
Prevalence of Personality Disorders
Prevalence of Personality Disorders
You might also like
- Stuvia 1115751 Test Bank Varcarolis Foundations of Psychiatric Mental Health Nursing 8th Edition 1Document499 pagesStuvia 1115751 Test Bank Varcarolis Foundations of Psychiatric Mental Health Nursing 8th Edition 1Pesiflora100% (7)
- Mymaxicare Revised Brochure 2023Document15 pagesMymaxicare Revised Brochure 2023Engilbert MaqueraNo ratings yet
- MIDTERM Community Nursing 2Document24 pagesMIDTERM Community Nursing 2Will Garcia100% (2)
- Prometric Oman Sample MCQDocument10 pagesPrometric Oman Sample MCQibrahim 120% (1)
- Fundamentals of EpidemiologyDocument584 pagesFundamentals of EpidemiologyapoomamaNo ratings yet
- Biocibernetica y DolorDocument17 pagesBiocibernetica y DolorSarapzmNo ratings yet
- Personality Disorder 1: SeriesDocument10 pagesPersonality Disorder 1: SeriesJosé Ignacio SáezNo ratings yet
- Tyrer, Reed - Crawford - 2015Document10 pagesTyrer, Reed - Crawford - 2015Cynthia Barrios ArriagadaNo ratings yet
- Personality Disorder 1: SeriesDocument10 pagesPersonality Disorder 1: SeriesYasser AlghrafyNo ratings yet
- PersonalityDocument27 pagesPersonalityVineetha Valsa KumarNo ratings yet
- Dissociative Identity Disorder Research Paper TopicsDocument5 pagesDissociative Identity Disorder Research Paper TopicsqwgqavvhfNo ratings yet
- Inflexibility Processes As Predictors of Social Functioning in Chronic PsychosisDocument12 pagesInflexibility Processes As Predictors of Social Functioning in Chronic PsychosisifclarinNo ratings yet
- Chapter 14 &15Document73 pagesChapter 14 &15baconhaterNo ratings yet
- Autism. TL 2014Document15 pagesAutism. TL 2014jujucastellNo ratings yet
- Af Firming Gender Identity of Patients With Serious Mental IllnessDocument3 pagesAf Firming Gender Identity of Patients With Serious Mental IllnessdelandrethNo ratings yet
- Social Anxiety Disorder in Review: Two Decades of ProgressDocument20 pagesSocial Anxiety Disorder in Review: Two Decades of ProgressResidentes INPRFMNo ratings yet
- Depression Research PaperDocument8 pagesDepression Research Paperapi-312817381100% (1)
- AQUINOFAVIS FinalDraft DAYZERO PDFDocument37 pagesAQUINOFAVIS FinalDraft DAYZERO PDFTurtle WildNo ratings yet
- DepressionDocument5 pagesDepressionapi-356602462100% (1)
- 10 - ASD, Lord 2018Document53 pages10 - ASD, Lord 2018Grijisha ChandranNo ratings yet
- Mental Health Is Biological Health. Why Tackling Diseases of The Mind Is An Imperative For Biological Anthropology in The 21st CenturyDocument31 pagesMental Health Is Biological Health. Why Tackling Diseases of The Mind Is An Imperative For Biological Anthropology in The 21st CenturyWalter VillalobosNo ratings yet
- The Impact of Mental Illness Stigma PDFDocument34 pagesThe Impact of Mental Illness Stigma PDFJuan David SanzNo ratings yet
- Depression and Trauma A Transgenerational Psychoanalytic PerspectiveDocument20 pagesDepression and Trauma A Transgenerational Psychoanalytic PerspectiveAnonymous 18EBcIw2C100% (1)
- cpn-12-171 (171-179) PDFDocument9 pagescpn-12-171 (171-179) PDFRiski Wahyudi LasarikaNo ratings yet
- Literature Review of Effective Treatment For Dissociative Identity DisorderDocument7 pagesLiterature Review of Effective Treatment For Dissociative Identity Disorderc5t6h1q5No ratings yet
- Personality DisordersDocument5 pagesPersonality DisordersFabianNo ratings yet
- Research DossierDocument24 pagesResearch Dossierapi-300458195No ratings yet
- Suicide Prevention in Psychiatric PatientsDocument11 pagesSuicide Prevention in Psychiatric PatientsDaniela DiazNo ratings yet
- Intelligence and Personality As PredictorsDocument96 pagesIntelligence and Personality As PredictorsTrifan DamianNo ratings yet
- The Social Construction and Reframing of ADHDDocument13 pagesThe Social Construction and Reframing of ADHDJustin M.100% (1)
