Download as pdf or txt
You might also like
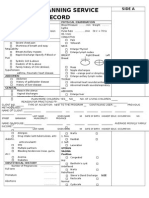
- Family Planning Service RecordDocument3 pagesFamily Planning Service RecordRJay Mon Marcos100% (2)
- Gyne - Benign LesionsDocument4 pagesGyne - Benign LesionsIsabel CastilloNo ratings yet
- PcosDocument5 pagesPcosAinul AzlindaNo ratings yet
- 7418 26240 1 PBDocument7 pages7418 26240 1 PBPattra KeeratibharatNo ratings yet
- Pcos 6Document5 pagesPcos 6MISS. COMNo ratings yet
- The Quality of Life of Women SufferDocument8 pagesThe Quality of Life of Women SufferKritika AgarwalNo ratings yet
- Development of A Health-Related Quality-of-Life Questionnaire (PCOSQ) For Women With Polycystic Ovary Syndrome (PCOS)Document12 pagesDevelopment of A Health-Related Quality-of-Life Questionnaire (PCOSQ) For Women With Polycystic Ovary Syndrome (PCOS)Ke XuNo ratings yet
- Bvaa 131Document10 pagesBvaa 131Sthephany AndreinaNo ratings yet
- Prevalence of Depression Anxiety and QuaDocument8 pagesPrevalence of Depression Anxiety and QuaMISS. COMNo ratings yet
- Polycystic Ovary SyndromeDocument13 pagesPolycystic Ovary SyndromeNAYSHA YANET CHAVEZ RONDINELNo ratings yet
- Psikologi N Emotional InfertilityDocument7 pagesPsikologi N Emotional InfertilityjawaralopangNo ratings yet
- Assessment of Hirsutism Impact On Quality of Life: Association With Severity, Marital Status and PCOSDocument4 pagesAssessment of Hirsutism Impact On Quality of Life: Association With Severity, Marital Status and PCOSInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- The Relationship Between Overactive Bladder and Sexual Activity in WomenDocument11 pagesThe Relationship Between Overactive Bladder and Sexual Activity in WomenJimmy GillNo ratings yet
- Journal Pone 0247486Document13 pagesJournal Pone 0247486MISS. COMNo ratings yet
- Artical PCOSDocument33 pagesArtical PCOSsyedaNo ratings yet
- Study of Prevalence and Risk Factors of Polycystic Ovarian Syndrome Among Adolescent and Young Adults of Rama UniversityDocument8 pagesStudy of Prevalence and Risk Factors of Polycystic Ovarian Syndrome Among Adolescent and Young Adults of Rama UniversityIJAR JOURNALNo ratings yet
- GuidliinesDocument13 pagesGuidliinesFaten NajarNo ratings yet
- Paper 8Document13 pagesPaper 8mansiprajapati2203No ratings yet
- Jurnal 8Document9 pagesJurnal 8Ade Yurga TonaraNo ratings yet
- Nonfar PcosDocument13 pagesNonfar PcosyuniNo ratings yet
- Polycystic Ovary Syndrome and Its Impact On Women's Quality of Life: More Than Just An Endocrine DisorderDocument8 pagesPolycystic Ovary Syndrome and Its Impact On Women's Quality of Life: More Than Just An Endocrine DisorderParthaNo ratings yet
- 06 Chapter 2Document48 pages06 Chapter 2Prakash BalagurunathanNo ratings yet
- Prevalence of Sexual Dysfunctions Among Women With Multiple SclerosisDocument13 pagesPrevalence of Sexual Dysfunctions Among Women With Multiple SclerosisDwi WirastomoNo ratings yet
- Plagrism Copy Last ModfiedDocument41 pagesPlagrism Copy Last ModfiedAfzal MuhammadNo ratings yet
- (PCOSQ) ImpDocument12 pages(PCOSQ) Impamanysalama5976No ratings yet
- Health-Related Quality of Life in Adult MediterranDocument21 pagesHealth-Related Quality of Life in Adult MediterrancxksvhszsvNo ratings yet
- Anxiety in PCOSDocument5 pagesAnxiety in PCOSUsama Bin ZubairNo ratings yet
- Experience of Mental Health in Women With Polycystic Ovary Syndrome A Descriptive Phenomenological StudyDocument11 pagesExperience of Mental Health in Women With Polycystic Ovary Syndrome A Descriptive Phenomenological StudyMelany AntounNo ratings yet
- ReviewDocument13 pagesReviewNelly ElizabethNo ratings yet
- Your Partner in Quality Education: Abada College College DepartmentDocument3 pagesYour Partner in Quality Education: Abada College College DepartmentMaye MadriNo ratings yet
