Volume 8, Issue 11, November – 2023 International Journal of Innovative Science and Research Technology
ISSN No:-2456-2165
Predictors of Unfavorable Treatment Outcome
Among Childhood Tuberculosis Patients in Ede Town
Health Centers, Sub-District of Osun, Nigeria
1 2
Ayodeji Oluwaseun Faremi Olanrewaju Sunday
Public Health Laboratory/TB Laboratory, State Hospital, Department of Community Medicine, Osun State
Ede, Osun State University, Osun State
3 4
Akinwale John Faniyi Ayoade Babatunde Olanrewaju
ORCID No: 0000-0003-1243-2751 Public Health Laboratory/TB Laboratory, State Hospital,
Sure Health Laboratory and Diagnostic Limited, Ede, Osun state
Asokoro, Abuja
5 6
Babatunde Joseph Abioye Temitope Daniel Adeleke,
Shepherd for Health Environment and Advocay and State Hospital, Ogbomosho
Development Centre, Ikire, Osunstate
7 8
Olawale Sunday Animasaun Ogunjimi Temitope,
ORCID No: 0000-0002-5203-6174 University College Hospital, Ibadan
Nigeria Field Epidemiology and Laboratory Training
Programme, NCDC, Abuja
9 10
Tolulope Adaran Abeeb Babatunde Jamiu
ORCID No: 0000-0001-6590-5474 Federal Medical Center, Markurdi, Benue State
Grant Management Unit, Lagos State Ministry of Health
11 12
Oladeji Moroof Gbadamosi Oluwafemi Odola
Osun-State Tuberculosis Leprosy Control Program Manager Institute of Human Virology, Osun-State , Nigeria
(STBLCP)
13 14
Maroof Adebayo Alatise, Adedayo Adeyemi,
Deputy Program Manager, State Tuberculosis and Leprosy Center for Infectious Disease Research and Evaluation,
Control Program, Osun-State, Nigeria Lafia, Nasarawa State, Nigeria
IJISRT23NOV2075 www.ijisrt.com 2476
Volume 8, Issue 11, November – 2023 International Journal of Innovative Science and Research Technology
ISSN No:-2456-2165
Abstract:- side effects, developmental changes, and inconsistent
routines contribute to these outcomes.
Background:
Tuberculosis in children is a consequence of adult Recommendation:
TB, but it's often neglected. Understanding treatment To improve drug adherence in children, healthcare
outcomes in children is crucial for designing effective providers, parents, and children should improve
interventions. education, communication, and technology use.
Collaboration between professionals, researchers, and
Aim: policymakers is essential for identifying barriers and
This study is aimed at evaluating some predicting implementing evidence-based strategies.
factors associated with and responsible for successful
and unsuccessful treatment in the Ede town health Keywords:- Childhood Tuberculosis, HIV Co-Infection,
centers of the sub-district of Osun State, Nigeria. Extra-Pulmonary Tuberculosis.
Methods: I. INTRODUCTION
This retrospective study involved analyzing
statistically reviewed TB records of patients aged 0–14 Tuberculosis is the 13th leading cause of death1 with
years that were reported and enrolled between April the causative agent called Mycobacterium tuberculosis. It is
2018 and July 2021 at selected health facilities in Ede the second leading infectious killer disease until the
town, including the laboratory Gene Xpert site. outbreak of COVID-19 and ranked above Human Immune
Deficiency Virus and Acquired Immune Deficiency Virus
Results: (HIV/AIDs).2 Tuberculosis is transmitted when an infected
Of the 102 enrollees, 24/102 were aged 0–4 years, person expels the bacteria (Mycobacterium tuberculosis) by
with the mortality ratio (MR) being 0.35% (95% CI coughing and another person inhaling the droplet. Primarily
0.17–0.56), and 45/102 [MR]:0.26% (95% CI 0.13-0.36) it affects the lungs (pulmonary tuberculosis) but can be
were aged 5–9 years. 33/102 [(MR): 0.46% (95% CI transmitted to other sites of the body. In this case it is
0.21-0.76)] were aged 10–14 years. 52/102 (51%) had a referred to as extra-pulmonary tuberculosis (EPTB).
household contact, while 45% represented other contacts.
One-quarter of our total respondents were co-infected In 2020 according to WHO, an estimate of 10 million
with HIV, while 75.5% had extra- people were victims of tuberculosis infection globally, of
pulmonary tuberculosis. The treatment failure rate which 5.6 million are men, 3.3 million are women and 1.1
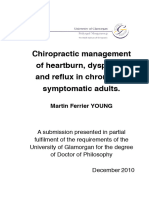
decreased with increasing age, with 0–4 years having the million are children1,3 and is presented in all countries and
worst treatment failure rate at 50% and 10–14 age groups1. Annual TB cases in Nigeria are predicted to
years having the highest treatment success rate at 60.6% reach 460,000 2. Due to the growing correlation between TB
compared to the remaining age group. Respondents with and HIV/AIDS, the prevalence of TB among patients with
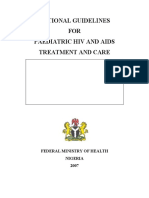
good drug adherence status had 100% treatment success, HIV/AIDS rose from 10.5 to 40%3. The incidence and
which was statistically significant (p value < 0.01). mortality rates of tuberculosis in the nation are 219/100,000
and 39/100,000, respectively, with a 24% treatment
Conclusion: coverage percentage in 2016, the nation has the lowest
The study found that drug adherence status in global TB treatment coverage rate2. With a drug resistance
children aged 0–14 in Ede Health Centers, Osun, Nigeria, TB frequency of 4.3% among new cases and 25% among
is a major predictor of unsuccessful tuberculosis those who have already received treatment, Nigeria is
treatments. Factors such as difficulty understanding ranked eighth among the 30 nations with the highest burden
instructions, parental supervision, taste, formulation, of multi drug-resistant tuberculosis (MDR-TB).
IJISRT23NOV2075 www.ijisrt.com 2477
Volume 8, Issue 11, November – 2023 International Journal of Innovative Science and Research Technology
ISSN No:-2456-2165
Historically, childhood TB has been given low priority children. The Xpert MTB/RIF as mentioned earlier is an
in most national programme because it contributes little to automated cartridge-based nucleic acid amplification test
6,7,8
disease transmission . While about 1.1 million children (NAAT) for simultaneous rapid tuberculosis diagnosis and
are diagnosed with tuberculosis globally in 2020, mostly in rapid antibiotic sensitivity test.
low and middle income countries, children as a vulnerable
population are frequently left out of randomized trials of The stool Xpert test hold a positive promise as an
9
novel treatments . alternative to sputum Xpert testing since stool collection is
easier and relatively safer compared to sputum collection in
As one of the top 10 causes of death, childhood TB is a children.
silent killer, with risk of mortality being particularly high in
children aged <5years and HIV co-infected children not One recurring challenge that still persists in health data
10,11
receiving Antiretroviral therapy (ART) among this vulnerable group is Multi-Drug Resistant
Tuberculosis (MDR-TB), as this was attributed to health
Difficulties in making a tuberculosis diagnosis provider not paying detailed attention to this age group 1.
