Download as pdf or txt
You might also like
- Eating Our Way To ExtinctionDocument2 pagesEating Our Way To ExtinctionJohanna0% (1)
- Career Barriers InventoryDocument107 pagesCareer Barriers InventoryAsya AlğanNo ratings yet
- Grief and Grief ReactionsDocument37 pagesGrief and Grief ReactionsjaydipNo ratings yet
- The Cornerhouse Forensic Interview Protocol: An Evolution in Practice For Almost 25 YearsDocument6 pagesThe Cornerhouse Forensic Interview Protocol: An Evolution in Practice For Almost 25 Yearsmaria ochoa100% (1)
- NRG 305 Chapter 5Document7 pagesNRG 305 Chapter 5peachesbang00No ratings yet
- Psychiatric Nursing ReviewerDocument20 pagesPsychiatric Nursing ReviewerCatherine Kaye PerezNo ratings yet
- Grief, Stages of Grief and Grief ProcessDocument6 pagesGrief, Stages of Grief and Grief ProcessEdrea Aquino Mendez100% (2)
- Grief Loss and Dying Week 11Document18 pagesGrief Loss and Dying Week 11Shaquilla TrappNo ratings yet
- Grief, Mourning and BereavementDocument5 pagesGrief, Mourning and BereavementDoc Prince Caballero100% (1)
- Death and DyingDocument4 pagesDeath and DyingGalvez Glaiza Elaine100% (1)
- Health PPT 4Document13 pagesHealth PPT 4Lemuel Español CamusNo ratings yet
- Grief and Loss, Dying/ DeadDocument5 pagesGrief and Loss, Dying/ DeadAaron ConstantinoNo ratings yet
- Loss & End of Life IssuesDocument4 pagesLoss & End of Life IssuesLalaine NadulpitNo ratings yet
- What Is Grief-1Document3 pagesWhat Is Grief-1api-665652347No ratings yet
- GriefDocument9 pagesGriefashishsipaiNo ratings yet
- Grief and Bereavement Training OneDocument22 pagesGrief and Bereavement Training OneSamantha MokgothuNo ratings yet
- Grieving in ElderlyDocument29 pagesGrieving in Elderlyjuss100% (1)
- End of Life Issues and Palliative Care: Presented by - Dr. Riya Singh Junior Resident 1Document10 pagesEnd of Life Issues and Palliative Care: Presented by - Dr. Riya Singh Junior Resident 1RiyaSinghNo ratings yet
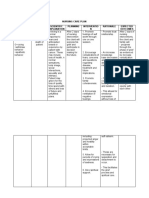
- NCP Case StudyDocument2 pagesNCP Case StudyGerome Isaiah RabangNo ratings yet
- 2 Dying Death and GrievingDocument54 pages2 Dying Death and Grievingi & vNo ratings yet
- Chapter 29 The Experience of Loss, Death and GriefDocument4 pagesChapter 29 The Experience of Loss, Death and GriefCARL JOHN MANALONo ratings yet
- GRIEF - NotesDocument3 pagesGRIEF - NotesNehalNo ratings yet
- End of Life Care Death & GriefDocument48 pagesEnd of Life Care Death & GriefJoanna RachelNo ratings yet
- Grief & Loss Presentation (Teens & Young Adults Presentation)Document17 pagesGrief & Loss Presentation (Teens & Young Adults Presentation)Nicole RiveraNo ratings yet
- Care of Terminally Ill PatientDocument64 pagesCare of Terminally Ill PatientSilpa Jose TNo ratings yet
- End of Life Care and IssuesDocument9 pagesEnd of Life Care and Issuesliana.s.vegaNo ratings yet
- The Experience of Loss, Death and GriefDocument14 pagesThe Experience of Loss, Death and GriefAries Gulle MacalamNo ratings yet
- Coping With LossDocument5 pagesCoping With LossRaman SamraoNo ratings yet
- Loss Grief and DeathDocument8 pagesLoss Grief and DeathFrauline YapNo ratings yet
- Loss, Grieving, Death and Post Mortem CareDocument14 pagesLoss, Grieving, Death and Post Mortem CareBill Conrad C AdriculaNo ratings yet
- Discharge Care and RehabilitationDocument1 pageDischarge Care and RehabilitationRosmaryNo ratings yet
- Coping With Loss Griving 0 DeathDocument16 pagesCoping With Loss Griving 0 DeathSandhya Gupta100% (1)