- Pyc1512 Unit 2Document21 pagesPyc1512 Unit 2maciabhenguNo ratings yet
- Vass 2015Document9 pagesVass 2015Amina LabiadhNo ratings yet
- Day 1 Intro RV Rushed Version For 2018Document30 pagesDay 1 Intro RV Rushed Version For 2018api-391411195No ratings yet
- The Antisocial Personality Disorder and Its Characteristics, Changes and Advances: A ChallengeDocument8 pagesThe Antisocial Personality Disorder and Its Characteristics, Changes and Advances: A ChallengeMerritaNo ratings yet
- An Overview of Autism Spectrum Disorder, Heterogeneity and Treatment OptionsDocument11 pagesAn Overview of Autism Spectrum Disorder, Heterogeneity and Treatment OptionsMaria Clara FeitosaNo ratings yet
- Themisconceptionsofmentalillness and Thestigmathatfollows Mini Ethnographyoriginaldraft2Document13 pagesThemisconceptionsofmentalillness and Thestigmathatfollows Mini Ethnographyoriginaldraft2api-437840816No ratings yet
- Paper 7Document31 pagesPaper 7DrAqeel AshrafNo ratings yet
- Jasminem Miniethno FinalversionDocument16 pagesJasminem Miniethno Finalversionapi-437840816No ratings yet
- Journal of Affective Disorders: Social Anxiety and Depression Stigma Among AdolescentsDocument10 pagesJournal of Affective Disorders: Social Anxiety and Depression Stigma Among AdolescentsPutri Indah PermataNo ratings yet
- JOURNAL CLUB NewDocument61 pagesJOURNAL CLUB Newaastha panthNo ratings yet
- The Lead-In : "List of People With Bipolar Disorder.")Document13 pagesThe Lead-In : "List of People With Bipolar Disorder.")api-321363387No ratings yet
- 1-Transidentities and Autism Spectrum Disorder A Systematic ReviewDocument14 pages1-Transidentities and Autism Spectrum Disorder A Systematic ReviewpietrovbhpNo ratings yet
- Chapter 22. SomatizationDocument14 pagesChapter 22. SomatizationDiego Francesco MacaliNo ratings yet
- An Overview of Autism Spectrum Disorder, Heterogeneity and Treatment OptionsDocument11 pagesAn Overview of Autism Spectrum Disorder, Heterogeneity and Treatment OptionsDiego CampillayNo ratings yet
- Psychopathology in Women: Incorporating Gender Perspective into Descriptive PsychopathologyFrom EverandPsychopathology in Women: Incorporating Gender Perspective into Descriptive PsychopathologyMargarita Sáenz-HerreroNo ratings yet
- Ansiedade SocialDocument12 pagesAnsiedade Socialvemec31798No ratings yet
- Ijpher: Research ArticleDocument9 pagesIjpher: Research ArticlePremier PublishersNo ratings yet
- Research Paper FinalDocument10 pagesResearch Paper Finalapi-300458195No ratings yet
- JAMWA Article - HopenwasserDocument24 pagesJAMWA Article - HopenwasserSex & Gender Women's Health CollaborativeNo ratings yet
- Mental Health Literacy and Anxiety Disorder PDFDocument11 pagesMental Health Literacy and Anxiety Disorder PDFShabrina Patriavy BennaradictaNo ratings yet
- Depression Taj Article 201116 Widdowson FinalDocument15 pagesDepression Taj Article 201116 Widdowson Finalvince yumulNo ratings yet
- Health Impact Framework - CollinsDocument12 pagesHealth Impact Framework - Collinsapi-355764752No ratings yet
- Mental Illness StigmaDocument27 pagesMental Illness StigmaAneehNo ratings yet
- Anthropology Research ReportDocument15 pagesAnthropology Research ReportSyeda Ramsha RizviNo ratings yet
- Livingwithschizophrenia KMDocument9 pagesLivingwithschizophrenia KMapi-285356333No ratings yet
- Demographic and Clinical Correlates of Suicidality in Adolescents Attending A Specialist Community Mental Health Service: A Naturalistic StudyDocument6 pagesDemographic and Clinical Correlates of Suicidality in Adolescents Attending A Specialist Community Mental Health Service: A Naturalistic StudyAna Paula Soares GondimNo ratings yet
- Final Research PaperDocument17 pagesFinal Research Paperapi-451460387No ratings yet
- Prac2 CpsirDocument30 pagesPrac2 CpsirSrishti GaurNo ratings yet
