Download as pdf or txt
You might also like
- Level II QuestionsDocument8 pagesLevel II Questionsabdallah250057% (7)
- Radiation Biology LectureDocument39 pagesRadiation Biology LectureBipin UpadhyayNo ratings yet
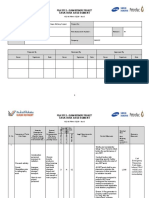
- Task Risk Assessment: PSJV Epc 2 - Duqm Refinery ProjectDocument16 pagesTask Risk Assessment: PSJV Epc 2 - Duqm Refinery Projectrodman823100% (2)
- Icru 16Document59 pagesIcru 16Alvaro Hermosilla Manríquez0% (1)
- Biological Effects of Ionizing Radiation: En. Mohd Fahmi B Mohd YusofDocument45 pagesBiological Effects of Ionizing Radiation: En. Mohd Fahmi B Mohd YusofFahmi BestNo ratings yet
- Biological Effects of Radiation (Physics)Document13 pagesBiological Effects of Radiation (Physics)Josiah Dave CalumpangNo ratings yet
- Radiobiology LectureDocument5 pagesRadiobiology LectureChukwu BlessingNo ratings yet
- Radiation Units and Biological Effects of RadiationDocument67 pagesRadiation Units and Biological Effects of RadiationSivirahul100% (2)
- Bilogical Effects and RisksDocument33 pagesBilogical Effects and RisksVictor LusamboNo ratings yet
- Biological Effects of Radiation: Sayan Samanta BWU/BRI/21/109Document10 pagesBiological Effects of Radiation: Sayan Samanta BWU/BRI/21/109Sayan SamantaNo ratings yet
- Nuclear Medicine 7 (Radiation Risk and Exposure)Document33 pagesNuclear Medicine 7 (Radiation Risk and Exposure)Najeeb Ullah Qadir via GTXNo ratings yet
- 10 - Radiation Biological EffectsDocument30 pages10 - Radiation Biological EffectsAbdullah El-ZaaboutNo ratings yet
- 259 FullDocument6 pages259 Fullmohammedfahadtvm493No ratings yet
- Biological Effects of RadiationDocument7 pagesBiological Effects of Radiationbpvarian100% (1)
- Biological Effects of Radiation & Safety ConsiderationDocument21 pagesBiological Effects of Radiation & Safety ConsiderationTareq AzizNo ratings yet
- Submitted by Registration Number-Roll Number - Section Submitted ToDocument28 pagesSubmitted by Registration Number-Roll Number - Section Submitted ToPriyanka JaswalNo ratings yet
- Biological Effect of Radiation 3Document8 pagesBiological Effect of Radiation 3Dannis VNo ratings yet
- Biological Effects of RadiationDocument32 pagesBiological Effects of Radiationmelannie adanteNo ratings yet
- BME481 Lecture5 PartIII Radiation Dose and RiskDocument28 pagesBME481 Lecture5 PartIII Radiation Dose and RiskMalekNo ratings yet
- Nuclear Radiation RiskDocument16 pagesNuclear Radiation RiskScribdTranslationsNo ratings yet
- Lalitbiological 2014Document8 pagesLalitbiological 2014Việt QuốcNo ratings yet
- RadiobiologyDocument70 pagesRadiobiologypia toledoNo ratings yet
- Ionization and Cell DamageDocument2 pagesIonization and Cell DamageMomo ItachiNo ratings yet
- Basic Biologic Interactions of RadiationDocument28 pagesBasic Biologic Interactions of RadiationAyu FadhilahNo ratings yet
- Biological Effects of Radiation IAEADocument87 pagesBiological Effects of Radiation IAEAkhushi786100% (1)
- Radio BiologyDocument7 pagesRadio BiologyLucelle CoquillaNo ratings yet
- Radioactive PollutionDocument18 pagesRadioactive PollutionKanishq BawejaNo ratings yet
- Biological Effects of Ionizing Radiation-2022Document138 pagesBiological Effects of Ionizing Radiation-2022Waleed TayyabNo ratings yet
- Class2 TypesOfDamage ARSDocument60 pagesClass2 TypesOfDamage ARSQassem MohaidatNo ratings yet
- Stochastic and Deterministic Effects of Radiation? AnswerDocument3 pagesStochastic and Deterministic Effects of Radiation? AnswerzahidNo ratings yet
- CSBC-321 Elementary of Human PhysiologyDocument9 pagesCSBC-321 Elementary of Human PhysiologyJessieNo ratings yet
- Assignment of Nuclear ChemistryDocument3 pagesAssignment of Nuclear ChemistryMubashir Hassan KhanNo ratings yet
- Lecture - 2 - Bioradiation Radiation Biology - Mechanisms - 1Document7 pagesLecture - 2 - Bioradiation Radiation Biology - Mechanisms - 1Naglaa MostafaNo ratings yet