(particularly the absence of microbiological confirmation), a Management of childhood and adolescent TB is still a
protracted course of treatment, lack of simple access to pressing challenge even in low incidence countries6,12.
fixed-dose palatable pediatric formulations, the burden of
pill-taking, and drug side effects are significant obstacle in To achieve comprehensive and excellent treatment
treating children 9. outcomes in children, it is therefore essential to scale up
more flexible diagnostic techniques, and a more pediatric
Pai et al., 2022 reveal that the majority of pediatric friendly fixed-dose formulations to overcome difficulties in
cases start out as mild illnesses with little bacillary burden diagnosis and treatment as well.
on smear and molecular tests. It was suggested in his report Hence, This study aimed to evaluate some predicting
that it is likely unnecessary to utilize microscopy to rule out factors associated and responsible for unsuccessful
situation where a smear is tested positive. A surrogate for treatment of childhood tuberculosis in Ede town Health
smear-negative tuberculosis in a way to simultaneously rule- Centers, Osun subdistrict, Osun state, Nigeria.
out rifampicin resistance low, very-low or trace positive
readings is by GeneXpert test which has also been micro- Aim:
biologically proven9. Bearing in mind at this juncture that in This study is aimed at determining the associated
TB treatment cascade, children constitute the “missing face” factors responsible for unsuccessful treatment of childhood
of TB due to diagnostic dilemma. The use of sputum as a tuberculosis in Ede town Health Centers Osun subdistrict,
biological specimen for pediatric TB diagnosis in past Osun state, Nigeria.
constitute a dilemma in specificity, sensitivity and accuracy
in the result produced. Sputum is difficult to obtain Objectives:
especially those of aged <5years and are unable to
effectively expectorate requiring laryngopharyngeal To determine the baseline clinical and laboratory status
aspiration followed by sputum induction. of tuberculosis in children
To access treatment outcomes (favorable-completed
The process of gastric aspirations, sputum induction treatment and unfavorable treatment)
and nasal/bronchial lavage are technical, painful and To determine the association between baseline clinical
invasive and very difficult to implement in resource- and laboratory on treatment outcome
constrained settings. With a multisectoral concerted efforts, To access predictors of unfavorable outcome using
the WHO endorsed and recommends innovative solutions appropriate statistical test
with the use of Xpert MTB/RIF and Xpert Ultra (where
available) to detect MTB DNA and Rif resistance in stool of
IJISRT23NOV2075 www.ijisrt.com 2478
Volume 8, Issue 11, November – 2023 International Journal of Innovative Science and Research Technology
ISSN No:-2456-2165
II. MATERIALS AND METHODS Ethambutol (E) followed by R and H for 10 months
(2RHZ+E/4RH)
This was a retrospective study. The extraction of data
was done using pro-formal that was designed to extract Treatment outcomes were categorized as successful
information from the case history of children treated for (treatment completed and cured) and unsuccessful
tuberculosis in the Chest clinic, Paediatric ward at the health (treatment failure, died, loss to followup, not evaluated)
centers over a period of 35 months, from April 2018 to based on National tuberculosis program guideline adopted
March 2021. Variable extracted from the archive included from World Health Organization depending on outcome of
the patients' age, gender, history of BCG vaccination, laboratory investigations at regular intervals 2nd , 5th and 6th
history of contact, classification based on anatomical site month for those under regimen 1 or 2nd and 10th month for
into pulmonary and extra-pulmonary, chest radiograph those under regimen 2 during course of treatment.
findings, GeneXpert results, HIV test results including CD4
values, drug adherence, and treatment outcome15 These include respondents age, sex, nutritional status,
method of diagnosis (clinical or Radiological), HIV status
In terms of diagnosis, children that are symptomatic (Positive or Negative) and Anatomical site ( Pulmonary or
have sputum collected for geneXpert or acid-fast bacilli Extra-pulmonary).
microscopy while those who could not produce sputum had
other samples such as gastric lavage, stool, examined also Data Collection
using Xpert. These according to National Program are Data collected using a Pro formal from the case note
classified as bacteriological while those diagnosed mainly were checked for errors before entry and analyzed using
based on clinical findings or radiological investigations Statistical Product for service solution version 23.
14
according to decision are classified as clinical Regarding study population, descriptive statistics (mean and
standard deviation) were calculated for continuous variables
Concerning classification, Pulmonary tuberculosis while categorical variables were presented as frequency and
cases was defined as symptomatic child with: (1) percentages in a tabular form. Chi-square test or Fisher's
bacteriologically confirmed tuberculosis using sputum AFB, exact test was used to test for association between
(2) Sputum with MTB detected using GeneXpert, (3) demographic, clinical characteristics with treatment
radiologically confirmed tuberculosis, or (4) Probable outcome (Successful and treatment failure). A p-value of
tuberculosis. Probable tuberculosis was said to be a TB <0.05 was taken as statistically significant. Multivariate
score >7, radiologic certainty and a good clinical response to analysis was done to assess predictors of unsuccessful
anti-tuberculosis treatment in the absence of bacteriologic treatment outcome.
confirmation. Radiologically confirmed pulmonary
tuberculosis was defined as an agreement between two Ethical Clearance
independent radiologists that the Chest X-ray indicated Ethical clearance for the conduct of the study was
certain tuberculosis and a TB score 1-6 in the absence of obtained from the Ethical clearance review committee, Osun
bacteriologic confirmation and a good clinical response to State University, Osogbo. The addresses, names, hospital
13
anti-tuberculosis treatment number and other identifiers of the patients were omitted in
order to maintain confidentiality.
Standard treatment regimen under National program
consist of 2 regimen namely Regimen 1 and Regimen 2. III. RESULT
Regimen 1 has 2 months of Isoniazid (H), Rifampicin (R),
Pyrazinamide (Z), Ethambutol (E) followed by R and H for Out of the 102 pediatric tuberculosis cases reported,
4months (2RHZ+E/4RH) while Regimen 2 has 2 months of Children in the range of 5-9 years have the highest
Isoniazid (H), Rifampicin (R), Pyrazinamide (Z), proportion (44.1) and 0-4 years have the lowest proportion
(23.5). The ratio of males to females was 1:1. When we
IJISRT23NOV2075 www.ijisrt.com 2479
Volume 8, Issue 11, November – 2023 International Journal of Innovative Science and Research Technology
ISSN No:-2456-2165
compared the nutrition, two third of the children reported than households had a significant treatment success rate
being malnourished, and one-third were not malnourished. (82%). Patients identified with the Bacille Calmette Guerin
Also, when the history of the patients was tracked, there was (BCG) vaccination history and those not exhibited higher
no difference between the percentage of those with treatment success than failure (52.1%, 59.3%, and 47.9%,
household contact and those whose connection was from 40.7%). However, there was no statistically significant in
other sources. Nearly three-quarters of our respondents were their comparison.
HIV-negative, and one-quarter were co-infected with HIV.
From the classification of tuberculosis, 24.5% were Table 3 shows that successful treatment outcome
pulmonary tuberculosis, while 75.5% were extrapulmonary among patients that adequately adheres to their prescription
tuberculosis. The respondents were checked for the history (Good adherence status) was more than patients who poorly
of the Bacille Calmette Guerin vaccine (BCG) vaccine. The adhere to their drug prescription (Poor adherence status).
ratio of those that took BCG and those that did not was 1:1. The difference is statistically significant with p value < 0.01.