- Mental Health NursingDocument37 pagesMental Health NursingjaydipNo ratings yet
- Dealing With Grief and LossDocument15 pagesDealing With Grief and Lossharrison machariaNo ratings yet
- Psychiatric Nursing ReviewerDocument20 pagesPsychiatric Nursing ReviewerLezel LaracasNo ratings yet
- Grief and TraumaDocument7 pagesGrief and TraumaMoonlight sweetheartNo ratings yet
- Topic 4Document11 pagesTopic 4Patricia Mae MurilloNo ratings yet
- Loss, Grief and Grieving ProcessDocument28 pagesLoss, Grief and Grieving ProcessSuper .K. music lyricsNo ratings yet
- Death and GrievingDocument25 pagesDeath and GrievingAmanda Scarlet100% (1)
- LOSS GRIEVING DEATH FinalsDocument72 pagesLOSS GRIEVING DEATH FinalsamaNo ratings yet
- Chapter 4 Personal and Mental HealthDocument25 pagesChapter 4 Personal and Mental HealthJyuan DavidNo ratings yet
- CCM PresentationDocument20 pagesCCM PresentationVarunPratapMehtaNo ratings yet
- Death and DyingDocument66 pagesDeath and DyingMc Ramil B. PraderoNo ratings yet
- Chapter 10 Grief and LossDocument6 pagesChapter 10 Grief and LossCatia FernandesNo ratings yet
- Personality DisorderDocument3 pagesPersonality DisorderazealealizNo ratings yet
- Anticipatory GrievingDocument2 pagesAnticipatory GrievingKM100% (5)
- Grief Resolution TherapyDocument51 pagesGrief Resolution TherapySandesh HegdeNo ratings yet
- Care of Terminally Ill Set 1Document27 pagesCare of Terminally Ill Set 1saranya amuNo ratings yet
- NCP - Indi CSDocument6 pagesNCP - Indi CSFretzgine Lou ManuelNo ratings yet
- Coping With Loss Death and GrievingDocument33 pagesCoping With Loss Death and Grievingsalmanhabeebek100% (1)
- Coping With Loss, Grief, DeathDocument23 pagesCoping With Loss, Grief, Deathsoumya sathesh100% (1)
- Psychological Reactions To Death and Dying FinalDocument31 pagesPsychological Reactions To Death and Dying FinalSaad khanNo ratings yet
- Death and Dying Grief and LossDocument28 pagesDeath and Dying Grief and LossromeojrNo ratings yet
- GS5 - Janina Fisher - Plenary Healing The Fragmented Self HandoutDocument12 pagesGS5 - Janina Fisher - Plenary Healing The Fragmented Self HandoutMargaret Kelomees100% (1)
- Supporting Patients Who Are BereavedDocument5 pagesSupporting Patients Who Are BereavedVictoria AlmeidaNo ratings yet
- Loss, Grief, Bereavement, and MourningDocument33 pagesLoss, Grief, Bereavement, and Mourningkirti thakurNo ratings yet
- Clinical Features of Grief and Management of Grief: Presenter Jyothsna.K.ADocument27 pagesClinical Features of Grief and Management of Grief: Presenter Jyothsna.K.AJonty ArputhemNo ratings yet
- Personality DisordersDocument3 pagesPersonality Disordersvzantua.k11831205No ratings yet
- Foundation of Nursing Ii - by Masino T (BSC, MSC)Document29 pagesFoundation of Nursing Ii - by Masino T (BSC, MSC)Seud BehruNo ratings yet
- Trauma-Informed Care Resources Guide: Cpi Exclusive DownloadDocument14 pagesTrauma-Informed Care Resources Guide: Cpi Exclusive DownloadHasrat ButtarNo ratings yet
- Module 4 HandoutsDocument20 pagesModule 4 HandoutsAlazar DejeneNo ratings yet
- NCP CholeraDocument4 pagesNCP CholeraARISNo ratings yet
- Chapter 10 - BloodDocument14 pagesChapter 10 - BloodrishellemaepilonesNo ratings yet
- Microbial Disease On Gastrointestinal SystemDocument2 pagesMicrobial Disease On Gastrointestinal SystemrishellemaepilonesNo ratings yet
- TFN ReviewDocument32 pagesTFN ReviewrishellemaepilonesNo ratings yet