- Infertility and Sexual Dysfunctions: A Systematic Literature ReviewDocument8 pagesInfertility and Sexual Dysfunctions: A Systematic Literature ReviewTantonio Tri PutraNo ratings yet
- Ijrm 13 061Document10 pagesIjrm 13 061R. WadlowNo ratings yet
- Ijrb 18 243Document10 pagesIjrb 18 243HappyLearnNo ratings yet
- Impact of Polycystic Ovary, Metabolic Syndrome and Obesity on Women Health: Volume 8: Frontiers in Gynecological EndocrinologyFrom EverandImpact of Polycystic Ovary, Metabolic Syndrome and Obesity on Women Health: Volume 8: Frontiers in Gynecological EndocrinologyNo ratings yet
- Functional Hypothalamic Amenorrhea and Its Psychological Correlates: A Controlled ComparisonDocument14 pagesFunctional Hypothalamic Amenorrhea and Its Psychological Correlates: A Controlled ComparisonLiaNo ratings yet
- Pcos Ob JournalDocument10 pagesPcos Ob JournalSean SialanaNo ratings yet
- Evaluation of Some Immunological Aspects of Women With Polycystic Ovary Syndrome in Wasit GovernorateDocument8 pagesEvaluation of Some Immunological Aspects of Women With Polycystic Ovary Syndrome in Wasit GovernorateCentral Asian StudiesNo ratings yet
- Development and Validation of Turkish Version of The Female SexualDocument8 pagesDevelopment and Validation of Turkish Version of The Female SexualceydaalyazhotamisNo ratings yet
- 2021 - Disfunção Sexual em Mulheres Com CADocument12 pages2021 - Disfunção Sexual em Mulheres Com CAHeriksonNo ratings yet
- Gender Differences in Health Related Quality of Life Measured by The Sarcoidosis Health QuestionnaireDocument7 pagesGender Differences in Health Related Quality of Life Measured by The Sarcoidosis Health Questionnairemuralim_phy1986No ratings yet
- DHEA and Polycystic Ovarian Syndrome Meta-Analysis of Case-Control StudiesDocument13 pagesDHEA and Polycystic Ovarian Syndrome Meta-Analysis of Case-Control StudiesMyriam CardenasNo ratings yet
- Tsarna - 2022 - Sistematic Review - Psychological Sexual and QoL ImpactsDocument24 pagesTsarna - 2022 - Sistematic Review - Psychological Sexual and QoL ImpactsLídia SilveiraNo ratings yet
- Systematic Review On Recognising Patterns in Incidence of Polycystic Ovarian Syndrome in Young WomenDocument4 pagesSystematic Review On Recognising Patterns in Incidence of Polycystic Ovarian Syndrome in Young WomenInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Menopouse 26 45 PDFDocument21 pagesMenopouse 26 45 PDFevilasusantiNo ratings yet
- Original Research-EndocrinologyDocument10 pagesOriginal Research-EndocrinologyScott LoveNo ratings yet
- Deu 342Document7 pagesDeu 342Javed AslamNo ratings yet
- 404 2017 Article 4623 PDFDocument9 pages404 2017 Article 4623 PDFMariam QaisNo ratings yet
- Ijwh 10 397Document12 pagesIjwh 10 397Jonida LeliNo ratings yet
- Ovario PoliqDocument16 pagesOvario PoliqlizethNo ratings yet
- Polikistik Pada RemajaDocument9 pagesPolikistik Pada Remajakinanti wulanNo ratings yet
- Pcos 4Document8 pagesPcos 4MISS. COMNo ratings yet
- Tayeb I 2017Document8 pagesTayeb I 2017Essay NationNo ratings yet
- Etiology and Risk Factors of Female Infertility in Pravara Rural Hospital, LoniDocument9 pagesEtiology and Risk Factors of Female Infertility in Pravara Rural Hospital, LoniIJAR JOURNALNo ratings yet
- Polycystic Ovary Syndrome and Its Impact On Women S Quality of Life More Than Just An Endocrine DisorderDocument9 pagesPolycystic Ovary Syndrome and Its Impact On Women S Quality of Life More Than Just An Endocrine DisorderShahzad Jawaid KhanNo ratings yet
- Polycystic Ovarian Syndrome PcosDocument15 pagesPolycystic Ovarian Syndrome Pcosapi-341766332No ratings yet
- Revisi MRKH - ParaphraseDocument4 pagesRevisi MRKH - Paraphrasestephie_aninditaNo ratings yet