The methods for diagnosis captured in this study are clinical Hence, the drug adherence status of respondents is a
and bacteriological, with 40.2% and 59.8%, respectively. significant predictor of successful treatment outcomes
among respondents.
The treatment failure rate decreased with increasing
age, with 0-4 years having 50% with the worst treatment IV. DISCUSSION
failure rate, 5-9 years at 44.4%, and 10-14 years at 39.4%.
On the contrary, the treatment success rate increased with A call for emergency response to protect children from
age, with 0-4 years having 50%, 5-9 years having 55.6%, TB and preventable deaths from this disease brings to the
and 10-14 years, with 60.6% being the age group with the rising attention being paid to the global epidemic of
highest treatment success rate compared to the remaining childhood TB17 . This study described the case distribution
age group. of childhood TB and predictors to successful and
unsuccessful treatment outcomes in Ede Town Health
There was no statistically significant difference Centres located in the South Western part of Nigeria, and
between the male and the female success and failure rates of assessed the relationship between demographic and clinical
the treatment. Patients who are HIV positive have more status with treatment outcomes.
success rate than patients with HIV negative, and the
difference between the two was slightly significant. The Age range, nutritional status, HIV status, drug
treatment success rate of malnourished patients was higher adherence status, history of contact has a strong interplay
than usual, with 61.2% and 45.7%, respectively. Normally with treatment outcomes. Though the WHO estimated the
nourished patients were seen with more failure in their TB prevalence rate19 infected children are at higher risk of
treatment, while malnourished patients have high treatment developing active TB when exposed to adults with smear-
success rates which are both significant in their differences. positive TB20.
Those who adhere to their drugs achieve 100% success in
the treatment, while an insignificant proportion of success This study however provides valuable insights into the
rate (4.3) was recorded from patients with poor adherence. underlying challenges of childhood TB management in
Pulmonary tuberculosis patients responded well (60%) to high-burden, resource-limited settings.
treatment compared to extra-pulmonary tuberculosis
patients, and there was no significant difference in their Children under the age of five represented the majority
failure in response to treatment. of childhood TB cases in earlier studies conducted in
Africa32,33, and young children had the highest risk of
Furthermore, patients with a history of household developing active TB, particularly those under the age of
contact reacted at the same rate to treatment success and two years 31. However, in our study, older children with age
failure (50%,50%). In contrast, those with connections other range (5 - 9 years) represented the highest distribution of the
IJISRT23NOV2075 www.ijisrt.com 2480
Volume 8, Issue 11, November – 2023 International Journal of Innovative Science and Research Technology
ISSN No:-2456-2165
age group and about 44.1%. The increase in TB disease in treatment outcome but showed no statistical significant. As
adolescence is linked to the increased independence, stated by Sinha et al., (2018), the WHO has stressed that all
18
mobility and risk taking behaviour in this age group . patients with active TB should receive individualized
nutritional assessment and management, including dietary
The treatment failure rate decreased with increasing counseling and nutritional interventions, to prevent
age group, with 0 - 4 years having the worst treatment treatment failure.
failure rate, while treatment failure rate increased with age,
with 10 - 14 years having the best treatment success rate. Nutritional status and anti-TB drug exposure should
This is primarily due to dependence on guidance or care- both be assessed and monitored over time, as both
giver after drug prescription which then facilitate drug nutritional status and pharmacokinetics change29. In
adherence at age group (5 - 9) years18 addition, there is more to be done on the drug adherence
status of other TB patients to ensure there is low risk of
Also, in this study, no significant gender difference transmission. This can be achieved by therapeutic drug
between children with extra-pulmonary and pulmonary TB monitoring (TDM)30, combined with drug susceptibility
was observed. Previous study by Oloyede et al., had shown testing, to improve outcomes and reduce drug toxicity by
conformance with the above that there is no significant tailoring treatment27. Exploration of a TDM program for
gender difference between children with extra-pulmonary malnourished TB patients may be helpful to assess the
and pulmonary TB in 2019 as published in World Journal of relationship between malnutrition and bioavailability of TB
Biomedical Research. drugs.
This study showed that TB patients who are co- BCG vaccination significantly reduced the progression
infected with HIV recorded more success in their treatment to severe TB among children with active TB24. Studies have
outcomes, that is patients who are HIV positive have more concluded that BCG is a cost-effective intervention against
success rate than patients with HIV negative, and the severe childhood TB, one that is only slightly less cost-
difference between the two was slightly significant. A joint effective than the treatment of active disease with short-
combinational efforts and an integration in treatment care course chemotherapy, especially in southeast Asia, Africa,
cascade with strong monitoring evaluation of the individual and the western Pacific region where TB infection rates are
in TB/HIV clinic activities and a biased keen interest in the high25. Thus, BCG vaccination of high-risk populations can
desired end results could be responsible for this. potentially contribute to the vision of “zero tuberculosis”
deaths in children. This study showed no significant
In addition, there is no statistical significance in the difference on the history of BCG vaccination in treatment
correlation of age and sex with the TB treatment outcome outcomes, and thus could be attributed to lack of knowledge
and this could be as result of low volume of data recorded about BCG vaccination record by the patient mother or care
for statistical presentations. Though, study by Chaves- giver.
Torres et al., 2021 and some others had indicates that these
factors are associated with unfavorable TB treatment It was previously stated scaling up more flexible
outcomes. diagnostic techniques that accommodate a pediatric friendly
fixed-dose in diagnosis and treatments are essential for
Malnutrition can detrimentally affect the treatment of successful treatment outcomes.
TB, but there is more to explore regarding the complex
interactions between malnutrition and TB. Patients with TB Though method of diagnosis had no or little impact in
may suffer from malabsorption because of malnutrition treatment outcomes and the overall objectives unlike in
and/or comorbidities such as diabetes and human other similar studies. In Nigeria the diagnosis of TB in
22
immunodeficiency virus/AIDS . This study revealed a children is done using the TB score chat and TB score
higher percentage of malnourished TB patients affecting the algorithm which is based on clinical findings, family history
IJISRT23NOV2075 www.ijisrt.com 2481
Volume 8, Issue 11, November – 2023 International Journal of Innovative Science and Research Technology
ISSN No:-2456-2165
of contact with a smear -positive case, x-ray examination, [3]. Awoyemi OB, Ige, OM, Onadeko, BO. Prevalence
tuberculin skin test (TST), molecular techniques of active tuberculosis in Human Immunodeficiency
29
(GeneXpert), TB Quantiferon and culture Virus Seropositive Adult Patients in University
College Hospital, Ibadan, Nigeria. African Journal of
V. CONCLUSION Medical Science. 2019; 31:329-32
[4]. Tamuzi, JL, Ayele BT, Shumba CS, Adetokunboh
This study assessed the factors responsible for OO, Uwimana-Nicol J, Haile ZT, Inugu J, Nyasulu
unsuccessful tuberculosis treatments in children (0 - 14 PS. Implications of COVID-19 in high burden
years) in Ede Health Centers, Osun sub-district, osun state, countries for HIV/TB. A systematic review of
Nigeria, and it was determined that drug adherence status of evidence. BMC Infectious Diseases, 2020; 20 (1).
the respondents showed a major predictor to unsuccessful [5]. Macneil A, Glaziou P, Sismanidis C, Date A,
treatment outcomes. This was primarily due to difficulty of Maloney S, Floyd K. Global Epidemiology of
children of this age group understanding and following Tuberculosis and Progress Toward Meeting Global
medication instructions, rely on parental supervision and Targets — Worldwide, 2018. MMWR. Morbidity and
support for medication administration, face challenges with Mortality Weekly Report, 2020; 69 (11), 281–285.
the taste and formulation of medications, experience side [6]. Gafar F, Arifin H, Jurnalis YD, Yani FF, Fitria N,
effects and discomfort, struggle with developmental changes Alffenaar J-WC, Wilffert B. Antituberculosis Drug-
in medication needs, and inconsistency routines that makes induced Liver Injury in Children. Pediatric Infectious
it harder to adhere to prescribed drug regimes. Disease Journal, 2019; 38 (1), 50–53.