- Summary of Major Minerals and Trace ElementsDocument2 pagesSummary of Major Minerals and Trace ElementsrishellemaepilonesNo ratings yet
- Module 11 - Instructional SettingsDocument2 pagesModule 11 - Instructional SettingsrishellemaepilonesNo ratings yet
- Stage 6 - Modern History Unit of WorkDocument18 pagesStage 6 - Modern History Unit of Workapi-532442874No ratings yet
- The Physical Self: The Self As Impacted by The Body: How Well Do I Know My Physical Self?Document35 pagesThe Physical Self: The Self As Impacted by The Body: How Well Do I Know My Physical Self?Angelica CervantesNo ratings yet
- Bus 428Document236 pagesBus 428Emeka Ken Nwosu100% (1)
- Roger BastideDocument2 pagesRoger BastideAna Cristina100% (1)
- When Does Transformational Leadership Enhance Employee Proactive Behavior The Role of Autonomy and Role Breadth Efficacy.Document10 pagesWhen Does Transformational Leadership Enhance Employee Proactive Behavior The Role of Autonomy and Role Breadth Efficacy.Ana GNo ratings yet
- Exploratory, Descrptive and Causal - Chapter 5Document6 pagesExploratory, Descrptive and Causal - Chapter 5Mahmoud SaeedNo ratings yet
- Introduction To The Philosophy of The Human Person: Subject SyllabusDocument8 pagesIntroduction To The Philosophy of The Human Person: Subject SyllabusAmadh PereyraNo ratings yet
- Traumata and ConsequencesFr RuppertDocument36 pagesTraumata and ConsequencesFr Ruppertrodicachirculescu100% (1)
- STA630 Assignment 2 SolutionDocument1 pageSTA630 Assignment 2 SolutionMãryåm ChNo ratings yet
- The Audience: Oral PresentationDocument2 pagesThe Audience: Oral PresentationrealNo ratings yet
- Bovee bct13 Inppt 14Document33 pagesBovee bct13 Inppt 14mzNo ratings yet
- Managerial CompetenciesDocument49 pagesManagerial CompetenciesJagannath Shashank Vadrevu100% (1)
- Moral 1: Slow & Steady Wins The RaceDocument71 pagesMoral 1: Slow & Steady Wins The RaceFall Out BoyzNo ratings yet
- Art of TeachingDocument39 pagesArt of Teachingchongtong100% (1)
- FINAL PR2 Group 5Document46 pagesFINAL PR2 Group 5Alex AlegreNo ratings yet
- Lesson Plan: Values and AttitudesDocument4 pagesLesson Plan: Values and Attitudesapi-313436217No ratings yet
- Lesson 1 - Nature and Process of CommunicationDocument59 pagesLesson 1 - Nature and Process of CommunicationJaoe Mae NavallascaNo ratings yet
- A Planning Docx Senior High TemplateDocument6 pagesA Planning Docx Senior High TemplateSheryline BonillaNo ratings yet
- Gen. Ed 1Document19 pagesGen. Ed 1Arleen TalamayanNo ratings yet
- Teaching To Learn, Learning To TeachDocument4 pagesTeaching To Learn, Learning To Teachシティ ctNo ratings yet
- Interview Skills Competency Based Questions Factsheet FinalDocument7 pagesInterview Skills Competency Based Questions Factsheet FinalYeshwanth VarmaNo ratings yet
- Teacher Observation Form - Google FormsDocument16 pagesTeacher Observation Form - Google FormsGrace KwongNo ratings yet
- Bowlbys Attachment TheoryDocument10 pagesBowlbys Attachment Theoryapi-276414713No ratings yet
- Mental HealthDocument16 pagesMental HealthAna rose VeluntaNo ratings yet
- Cek SoalDocument6 pagesCek SoalYunita De' AlayNo ratings yet
- Reading Artifact Reflectionstandard7planningDocument4 pagesReading Artifact Reflectionstandard7planningapi-292471312No ratings yet
- TfZG0xOISK6gEYBLWXrC Learningact Resource GuideDocument26 pagesTfZG0xOISK6gEYBLWXrC Learningact Resource GuideMarco PNo ratings yet