- Basic Review of Radiation Biology and TerminologyDocument7 pagesBasic Review of Radiation Biology and TerminologyAjay MohanNo ratings yet
- Nuclear Pollution and Its Biological Effects: Presented By: Archit Sharma Sahil Mohd - Ali Khan Amity University HaryanaDocument22 pagesNuclear Pollution and Its Biological Effects: Presented By: Archit Sharma Sahil Mohd - Ali Khan Amity University HaryanaSahil VatsNo ratings yet
- Bioloical Effects and Hazards of RadiationDocument19 pagesBioloical Effects and Hazards of Radiationnabawenda. joan.2019No ratings yet
- Radioactive PollutionDocument2 pagesRadioactive PollutionIulia VladNo ratings yet
- Electromagnetic Radiations and Properties of X-RaysDocument57 pagesElectromagnetic Radiations and Properties of X-RaysRosette DawoudNo ratings yet
- Radio Biophysics Level 3Document74 pagesRadio Biophysics Level 3Naglaa MostafaNo ratings yet
- Basic Radiation BiologyDocument25 pagesBasic Radiation Biologysazaki224No ratings yet
- Radiobiology 1Document36 pagesRadiobiology 1Santanu SamantaNo ratings yet
- Glenda Chivandire H180109H Equipment Assignment 1 MR Mutasa 2021Document6 pagesGlenda Chivandire H180109H Equipment Assignment 1 MR Mutasa 2021eltonNo ratings yet
- Ch. 37 Biomedical PhyDocument23 pagesCh. 37 Biomedical PhyMahmoud Abu MayalehNo ratings yet
- Biological Effects of RadiationDocument28 pagesBiological Effects of RadiationRoydenPTNo ratings yet
- Biological Effects of RadiationDocument28 pagesBiological Effects of RadiationShahzaib Ahmad ZiaNo ratings yet
- YG Biological EffectDocument13 pagesYG Biological EffectMariel Peña CuadrosNo ratings yet
- Trauma & Cell InjuryDocument27 pagesTrauma & Cell InjuryTauqeer AhmedNo ratings yet
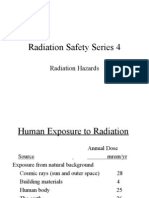
- Radiation Saftey Series 4Document26 pagesRadiation Saftey Series 4johntoblerNo ratings yet
- Units of Radiation DoseDocument20 pagesUnits of Radiation DoseMadduri NithamNo ratings yet
- Occupational Radiation Safety: Directed Readings in The ClassroomDocument54 pagesOccupational Radiation Safety: Directed Readings in The ClassroomErick Calcaligong100% (2)
- Biological Effects of RadiationDocument28 pagesBiological Effects of Radiationk_472894540No ratings yet
- En 417 ProjectDocument23 pagesEn 417 Project2K18/ME/202 SAURAV BANSALNo ratings yet
- Icrp2013 s2 DorrDocument11 pagesIcrp2013 s2 DorrEdis ĐedovićNo ratings yet
- 42 - Principles of Cancer TherapyDocument54 pages42 - Principles of Cancer TherapyLucero BautistaNo ratings yet
- Effects of Radiation On FoetusDocument3 pagesEffects of Radiation On FoetusMubashir Hassan KhanNo ratings yet
- 4.bilogical EffectsDocument56 pages4.bilogical Effectswajira sanjaya pereraNo ratings yet
- Photobiology 1 - 231103 - 171019Document25 pagesPhotobiology 1 - 231103 - 171019eslam.h.mohamed1No ratings yet
- Biological Effects of RadiationDocument15 pagesBiological Effects of RadiationShaikh SalmanNo ratings yet
- Reviews: Effects of Radiation On Normal Tissue: Consequences and MechanismsDocument8 pagesReviews: Effects of Radiation On Normal Tissue: Consequences and Mechanismssardartalabany2No ratings yet
- Radiation Hazards and Protection HandoutDocument7 pagesRadiation Hazards and Protection Handoutعبد المنعم حسنNo ratings yet
- Laser / IPL Technology for Skin Care: A Comprehensive Technical and Informative TextbookFrom EverandLaser / IPL Technology for Skin Care: A Comprehensive Technical and Informative TextbookRating: 4 out of 5 stars4/5 (8)
- Cell and Molecular Biology: An Introductory Guide for Learning Cellular & Molecular BiologyFrom EverandCell and Molecular Biology: An Introductory Guide for Learning Cellular & Molecular BiologyNo ratings yet
- Anatomy of The Upper LimbDocument1 pageAnatomy of The Upper Limb202210034No ratings yet
- Purines, Pyrimidine MetabolismDocument22 pagesPurines, Pyrimidine Metabolism202210034No ratings yet
- Metabolism of XenobioticsDocument9 pagesMetabolism of Xenobiotics202210034No ratings yet