[7]. Snow KJ, Sismanidis C, Denholm J, Susan, Graham
RECOMMENDATION SM. The incidence of tuberculosis among
adolescents and young adults: a global estimate.
To enhance drug adherence in children, it is European Respiratory Journal. 2018; 51 (2),
recommended to improve education and communication 1702352.
between healthcare providers, parents, and children. This [8]. García-Basteiro AL, DiNardo A, Saavedra B, Silva
can be achieved by providing clear and simplified DR, Palmero D, Gegia M, Migliori GB, Duarte R,
instructions for medication administration to parents and Mambuque E, Centis R, Cuevas LE, Izco S, Theron
developing child-friendly educational resources. G. Point of Care Diagnosis in Tuberculosis.
Additionally, technology could play a role by incorporating Pulmonology.2018 ; 24(2); 73-85
applications and reminder systems to help parents and [9]. Pai M. Zar HJ, Childhood Tuberculosis — Time for
children remember medication schedules. Collaboration Shorter and Differentiated Treatment. New England
between healthcare professionals, researchers, and Journal of Medicine, 2022; 386 (10), 988–989.
policymakers is also crucial to identifying and addressing [10]. Dodd PJ, Yuen CM, Sismanidis C, Seddon JA,
barriers to drug adherence, as well as implementing Jenkins HE. The global burden of tuberculosis
evidence-based strategies to improve health outcomes. mortality in children: a mathematical modelling
study. The Lancet Global Health, 2017; 5 (9), e898–
REFERENCES e906.
[11]. Jenkins HE, Tolman AW, Yuen CM, Parr JB,
[1]. WHO 2020, World Malaria Reports, launched in Keshavjee S, Perez-Velez CM, Pagano M, Becerra
th
Washington DC, 11 December 2020. MC, Cohen T. 2014. Incidence of multidrug-resistant
[2]. Federal Ministry of Health Nigeria (FMoH). National tuberculosis disease in children: Systematic review
Tuberculosis Catastrophic Cost Survey: Report of the and global estimates. Lancet 383: 1572–1579
National Survey to Determine the Proportion of TB
Patients and their Households Experiencing
Catastrophic Cost due to TB. 2017
IJISRT23NOV2075 www.ijisrt.com 2482
Volume 8, Issue 11, November – 2023 International Journal of Innovative Science and Research Technology
ISSN No:-2456-2165
[12]. Gröschel MI, Van Den Boom M, Migliori GB, Dara [21]. Oloyede IP, Johnson OE, David U, Edem B. Pattern
M. Prioritising children and adolescents in the of Diagnosis and Treatment of Childhood
tuberculosis response of the WHO European Region. Tuberculosis in a Teaching Hospital in Southern
European Respiratory Review, 2019; 28 (151), Nigeria. W J Biomed Res 2019, Vol. 6 No. 1, p. 29 –
180106. 38.
[13]. Cold Spring Harb Perspect Med 2014;4:a017855 [22]. Beek TL., Jan-Willem C Alffenaar, Mathieu S
[14]. Lange C, Chesov D, Heyckendorf J, Leung CC, Bolhuis, Tjip S van der Werf, Onno W Akkerman .
Udwadia Z, Dheda K, Drug-resistant tuberculosis: Tuberculosis-Related Malnutrition: Public Health
An update on disease burden, diagnosis and Implications . The Journal of Infectious Diseases,
treatment. Respirology, 2018; 23 (7), 656–673. Volume 220, Issue 2, 15 July 2019, Pages 340–341
[15]. Graham S.M, Ahmed T, Amanullah F, Browning R, [23]. Sinha P, Davis J, Saag L, Undernutrition and
Cardenas V, Casenghi M. "Evaluation of tuberculosis: public health implications [manuscript
tuberculosis diagnostics in children: Proposed published online ahead of print 22 November 2018].
clinical case definitions for classification of J Infect Dis 2018. doi:10.1093/infdis/jiy675
intrathoracic tuberculosis disease. Consensus from an [24]. Liao Q, Zheng Y, Wang Y, Ye L, Liu X, Jiao W.
expert panel". Journal of Infectious Diseases.2019; Effectiveness of Bacillus Calmette-Guérin
205:S199-208. vaccination against severe childhood tuberculosis in
[16]. Federal Ministry of Health. National Strategic Plan China: a case-based, multicenter retrospective study.
for Tuberculosis 2015–2020, Nigeria. Abuja, International Journal of Infectious Diseases. (2022).
Nigeria: Federal Ministry of Health; 2015. Volume 121, August 2022, Pages 113-119
[17]. Jenkins HE, Yuen CM, Rodriguez CA, [25]. Trunz BB, Fine P, Dye C. Effect of BCG
Nathavitharana RR, McLaughlin MM, Donald P, et vaccination on childhood tuberculous meningitis and
al. Mortality in children diagnosed with tuberculosis: miliary tuberculosis worldwide: a metaanalysis and
a systematic review and meta-analysis. Lancet Infect assessment of cost-effectiveness. Lancet, 367 (2006),
Dis. 2017;17:285–295. doi: 10.1016/S1473- pp. 1173-118
3099(16)30474-1. [26]. Alao M, Maroushek S, Chan Y, Asinobi A,
[18]. Ahmed P, Ulonnam C. Clinical presentation of Slusher T, Gbadero D, Treatment outcomes of
tuberculosis in adolescents as seen at National Nigerian patients with tuberculosis: A retrospective
Hospital Abuja, Nigeria. Nig J Paediatr. 25-year review in a regional medical center. PLoS
2014;41:331-6 One. 2020; 15(10): e0239225. Published online 2020
[19]. World Health Organization. Global tuberculosis Oct 29. doi: 10.1371/journal.pone.0239225 PMCID:
report, 2014. Geneva, Switzerland:WHO;2014. PMC7595370 PMID: 33119601
WHO/HTM/TB/2014.08.http://apps.who.int/iris/bitst [27]. Ghimire S, Bolhuis MS, Sturkenboom MG (2016).
ream/10665/137094/1/9789241564809_eng.pdf?ua= Incorporating therapeutic drug monitoring into the
1 Accessed July 2015. World Health Organization hierarchy of tuberculosis
[20]. Chaves-Torres NM, Fadul S, Patiño J, Netto E diagnostics. Eur Respir J 2016; 47: 1867 – 9.
