Download as doc, pdf, or txt
You might also like
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5820)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1093)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (852)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (590)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (898)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (540)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (349)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (822)
- FINAL EXAM Advanced Health Assessment and Diagnostic ReasoningDocument15 pagesFINAL EXAM Advanced Health Assessment and Diagnostic ReasoningGeorge Ekai100% (2)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (122)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (403)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- Earth Clinic - Borax Cures and Health BenefitsDocument4 pagesEarth Clinic - Borax Cures and Health BenefitsLife Force Energy Plasterite100% (2)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- Gender SensitivityDocument10 pagesGender Sensitivityapi-3704562100% (10)
- Gender SensitivityDocument2 pagesGender Sensitivityapi-370456296% (26)
- SURGERYDocument36 pagesSURGERYapi-3704562No ratings yet
- PulmoconDocument64 pagesPulmoconapi-3704562100% (1)
- Vasculitis SyndromesDocument9 pagesVasculitis Syndromesapi-3704562No ratings yet
- Dr. JTG Presentation (Diarrheas)Document33 pagesDr. JTG Presentation (Diarrheas)api-3704562No ratings yet
- PlasticischwartsDocument3 pagesPlasticischwartsapi-3704562No ratings yet
- Kaplan Community EpidemDocument3 pagesKaplan Community Epidemapi-3704562No ratings yet
- SLE SummaryDocument5 pagesSLE Summaryapi-3704562100% (1)
- Bacterial and Viral MeningitisDocument12 pagesBacterial and Viral Meningitisapi-3704562100% (1)
- Neurosurgery Case 1Document111 pagesNeurosurgery Case 1api-3704562No ratings yet
- Psych AdjustmentDocument2 pagesPsych Adjustmentapi-3704562No ratings yet
- CHAPTER 127 MENINGOCOCCAL INFECTIONS SummaryDocument3 pagesCHAPTER 127 MENINGOCOCCAL INFECTIONS Summaryapi-3704562No ratings yet
- Ringkasan MeningitisDocument2 pagesRingkasan Meningitisd17oNo ratings yet
- HUMAN HERPES VIRUS Types 6Document1 pageHUMAN HERPES VIRUS Types 6api-3704562100% (1)
- NCMB316: Compilation Finals in NCMB316Document23 pagesNCMB316: Compilation Finals in NCMB316Armand Bong Santiago100% (1)
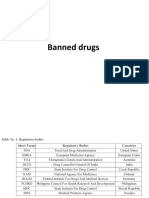
- Banned DrugsDocument26 pagesBanned DrugskarthikeyanpgtNo ratings yet
- Maternal Physiology: Metabolic Changes Hematological ChangesDocument33 pagesMaternal Physiology: Metabolic Changes Hematological ChangesironNo ratings yet
- WEBSITE SchemesDocument48 pagesWEBSITE SchemesVivek LuckyNo ratings yet
- 10.1016/j.ymgme.2016.11.045: Abstracts / Molecular Genetics and Metabolism 120 (2016) S17 - S145 S29Document2 pages10.1016/j.ymgme.2016.11.045: Abstracts / Molecular Genetics and Metabolism 120 (2016) S17 - S145 S29Larisa IliescuNo ratings yet
- Paper 2 Biology 1995 Paper 2+ansDocument30 pagesPaper 2 Biology 1995 Paper 2+ansapi-3812894No ratings yet
- BASIC CONCEPTS IN MEDICINAL CHEMISTRY, 3RD EDITION. (MARC W.. ZAVOD HARROLD (ROBIN M.) ) (Z-Library)Document1 pageBASIC CONCEPTS IN MEDICINAL CHEMISTRY, 3RD EDITION. (MARC W.. ZAVOD HARROLD (ROBIN M.) ) (Z-Library)duy luuNo ratings yet
- Anatomy Mnemonics: Diaphragm Apertures: Spinal LevelsDocument22 pagesAnatomy Mnemonics: Diaphragm Apertures: Spinal Levelsagar agarNo ratings yet
- Pacemakers, Heart BlocksDocument31 pagesPacemakers, Heart BlockscindybevNo ratings yet
- Diabetic Retinopathy Detection Using Deep Learning: January 2022Document8 pagesDiabetic Retinopathy Detection Using Deep Learning: January 2022Hello ThereNo ratings yet
- Acute Biologic Crisis: Nina Hamili G. Piao RNDocument62 pagesAcute Biologic Crisis: Nina Hamili G. Piao RNNina OaipNo ratings yet
- An Analysis of The Causes of Mental IllnessDocument9 pagesAn Analysis of The Causes of Mental IllnessDanish AhmadNo ratings yet
- Jyane ReubenDocument35 pagesJyane ReubenAmr El-RefaeyNo ratings yet
- Smart PillDocument2 pagesSmart Pillpappu khanNo ratings yet
- Nephrology Final Spring 2020Document8 pagesNephrology Final Spring 2020Srinivas PingaliNo ratings yet
- Varicose Veins: Dr. Yonas G. (MD)Document18 pagesVaricose Veins: Dr. Yonas G. (MD)Mikiale kirosNo ratings yet
- The Basis of Brain Rehab by Dr. John Hatch Inspires and Provides Renewed Hope To Anyone Looking To Improve Their Health Available On Amazon and Audible Thursday, May 4thDocument3 pagesThe Basis of Brain Rehab by Dr. John Hatch Inspires and Provides Renewed Hope To Anyone Looking To Improve Their Health Available On Amazon and Audible Thursday, May 4thPR.comNo ratings yet
- Cardiac Catheterization - Post ProcedureDocument2 pagesCardiac Catheterization - Post ProcedureHendi Refiaguna100% (1)
- Daftar PustakaDocument2 pagesDaftar PustakaSalwiyadiNo ratings yet
- I'll See You Tomorrow: Ayza Bolanos Autobiographical Reading and Writing Brett Williams 09 December 2015Document30 pagesI'll See You Tomorrow: Ayza Bolanos Autobiographical Reading and Writing Brett Williams 09 December 2015api-357172052No ratings yet
- Somatic UmbrellaDocument10 pagesSomatic UmbrellaYiomarie Ojeda-Rodz100% (1)
- Pulmonary Embolism: Presented By: Miss. M.K.Kaku Nursing TutorDocument9 pagesPulmonary Embolism: Presented By: Miss. M.K.Kaku Nursing TutorKaku ManishaNo ratings yet
- Clinical ManualDocument75 pagesClinical ManualAdri Fortin de CosenzaNo ratings yet
- Protein Energy Malnutrition SethDocument55 pagesProtein Energy Malnutrition SethKojo Duncan100% (1)
- Catch Up Friday Feb 29Document4 pagesCatch Up Friday Feb 29leicatapangNo ratings yet
- DES With AnswerDocument123 pagesDES With AnswersoksothyspsNo ratings yet
- Swarnaprashana PDFDocument9 pagesSwarnaprashana PDFAnuroop MondruNo ratings yet
- CVS/ The Blood Vessels: by DR - Ahmed Avdel MandaniDocument27 pagesCVS/ The Blood Vessels: by DR - Ahmed Avdel MandaniSerwan J AbdulrahmanNo ratings yet