- Pre-Existing Mental Health Disorders Affect Pregnancy and Neonatal Outcomes: A Retrospective Cohort StudyDocument7 pagesPre-Existing Mental Health Disorders Affect Pregnancy and Neonatal Outcomes: A Retrospective Cohort StudyRaden Ayu Miftah CahyaniNo ratings yet
- McGrath, 2017Document16 pagesMcGrath, 2017Zeynep ÖzmeydanNo ratings yet
- 1 s2.0 S0015028211027075 MainDocument8 pages1 s2.0 S0015028211027075 MainHanine El-DekmakNo ratings yet
- Criterios y Fenotipos Del PCOSDocument10 pagesCriterios y Fenotipos Del PCOSGeos KarNo ratings yet
- AydinDocument6 pagesAydinDedi SaputraNo ratings yet
- Strategies and Methods To Study Female-Specific CV Health and Disease-Guide For Clinical-Ouyang Et Al 2016Document24 pagesStrategies and Methods To Study Female-Specific CV Health and Disease-Guide For Clinical-Ouyang Et Al 2016Bumbum AtaunNo ratings yet
- Saliva Test Report: Your Results at A GlanceDocument7 pagesSaliva Test Report: Your Results at A GlanceKaveh EshkoftiNo ratings yet
- Midterms - Maternal and Child Health NursingDocument40 pagesMidterms - Maternal and Child Health NursingMrz AlzNo ratings yet
- Case Study Preterm LaborDocument6 pagesCase Study Preterm LaborAdriane ComaNo ratings yet
- Articulo 4Document6 pagesArticulo 4Eduardo GarcíaNo ratings yet
- Impotency, Sterility & Artificial InseminationDocument51 pagesImpotency, Sterility & Artificial Inseminationdrmansur56No ratings yet
- Immature Schistosoma ReflexDocument2 pagesImmature Schistosoma Reflexpramod kumarNo ratings yet
- Kanker Payudara: Dr. Dian Andriani, SPKK, M.Biomed, MarsDocument31 pagesKanker Payudara: Dr. Dian Andriani, SPKK, M.Biomed, Marsdian andriani ratna dewiNo ratings yet
- 10.appendix - Visuals FinalDocument15 pages10.appendix - Visuals FinalJosie MercyNo ratings yet
- Menstrual Hygiene Management - EnglishDocument16 pagesMenstrual Hygiene Management - EnglishGunnenthriftNo ratings yet
- ObstetricsDocument7 pagesObstetricsArleneDelosSantos100% (1)
- Anatomy and Physiology CorrectedDocument15 pagesAnatomy and Physiology CorrectedSANCHAYEETANo ratings yet
- Detailed Study On Infertility Its Causes and TreatmentDocument2 pagesDetailed Study On Infertility Its Causes and TreatmentBibhuti bhusan MondalNo ratings yet
- International Institute of Reproduction and Fertility TrainingDocument6 pagesInternational Institute of Reproduction and Fertility Trainingapi-294745900No ratings yet
- Cervical Erosion/ Cervical EctopyDocument12 pagesCervical Erosion/ Cervical EctopyPrajwal KpNo ratings yet
- Dism-PMSDocument29 pagesDism-PMSAg NesNo ratings yet
- MenstruationDocument33 pagesMenstruationmskot100% (3)
- IUD Aftercare InstructionsDocument2 pagesIUD Aftercare Instructionswhiterose08No ratings yet
- Ehs Hospitals All StatesDocument85 pagesEhs Hospitals All Statesnaiduu497No ratings yet
- Name of The Drug Mechani SM of Action Dosage Indicatio NS Contraindica Tions Adverse Reaction Nursing ResponsibilitiesDocument2 pagesName of The Drug Mechani SM of Action Dosage Indicatio NS Contraindica Tions Adverse Reaction Nursing Responsibilitieshey aadarshaNo ratings yet
- Labor and DeliveryDocument4 pagesLabor and DeliveryJinky Teneza100% (1)
- CH 19Document5 pagesCH 19Ryan Carlo IbayanNo ratings yet
- Acuan Tarif Jasa MedikDocument8 pagesAcuan Tarif Jasa MedikhikmahNo ratings yet
- Essential Procedures in Normal PregnancyDocument4 pagesEssential Procedures in Normal PregnancyRuffa Mae CalimagNo ratings yet
- SimsDocument4 pagesSimsMariel AbatayoNo ratings yet
- OB SHIFTING EXAM Feb2019Document10 pagesOB SHIFTING EXAM Feb2019christinejoanNo ratings yet
- Anniversary Gift List 2024Document7 pagesAnniversary Gift List 2024Nishad NPNo ratings yet
- Abortion Law Shodhganga 8Document42 pagesAbortion Law Shodhganga 8Ritesh kumarNo ratings yet
- Doh MCNDocument14 pagesDoh MCNCbrc CebuNo ratings yet