Factors associated with unfavorable treatment [28]. Beek TL, Jan-Willem C Alffenaar, Mathieu S
outcomes in patients with rifampicin-resistant Bolhuis, Tjip S van der Werf, Onno W Akkerman .
tuberculosis in Colombia 2013–2015: A retrospective Tuberculosis-Related Malnutrition: Public Health
cohort study. PLoS ONE, (2021) 16(4): e0249565. Implications. The Journal of Infectious Diseases,
https://doi.org/10.1371/journal.pone.0249565. Volume 220, Issue 2, 15 July 2019, Pages 340–341
IJISRT23NOV2075 www.ijisrt.com 2483
Volume 8, Issue 11, November – 2023 International Journal of Innovative Science and Research Technology
ISSN No:-2456-2165
[29]. Oloyede IP, Johnson OE, David U, Edem B. Pattern [32]. Newton SM, Brent AJ, MRCP, Anderson S,
of Diagnosis and Treatment of Childhood Whittaker E, Kampmann B: Paediatric tuberculosis.
Tuberculosis in a Teaching Hospital in Southern Lancet Infect Dis 2008, 8(8):498–510.
Nigeria. W J Biomed Res 2019, Vol. 6 No. 1, p. 29 – [33]. Harries AD, Hargreaves NJ, Graham SM,
38. Mwansambo C, Kazembe P, Broadhead RL, Maher
[30]. Warmelink I, Ten Hacken NH, Van Der Werf TS, D, Salaniponi FM: Childhood tuberculosis in
Van Altena R. Weight loss during tuberculosis Malawi: Nationwide case-finding and treatment
treatment is an important risk factor for drug-induced outcomes. Int J Tuberc Lung Dis 2002, 6(5):424–
hepatotoxicity. British Journal of Nutrition, 2011; 431.
105 (3), 400–408. [34]. Mtabho CM, Irongo C, Boeree MJ, Aarnoutse RE,
[31]. Nahid, P., Dorman, S.E., Alipanah, N., Barry, P.M., Kibiki GS: Childhood Tuberculosis in the
Brozek, J.L., Cattamanchi, A., et al., 2016. Official Kilimanjaro region: lessons from and for the TB
American Thoracic Society/Centers for Disease Programme. Trop Med Int Health 2010, 15(5):496–
Control and Prevention/Infectious Diseases Society 501.
of America Clinical Practice Guidelines: Treatment
of Drug-Susceptible Tuberculosis. Clinical Infectious
Diseases, 63 (7), e147–e195.
Table 1 Demographic and Clinical Status of Respondents (N=102)
Variable Frequency Percentages
Age in Categories
0-4 years 24 23.5
5-9 years 45 44.1
10-14 year 33 32.4
Sex of respondents
Male 49 48
Female 53 52
Respondent Nutritional Status
Malnourished 67 65.7
Normal 35 34.3
History of TB contacts
Household members 52 51
Other source of contacts 50 49
Respondents HIV status
HIV positive 23 22.5
HIV negative 79 77.5
Classification of Tuberculosis
Pulmonary 25 24.5
Extra-pulmonary 77 75.5
History of BCG Vaccine
Known
known 48 47.1
Not known 54 52.9
Method of diagnosis
Clinical 41 40.2
Bacteriological 61 59.8
Mean age is 7.7 + 3.4 years with age range of 2- 14 years.
IJISRT23NOV2075 www.ijisrt.com 2484
Volume 8, Issue 11, November – 2023 International Journal of Innovative Science and Research Technology
ISSN No:-2456-2165
Fig 1 Drug Adherence Status Among Respondents Fig 2 Treatment Out come Among Respondents
Table 2 Association between Demographic and Clinical Status and Treatment Outcome
Variables Treatment failure Treatment success X2 DF OR P
Age in Categories
0-4 years 12(50%) 12(50%) 0.64 1 0.53-4.45 0.43
5-9 years 20(44.4%) 25(55.6%) 0.19 1 0.49-3.07 0.66
10-14 year (R) 13(39.4%) 20(60.6%)
Sex
Male 22(44.9%) 27(55.1%) 0.023 1 0.49-2.32 0.88
Female 23(43.4%) 30(56.6%)
HIV Status
HIV positive 7(30.4%) 16(69.6%) 2.26 1 0.18-1.27 0.13
HIV negative 38(48.1%) 41(51.9%)
Nutritional Status
Malnourished 26(38.8%) 41(61.2%) 2.24 1 0.23-1.22 0.14
Normal 19(54.3%) 16(45.7%)
Drug adherence status
Good 0(0%) 55(100%) 94.38 1 6.06-81.21 < 0.01
Poor 45(95.7%) 2(4.3%)
Classification of Tuberculosis
Pulmonary 10(40%) 15(60%) 0.23 1 0.32-2.0 0.65
Extra-pulmonary 35(45.5%) 42(54.5%)
History of Contact
Household contact 26(50%) 26(50%) 1.49 1 0.74-3.59 0.22
Other contacts 19(38%) 31(82%)
History of BCG vaccination
Known 23(47.9%) 25(52.1%) 0.54 1 0.61-2.93 0.53
Unknown 22(40.7%) 32(59.3%)
Method of diagnosis
Clinical 17(41.5%) 24(58.5%) 0.19 1 0.38-1.86 0.84
Bacteriological 28(45.9%) 33(54.1%)
Table 3 Predictors of Unsuccessful Treatment Outcome
Variable Treatment failure Treatment success X2 AOR CI P
Drug adherence status
Good 0(0%) 55(100%) 94.38 6.06-81.21 < 0.01
Poor (R) 45(95.7%) 2(4.3%)
IJISRT23NOV2075 www.ijisrt.com 2485
You might also like
- Summative Test in SCIENCE 4 - Q2Document4 pagesSummative Test in SCIENCE 4 - Q2Marcus Malinao100% (3)
- Mypublicationin Int JResearchand Med SC Oct 2015Document9 pagesMypublicationin Int JResearchand Med SC Oct 2015Dr-Dalya ShakirNo ratings yet
- Knowledge, Attitude, Practice Towards COVID-19 Pandemic and Its Prevalence Among Hospital Visitors at Ataye District Hospital, Northeast EthiopiaDocument19 pagesKnowledge, Attitude, Practice Towards COVID-19 Pandemic and Its Prevalence Among Hospital Visitors at Ataye District Hospital, Northeast EthiopiaHandaNo ratings yet
- A Community-Based Isoniazid Preventive Therapy For PDFDocument8 pagesA Community-Based Isoniazid Preventive Therapy For PDFbekele badeNo ratings yet
- A Review of Incidence and Clinical Outcomes of Neonate With False Tooth ExtractionDocument3 pagesA Review of Incidence and Clinical Outcomes of Neonate With False Tooth ExtractionKIU PUBLICATION AND EXTENSIONNo ratings yet
- 03 Adeh Seras Yawan - Risk Factors of Multidrug-Resistant TuberculosisDocument16 pages03 Adeh Seras Yawan - Risk Factors of Multidrug-Resistant TuberculosisRose MariatiNo ratings yet
- Knowledge and Practice of Preventive Measures AgaiDocument28 pagesKnowledge and Practice of Preventive Measures AgaiJoann PunzalanNo ratings yet
- 29-D18 683 Diah-Savitri ErnawatiDocument5 pages29-D18 683 Diah-Savitri ErnawatiFikry AlbarNo ratings yet
- Journal Pone 0276730Document14 pagesJournal Pone 0276730Suryadi LimardiNo ratings yet
- Prevalence of Neonatal Jaundice at A TertiaryDocument4 pagesPrevalence of Neonatal Jaundice at A TertiaryJulia StantonNo ratings yet
- 10363-Article Text-49073-1-10-20220207Document7 pages10363-Article Text-49073-1-10-20220207Triyana Puspa DewiNo ratings yet
- Comparison of Antiretroviral Therapy Adherence Among HIV Infected Older Adults With Younger Adults in Africa: Systematic Review and Meta AnalysisDocument14 pagesComparison of Antiretroviral Therapy Adherence Among HIV Infected Older Adults With Younger Adults in Africa: Systematic Review and Meta AnalysisCliff Daniel DIANZOLE MOUNKANANo ratings yet
- 109-124 Factors Influencing Routine Immunization Uptake Among NursingDocument16 pages109-124 Factors Influencing Routine Immunization Uptake Among Nursingclement johnNo ratings yet
- Bacteriological Prevalence Tuberculosis Among Children Seen Health Facilities Nasarawa State Nigeria 2576 8484 EAST 18 121Document5 pagesBacteriological Prevalence Tuberculosis Among Children Seen Health Facilities Nasarawa State Nigeria 2576 8484 EAST 18 121fatimakh462No ratings yet
