharaaniNo ratings yet
- 1 s2.0 S2049080122002709 Main 2Document4 pages1 s2.0 S2049080122002709 Main 2Saffa AzharaaniNo ratings yet
- Jove 96 52238Document10 pagesJove 96 52238Saffa AzharaaniNo ratings yet
- Pamj 33 234Document8 pagesPamj 33 234Saffa AzharaaniNo ratings yet
- Chliaoutakis 2002Document13 pagesChliaoutakis 2002Saffa AzharaaniNo ratings yet
- 1 s2.0 S1078588413007946 Main 2Document7 pages1 s2.0 S1078588413007946 Main 2Saffa AzharaaniNo ratings yet
- s40634 021 00334 1Document6 pagess40634 021 00334 1Saffa AzharaaniNo ratings yet
- Prognosis of Pulmonary: TuberculosisDocument5 pagesPrognosis of Pulmonary: TuberculosisSaffa AzharaaniNo ratings yet
- OTCN4 TH EditionDocument13 pagesOTCN4 TH EditionSaffa AzharaaniNo ratings yet
- The Effect of Problem-Based Learning On Learning Outcomes of Accounting StudentsDocument20 pagesThe Effect of Problem-Based Learning On Learning Outcomes of Accounting StudentsSaffa AzharaaniNo ratings yet
- DD CommandsDocument30 pagesDD CommandsAdriana Hernandez YescasNo ratings yet
- 2017 Mohammad-ThesisDocument128 pages2017 Mohammad-ThesisLetalis IraNo ratings yet
- Design of ColumnsDocument20 pagesDesign of ColumnsnoahNo ratings yet
- Last Area Day 8 - Basic Electronics-1Document7 pagesLast Area Day 8 - Basic Electronics-1ellajanepoNo ratings yet
- Motion DimensionDocument113 pagesMotion DimensionMaya Satih KanteyanNo ratings yet
- Photo Mechanic 4.5.3 ManualDocument132 pagesPhoto Mechanic 4.5.3 ManualRodrigo Franco Carlovich MoreiraNo ratings yet
- JasperReports Server REST API Reference PDFDocument174 pagesJasperReports Server REST API Reference PDFJosé Antonio Gómez ViracaNo ratings yet
- Doors EntryDocument4 pagesDoors EntryAndrea Nicola TurcatoNo ratings yet
- Notas Experimento MeldeDocument7 pagesNotas Experimento MeldeArielPonceNo ratings yet
- CCCCC PDFDocument1 pageCCCCC PDFGanapathi RajNo ratings yet
- Technicalproposal: For 750kva Substation EquipmentDocument4 pagesTechnicalproposal: For 750kva Substation EquipmentHarun MohamodNo ratings yet
- SN 1 Jul 2013 NTNU Wind Turbine Drivtrain CeSOSDocument8 pagesSN 1 Jul 2013 NTNU Wind Turbine Drivtrain CeSOSanteoprivatoNo ratings yet
- Cs101 Program Logic Formulation 1Document4 pagesCs101 Program Logic Formulation 1Multiple Criteria DssNo ratings yet
- Structural Tubing Square Dimensions and PropertiesDocument11 pagesStructural Tubing Square Dimensions and Propertiesnando riskyNo ratings yet
- Crime Type and Occurrence Prediction Using Machine LearningDocument28 pagesCrime Type and Occurrence Prediction Using Machine Learninggateway.manigandanNo ratings yet
- Catalogo de RodamientosDocument399 pagesCatalogo de RodamientosmarragezNo ratings yet
- Infinity Other Solar Systems: TrinityDocument1 pageInfinity Other Solar Systems: TrinityP Eng Suraj SinghNo ratings yet
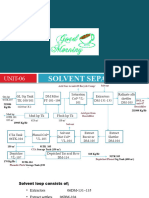
- Solvent Separation UNIT-06 - GOODDocument17 pagesSolvent Separation UNIT-06 - GOODAamir HasanNo ratings yet
- MOCK - TEST - (Chemistry) - Term 1 - 2015Document19 pagesMOCK - TEST - (Chemistry) - Term 1 - 2015Ung Hie HuongNo ratings yet
- How To Turn Your TP Link TL-WRT740N Router Into A Fully Functional One Using OpenWRT PhobosK's BlogDocument25 pagesHow To Turn Your TP Link TL-WRT740N Router Into A Fully Functional One Using OpenWRT PhobosK's BlogpedjavgdNo ratings yet
- RT430 RT434 GNSS TM EN HWB 8v4Document107 pagesRT430 RT434 GNSS TM EN HWB 8v4Carlos Sulca NeiraNo ratings yet
- Air DryersDocument4 pagesAir Dryersmanpreetsodhi08No ratings yet
- High Impedance Fault Detection Using Multi Domain Feature With Artificial Neural NetworkDocument15 pagesHigh Impedance Fault Detection Using Multi Domain Feature With Artificial Neural NetworkANKAN CHANDRANo ratings yet
- Module 7 - Acting and Performance in AnimationDocument24 pagesModule 7 - Acting and Performance in AnimationLovely Jenn ReformadoNo ratings yet
- TSJ Transportation Frame General NotesDocument1 pageTSJ Transportation Frame General NotesBhuvan GanesanNo ratings yet
- Elementary Differential Equations BookDocument183 pagesElementary Differential Equations BookabadittadesseNo ratings yet
- Math (F4) - Straight Line 5.1Document33 pagesMath (F4) - Straight Line 5.1Roszelan MajidNo ratings yet
- 2017 Catalog 99812723Document508 pages2017 Catalog 99812723Valco0% (1)
- ABAP Dictionary NotesDocument11 pagesABAP Dictionary NotesYousif AhmedNo ratings yet