- Lecture 12 Molecular BiologyDocument231 pagesLecture 12 Molecular Biology202210034No ratings yet
- Blood 1-2 HemopoiesisDocument25 pagesBlood 1-2 Hemopoiesis202210034No ratings yet
- Blood 3-4 HemoglobinDocument14 pagesBlood 3-4 Hemoglobin202210034No ratings yet
- Autonomic Nervous System QuestionsDocument6 pagesAutonomic Nervous System Questions202210034No ratings yet
- Introduction To InterpretationDocument22 pagesIntroduction To Interpretation202210034No ratings yet
- Radiation ProtectionDocument31 pagesRadiation Protection202210034No ratings yet
- 1-General PharmacologyDocument59 pages1-General Pharmacology202210034No ratings yet
- Department of Physics Department of Physics Department of PhysicsDocument235 pagesDepartment of Physics Department of Physics Department of Physicstatis reyesNo ratings yet
- 5415035-1EN Rev 03 9800 9900 Regulatory Reference ChartDocument22 pages5415035-1EN Rev 03 9800 9900 Regulatory Reference ChartJonathan WoodwardNo ratings yet
- Reg0012 - KVP Accuracy: 1 Personnel RequirementsDocument66 pagesReg0012 - KVP Accuracy: 1 Personnel RequirementsGeorgiana KokonaNo ratings yet
- Radiographic Testing: Compiled For ASNT by Bahman Zoofan The Ohio State UniversityDocument293 pagesRadiographic Testing: Compiled For ASNT by Bahman Zoofan The Ohio State UniversityTrajko GorgievskiNo ratings yet
- Development OfpointkernelDocument13 pagesDevelopment Ofpointkernelbilguun_byambadorjNo ratings yet
- RadiotherapyDocument60 pagesRadiotherapyAARYANo ratings yet
- Training On RT - ASNT Level IIDocument72 pagesTraining On RT - ASNT Level IIAguara OghenevwedeNo ratings yet
- Icrp 113Document35 pagesIcrp 113Mario GarcíaNo ratings yet
- 1-'Introduction To Imaging ModalitiesDocument26 pages1-'Introduction To Imaging Modalitiesmohameeedar1No ratings yet
- Radiology and Radiation SafetyDocument4 pagesRadiology and Radiation Safetycoordinator.dargaiNo ratings yet
- SAFC Biosciences Research Report - Validated Gamma Irradiated Trypsin PowderDocument4 pagesSAFC Biosciences Research Report - Validated Gamma Irradiated Trypsin PowderSAFC-GlobalNo ratings yet
- Pediatric RadiographyDocument31 pagesPediatric RadiographyHakim Abdul Pakaya100% (3)
- CT-PET Shielding DesingDocument24 pagesCT-PET Shielding DesingGezim Hodolli100% (1)
- Dosimetric Models of The Eye and LensDocument21 pagesDosimetric Models of The Eye and LensIshani Anushika JayakodyNo ratings yet
- Radiation Safety Paper - Kristen DezellDocument4 pagesRadiation Safety Paper - Kristen Dezellapi-568316609No ratings yet
- Anritsu XRay Inspection OverviewDocument12 pagesAnritsu XRay Inspection Overviewyobeli7912No ratings yet
- Dose Amd Eq DoseDocument30 pagesDose Amd Eq DoseKhalid AbeedNo ratings yet
- Brachytherapy in The Treatment of Cervical CancerDocument10 pagesBrachytherapy in The Treatment of Cervical CancervchendilNo ratings yet
- DR 100s (English - Brochure)Document9 pagesDR 100s (English - Brochure)jacksmar prietoNo ratings yet
- 15McEwen PrimaryStandardsfinalforVLDocument69 pages15McEwen PrimaryStandardsfinalforVLCristian GondacNo ratings yet
- MedPhysTerm-KSMP First Version (200906)Document216 pagesMedPhysTerm-KSMP First Version (200906)Ilkuk EomNo ratings yet
- Aapm Tg114 Mu CalcDocument27 pagesAapm Tg114 Mu CalcHuntingparxxNo ratings yet
- Digital RT PPT (04.04.2018)Document134 pagesDigital RT PPT (04.04.2018)AURORA NDT Services75% (4)
- Handheld X-Ray System: For Intraoral Radiographic ImagingDocument44 pagesHandheld X-Ray System: For Intraoral Radiographic Imagingdie6o_brNo ratings yet
- Validation of A Virtual Source Model For Monte Carlo Dose Calculations of A FFF LinacDocument8 pagesValidation of A Virtual Source Model For Monte Carlo Dose Calculations of A FFF LinacJoseLuisDumontNo ratings yet
- Multiple Choice RadioactivityDocument4 pagesMultiple Choice RadioactivityGodhrawala AliasgerNo ratings yet
- IAEA - Radiation Protection For LINACsDocument343 pagesIAEA - Radiation Protection For LINACsSuhey07100% (1)