- Femi OgundeleDocument8 pagesFemi OgundeleAbdullahi nurudeenNo ratings yet
- 718-1519-1-SM 2Document6 pages718-1519-1-SM 2NicoleNo ratings yet
- 2021 - Factors Affecting Outcome of Longer Regimen Multidrug-Resistant Tuberculosis Treatment in West Java Indonesia A Retrospective Cohort StudyDocument13 pages2021 - Factors Affecting Outcome of Longer Regimen Multidrug-Resistant Tuberculosis Treatment in West Java Indonesia A Retrospective Cohort StudyNurul RifqianiNo ratings yet
- Infant Mortality Rate and Medical Care in Kaliro District, UgandaDocument9 pagesInfant Mortality Rate and Medical Care in Kaliro District, UgandaKIU PUBLICATION AND EXTENSIONNo ratings yet
- JulianaDocument39 pagesJulianaNyagawa GodkNo ratings yet
- Prognostic of Sepsis in A Congolese Pediatric Emergency Service Using PSOFA Score A Prospective StudyDocument6 pagesPrognostic of Sepsis in A Congolese Pediatric Emergency Service Using PSOFA Score A Prospective StudyInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Rabies Vaccines Its Role Challenges Considerationsand ImplicationsforDocument27 pagesRabies Vaccines Its Role Challenges Considerationsand ImplicationsforNimra Naveed ShaikhNo ratings yet
- Surveillance of Healthcare-Associated Infections in Indonesian HospitalsDocument12 pagesSurveillance of Healthcare-Associated Infections in Indonesian HospitalsRidha MardiyaniNo ratings yet
- Public Health - Vol 2 - Issue 4 - Article 5Document44 pagesPublic Health - Vol 2 - Issue 4 - Article 5kaisamerno2003No ratings yet
- Jurnal 2Document9 pagesJurnal 2Trisno Adhy KusumaNo ratings yet
- Jurnal TugasDocument10 pagesJurnal Tugasshola_shobrinasNo ratings yet
- Ajol File Journals - 494 - Articles - 112516 - Submission - Proof - 112516 5833 312396 1 10 20150204Document6 pagesAjol File Journals - 494 - Articles - 112516 - Submission - Proof - 112516 5833 312396 1 10 20150204ASK De OliveiraNo ratings yet
- Recognizable Birth Defects Among Neonatal Admissions at A Tertiary Hospital in South Western Uganda: Prevalence, Patterns and Associated FactorsDocument13 pagesRecognizable Birth Defects Among Neonatal Admissions at A Tertiary Hospital in South Western Uganda: Prevalence, Patterns and Associated FactorsInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Adhrence Article 1Document6 pagesAdhrence Article 1OBIOMA LILIAN OKWUONUNo ratings yet
- Knowledge, Attitude, and Practices of Isoniazid Preventive Therapy Among HIV-Positive Patients at Itojo Hospital, Ntungamo DistrictDocument11 pagesKnowledge, Attitude, and Practices of Isoniazid Preventive Therapy Among HIV-Positive Patients at Itojo Hospital, Ntungamo DistrictKIU PUBLICATION AND EXTENSIONNo ratings yet
- Nps D8Document7 pagesNps D8Jasper Benjamin JuradoNo ratings yet
- Sepsis Proposal1Document34 pagesSepsis Proposal1Appiah Peter OforiNo ratings yet
- AIDS & Clinical Research: Journal ofDocument7 pagesAIDS & Clinical Research: Journal ofzakiNo ratings yet
- Adenosine Deaminase Level in Drug Resistant TuberculosisDocument9 pagesAdenosine Deaminase Level in Drug Resistant TuberculosisIJAR JOURNALNo ratings yet
- Neonatal Infections PerspectiveDocument13 pagesNeonatal Infections PerspectiveYUDY LORENA GIRALDO ALFONSONo ratings yet
- Effect of COVID-19 On Doctor-Patient Relationship: Original Research ArticleDocument7 pagesEffect of COVID-19 On Doctor-Patient Relationship: Original Research ArticleMarlisa LionoNo ratings yet
- 1 s2.0 S2352304219300698 Main PDFDocument9 pages1 s2.0 S2352304219300698 Main PDFdioNo ratings yet
- DR Thesis 2015 Razia Kaniz FatimaDocument90 pagesDR Thesis 2015 Razia Kaniz FatimaNatasha AnwarNo ratings yet
- 1471 5945 13 12Document5 pages1471 5945 13 12jukilokiNo ratings yet
- Knowledge, Attitudes and Perceptions of HIV/AIDS Among Traditional Birth Attendants and Herbal Practitioners in Lagos State, NigeriaDocument7 pagesKnowledge, Attitudes and Perceptions of HIV/AIDS Among Traditional Birth Attendants and Herbal Practitioners in Lagos State, NigeriaIngrid KoutioNo ratings yet
- Afhs2002 0860Document11 pagesAfhs2002 0860shindyNo ratings yet
- Adherence To Medication Behavior Among TuberculosiDocument7 pagesAdherence To Medication Behavior Among TuberculosiPPI RSUI MBNo ratings yet
- Netal 2021Document8 pagesNetal 2021francinemeneken74No ratings yet
- JMDH 15 1069Document14 pagesJMDH 15 1069AKIM WONGNo ratings yet
- Journal Pone 0262720Document12 pagesJournal Pone 0262720cristhian manriqueNo ratings yet
- Reinforcing and Enabling Factors Involved in The Uptake of Sickle-Cell Disease Screening Among College of Education Students in NigeriaDocument10 pagesReinforcing and Enabling Factors Involved in The Uptake of Sickle-Cell Disease Screening Among College of Education Students in NigeriaIJAR JOURNALNo ratings yet
- Journal Pone 0244265Document15 pagesJournal Pone 0244265Faisal YousafNo ratings yet
- Presentation and Outcomes of Early and Late Onset Neonatal Sepsis in A Nigerian HospitalDocument10 pagesPresentation and Outcomes of Early and Late Onset Neonatal Sepsis in A Nigerian HospitalPSIK sarimuliaNo ratings yet
- Mosquito Vectors of Japanese Encephalitis Virus From Northern India - Role of BPD Hop Cage Method (PDFDrive)Document156 pagesMosquito Vectors of Japanese Encephalitis Virus From Northern India - Role of BPD Hop Cage Method (PDFDrive)gegewi7489No ratings yet
- 1732-Article Text-9637-2-10-20210208Document5 pages1732-Article Text-9637-2-10-20210208Siti lestarinurhamidahNo ratings yet
- Early Neonatal Morbidities Among Term and Late Preterm Infants in A Tertiary Care Centre - A Comparative StudyDocument4 pagesEarly Neonatal Morbidities Among Term and Late Preterm Infants in A Tertiary Care Centre - A Comparative StudyIJAR JOURNALNo ratings yet
- Vital Sign Predictors of Severe InfluenzaDocument11 pagesVital Sign Predictors of Severe InfluenzaDesiska PriciliaNo ratings yet
- BacterialmeningitisDocument9 pagesBacterialmeningitisTofik HusseinNo ratings yet
- Nigeria Paediatric 2007 PDFDocument185 pagesNigeria Paediatric 2007 PDFsusanaadolina sipathaNo ratings yet
- The Effect of Communication Family Patterns On Prevention Effort Hiv/Aids TransmissionDocument5 pagesThe Effect of Communication Family Patterns On Prevention Effort Hiv/Aids TransmissionKristiani AmbengNo ratings yet
- Prevalence of Severe Acute Respiratory Syndrome Coronavirus (SARS-CoV-2) in NigeriaDocument7 pagesPrevalence of Severe Acute Respiratory Syndrome Coronavirus (SARS-CoV-2) in NigeriaKIU PUBLICATION AND EXTENSIONNo ratings yet
- Volume: 04 Issue: 03 - May-Jun 2023Document8 pagesVolume: 04 Issue: 03 - May-Jun 2023Central Asian StudiesNo ratings yet
- Journal Pone 0254890Document16 pagesJournal Pone 0254890muhammmad haris faisalNo ratings yet
- Sociodemographic Characteristics of Patients With Advanced HIV Disease in Enugu, South-East Nigeria: A Retrospective Analysis of Program DataDocument6 pagesSociodemographic Characteristics of Patients With Advanced HIV Disease in Enugu, South-East Nigeria: A Retrospective Analysis of Program DataInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Pone 0269706Document13 pagesPone 0269706Meidita Annisa PurmanNo ratings yet
- International Journal of Pediatric Research Ijpr 9 111Document6 pagesInternational Journal of Pediatric Research Ijpr 9 111VsbshNo ratings yet
- Integration of Information Communication Technology, Strategic Leadership and Academic Performance in Universities in North Kivu, Democratic Republic of CongoDocument7 pagesIntegration of Information Communication Technology, Strategic Leadership and Academic Performance in Universities in North Kivu, Democratic Republic of CongoInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- The Effects of Liquid Density and Impeller Size with Volute Clearance on the Performance of Radial Blade Centrifugal Pumps: An Experimental ApproachDocument16 pagesThe Effects of Liquid Density and Impeller Size with Volute Clearance on the Performance of Radial Blade Centrifugal Pumps: An Experimental ApproachInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Dynamic Analysis of High-Rise Buildings for Various Irregularities with and without Floating ColumnDocument3 pagesDynamic Analysis of High-Rise Buildings for Various Irregularities with and without Floating ColumnInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Intrusion Detection and Prevention Systems for Ad-Hoc NetworksDocument8 pagesIntrusion Detection and Prevention Systems for Ad-Hoc NetworksInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Fuzzy based Tie-Line and LFC of a Two-Area Interconnected SystemDocument6 pagesFuzzy based Tie-Line and LFC of a Two-Area Interconnected SystemInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Geotechnical Assessment of Selected Lateritic Soils in Southwest Nigeria for Road Construction and Development of Artificial Neural Network Mathematical Based Model for Prediction of the California Bearing RatioDocument10 pagesGeotechnical Assessment of Selected Lateritic Soils in Southwest Nigeria for Road Construction and Development of Artificial Neural Network Mathematical Based Model for Prediction of the California Bearing RatioInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Innovative Mathematical Insights through Artificial Intelligence (AI): Analysing Ramanujan Series and the Relationship between e and π\piDocument8 pagesInnovative Mathematical Insights through Artificial Intelligence (AI): Analysing Ramanujan Series and the Relationship between e and π\piInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Breaking Down Barriers To Inclusion: Stories of Grade Four Teachers in Maintream ClassroomsDocument14 pagesBreaking Down Barriers To Inclusion: Stories of Grade Four Teachers in Maintream ClassroomsInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Importance of Early Intervention of Traumatic Cataract in ChildrenDocument5 pagesImportance of Early Intervention of Traumatic Cataract in ChildrenInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- A Novel Approach to Template Filling with Automatic Speech Recognition for Healthcare ProfessionalsDocument6 pagesA Novel Approach to Template Filling with Automatic Speech Recognition for Healthcare ProfessionalsInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Diode Laser Therapy for Drug Induced Gingival Enlaregement: A CaseReportDocument4 pagesDiode Laser Therapy for Drug Induced Gingival Enlaregement: A CaseReportInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Analysis of Factors Obstacling Construction Work in The Tojo Una-Una Islands RegionDocument9 pagesAnalysis of Factors Obstacling Construction Work in The Tojo Una-Una Islands RegionInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Occupational Safety: PPE Use and Hazard Experiences Among Welders in Valencia City, BukidnonDocument11 pagesOccupational Safety: PPE Use and Hazard Experiences Among Welders in Valencia City, BukidnonInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- The Relationship of Total Quality Management Practices and Project Performance With Risk Management As Mediator: A Study of East Coast Rail Link Project in MalaysiaDocument19 pagesThe Relationship of Total Quality Management Practices and Project Performance With Risk Management As Mediator: A Study of East Coast Rail Link Project in MalaysiaInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Comparison of JavaScript Frontend Frameworks - Angular, React, and VueDocument8 pagesComparison of JavaScript Frontend Frameworks - Angular, React, and VueInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- The Influence of Artificial Intelligence On Employment Trends in The United States (US)Document5 pagesThe Influence of Artificial Intelligence On Employment Trends in The United States (US)International Journal of Innovative Science and Research TechnologyNo ratings yet
- Organizational Factors That Influence Information Security in Smes: A Case Study of Mogadishu, SomaliaDocument10 pagesOrganizational Factors That Influence Information Security in Smes: A Case Study of Mogadishu, SomaliaInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Disseminating The Real-World Importance of Conjunct Studies of Acculturation, Transculturation, and Deculturation Processes: Why This Can Be A Useful Technique To Analyze Real-World ObservationsDocument15 pagesDisseminating The Real-World Importance of Conjunct Studies of Acculturation, Transculturation, and Deculturation Processes: Why This Can Be A Useful Technique To Analyze Real-World ObservationsInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Mediating Effect of Encouraging Attitude of School Principals On Personal Well-Being and Career Ethics of TeachersDocument10 pagesMediating Effect of Encouraging Attitude of School Principals On Personal Well-Being and Career Ethics of TeachersInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Classifying Crop Leaf Diseases Using Different Deep Learning Models With Transfer LearningDocument8 pagesClassifying Crop Leaf Diseases Using Different Deep Learning Models With Transfer LearningInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Total Cost of Ownership of Electric Car and Internal Combustion Engine Car With Performance NormalizationDocument11 pagesTotal Cost of Ownership of Electric Car and Internal Combustion Engine Car With Performance NormalizationInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Gender-Based Violence: Engaging Children in The SolutionDocument10 pagesGender-Based Violence: Engaging Children in The SolutionInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Integrating Multimodal Deep Learning For Enhanced News Sentiment Analysis and Market Movement ForecastingDocument8 pagesIntegrating Multimodal Deep Learning For Enhanced News Sentiment Analysis and Market Movement ForecastingInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Personality Factors As Predictors of The Level of Personality Functioning in Adolescence: Examining The Influence of Birth Order, Financial Status, and SexDocument10 pagesPersonality Factors As Predictors of The Level of Personality Functioning in Adolescence: Examining The Influence of Birth Order, Financial Status, and SexInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- The Relationship Between Knowledge About Halitosis and Dental and Oral Hygiene in Patients With Fixed Orthodontics at The HK Medical Center MakassarDocument4 pagesThe Relationship Between Knowledge About Halitosis and Dental and Oral Hygiene in Patients With Fixed Orthodontics at The HK Medical Center MakassarInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Development of Creative Thinking: Case Study of Basic Design StudioDocument9 pagesDevelopment of Creative Thinking: Case Study of Basic Design StudioInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Evaluation of Causes of Visual Impairment Among Bespectacled Between The Age 18-23: A Study From Tamil Nadu, IndiaDocument3 pagesEvaluation of Causes of Visual Impairment Among Bespectacled Between The Age 18-23: A Study From Tamil Nadu, IndiaInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Monetary and Non-Monetary Rewards For Employees Motivation in Tanzania Public Sector: The Management PerspectivesDocument8 pagesMonetary and Non-Monetary Rewards For Employees Motivation in Tanzania Public Sector: The Management PerspectivesInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- An Investigation Model To Combat Computer Gaming Delinquency in South Africa, Server-Based Gaming, and Illegal Online GamingDocument15 pagesAn Investigation Model To Combat Computer Gaming Delinquency in South Africa, Server-Based Gaming, and Illegal Online GamingInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- A Comparative Analysis of Pineapples (Ananas Comosus) From Different Bioethanol Sources Available in The PhilippinesDocument39 pagesA Comparative Analysis of Pineapples (Ananas Comosus) From Different Bioethanol Sources Available in The PhilippinesInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Roberts ML. Adolescent Suicide Prevention Life Experiences Contributing To Suicidal Ideation ResilienceDocument119 pagesRoberts ML. Adolescent Suicide Prevention Life Experiences Contributing To Suicidal Ideation ResilienceGê AnatmanNo ratings yet
- Trends of Development Modern Science and PracticeDocument10 pagesTrends of Development Modern Science and PracticeАлия ПануроваNo ratings yet
- High Condylectomy For The Treatment of Mandibular Condylar Hyperplasia: A Systematic Review of The LiteratureDocument12 pagesHigh Condylectomy For The Treatment of Mandibular Condylar Hyperplasia: A Systematic Review of The Literaturemarcela0426No ratings yet
- Transfusion and Apheresis Science: SciencedirectDocument5 pagesTransfusion and Apheresis Science: Sciencedirectkatherine juliaNo ratings yet
- Pituitary &thyroid NotesDocument7 pagesPituitary &thyroid NotesAli salimNo ratings yet
- Necrosis: Erbil Polytechnic University Erbil Health Technical College MLT Department Third Stage Group CDocument13 pagesNecrosis: Erbil Polytechnic University Erbil Health Technical College MLT Department Third Stage Group CRayan JabbarNo ratings yet
- Peripheral VascularDocument17 pagesPeripheral VascularBiBOYz 143No ratings yet
- Cryptogenetic Ischemic Stroke: The Role of Patent Foramen Ovale ClosureDocument3 pagesCryptogenetic Ischemic Stroke: The Role of Patent Foramen Ovale ClosureInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Ansiedad y Depresión en JóvenesDocument16 pagesAnsiedad y Depresión en JóvenesFarid AliveNo ratings yet
- What Is SepticemiaDocument3 pagesWhat Is SepticemiaYhna Nesperos GelverioNo ratings yet
- Certificate of Employment - Travel Pass SeafarersDocument1 pageCertificate of Employment - Travel Pass SeafarersAldren Gilana100% (1)
- Topic 1 - Principles of ImmunologyDocument2 pagesTopic 1 - Principles of ImmunologyKim Alyssa GoNo ratings yet
- APTT & PT Mixing StudiesDocument9 pagesAPTT & PT Mixing StudiesmarrowbiopsyNo ratings yet
- 628-Article Text-1485-1-10-20181114Document14 pages628-Article Text-1485-1-10-20181114Anggelia Hayuning AriffaNo ratings yet
- MR Prateek 60514302023 08 05 11 51 54 069 1 6 114 133357227964726067 PDFDocument7 pagesMR Prateek 60514302023 08 05 11 51 54 069 1 6 114 133357227964726067 PDFsuraj galbaleNo ratings yet
- Journal Pre-Proof: International Journal of Antimicrobial AgentsDocument9 pagesJournal Pre-Proof: International Journal of Antimicrobial AgentsBeatrizNo ratings yet
- Thesis Statement On Alzheimers DiseaseDocument7 pagesThesis Statement On Alzheimers Diseasegbwygt8n100% (1)
- POSTER Tramadol A2 PRINT PDFDocument1 pagePOSTER Tramadol A2 PRINT PDFJohnny ZinzNo ratings yet
- MPhill Resubmission Young 98100106Document442 pagesMPhill Resubmission Young 98100106Vaggelis ChadoliasNo ratings yet
- LESSON PLAN ON. Lung AbscessDocument12 pagesLESSON PLAN ON. Lung AbscessFriends ForeverNo ratings yet
- English: Quarter 1 - Module 2: Thought Organizing ToolsDocument23 pagesEnglish: Quarter 1 - Module 2: Thought Organizing ToolsGerome LoreteNo ratings yet
- Trichuris TrichiuraDocument1 pageTrichuris TrichiuravioNo ratings yet
- Notes (Health Assessment)Document23 pagesNotes (Health Assessment)Sheena Español0% (1)
- Streptocococci enDocument50 pagesStreptocococci enAndreea Ofelia RusNo ratings yet
- Alcoholic Liver Disease - A Complete SpectrumDocument160 pagesAlcoholic Liver Disease - A Complete SpectrumViju K GNo ratings yet
- Bone InjuriesDocument35 pagesBone InjuriesSharmaine CabreraNo ratings yet
- Medical Surgical NursingDocument21 pagesMedical Surgical NursingSanthosh.S.UNo ratings yet
- Urgences C.A.TDocument16 pagesUrgences C.A.TendotronixNo ratings yet
- BHP Formula No 55 Refrence - Bioplasgen 20 Homeopathic Medicine For Skin DiseasesDocument2 pagesBHP Formula No 55 Refrence - Bioplasgen 20 Homeopathic Medicine For Skin DiseasesKazy Habibur RahmanNo ratings yet