- HHS Public Access: Social Epidemiology of Depression and Anxiety by Gender IdentityDocument12 pagesHHS Public Access: Social Epidemiology of Depression and Anxiety by Gender Identitychoi yeontteomeokNo ratings yet
- Research Paper Topics Mental IllnessDocument5 pagesResearch Paper Topics Mental Illnessafmcueagg100% (1)
- Primer: Autism Spectrum DisorderDocument23 pagesPrimer: Autism Spectrum DisorderMakanudo.No ratings yet
- Final Honours Thesis-10Document23 pagesFinal Honours Thesis-10api-288362330No ratings yet
- Depression and Trauma - A Transgenerational Psychoanalytic PerspectiveDocument20 pagesDepression and Trauma - A Transgenerational Psychoanalytic PerspectiveCarlos DevotoNo ratings yet
- Final PaperDocument25 pagesFinal Paperapi-495169810No ratings yet
- Borderline Personality Disorder EssayDocument7 pagesBorderline Personality Disorder Essayapi-574298740No ratings yet
- Stress in AutismDocument38 pagesStress in Autismmatt lordNo ratings yet
- Design and Analysis of Various Formwork SystemsDocument6 pagesDesign and Analysis of Various Formwork SystemsInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Reintegration of Dairy in Daily American Diets: A Biochemical and Nutritional PerspectiveDocument1 pageReintegration of Dairy in Daily American Diets: A Biochemical and Nutritional PerspectiveInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Nurturing Corporate Employee Emotional Wellbeing, Time Management and the Influence on FamilyDocument8 pagesNurturing Corporate Employee Emotional Wellbeing, Time Management and the Influence on FamilyInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Occupational Injuries among Health Care Workers in Selected Hospitals in Ogbomosho, Oyo StateDocument6 pagesOccupational Injuries among Health Care Workers in Selected Hospitals in Ogbomosho, Oyo StateInternational Journal of Innovative Science and Research Technology100% (1)
- Appraisal of Nursing Care Received and it’s Satisfaction: A Case Study of Admitted Patients in Afe Babalola Multisystem Hospital, Ado Ekiti, Ekiti StateDocument12 pagesAppraisal of Nursing Care Received and it’s Satisfaction: A Case Study of Admitted Patients in Afe Babalola Multisystem Hospital, Ado Ekiti, Ekiti StateInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Evaluation of Lateral and Vertical Gingival Displacement Produced by Three Different Gingival Retraction Systems using Impression Scanning: An in-Vivo Original StudyDocument6 pagesEvaluation of Lateral and Vertical Gingival Displacement Produced by Three Different Gingival Retraction Systems using Impression Scanning: An in-Vivo Original StudyInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Salivary Diagnostics in Oral and Systemic Diseases - A ReviewDocument5 pagesSalivary Diagnostics in Oral and Systemic Diseases - A ReviewInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Prevalence of Microorganisms in UTI and Antibiotic Sensitivity Pattern among Gram Negative Isolates: A Cohort StudyDocument4 pagesPrevalence of Microorganisms in UTI and Antibiotic Sensitivity Pattern among Gram Negative Isolates: A Cohort StudyInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Biometric Security Systems Enhanced by AI: Exploring Concerns with AI Advancements in Facial Recognition and Other Biometric Systems have Security Implications and VulnerabilitiesDocument5 pagesBiometric Security Systems Enhanced by AI: Exploring Concerns with AI Advancements in Facial Recognition and Other Biometric Systems have Security Implications and VulnerabilitiesInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- MSMEs and Rural Prosperity: A Study of their Influence in Indonesian Agriculture and Rural EconomyDocument6 pagesMSMEs and Rural Prosperity: A Study of their Influence in Indonesian Agriculture and Rural EconomyInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Shift from Traditional to Modern Building Concepts and Designs in Ringim Town: A Comparative Study of Aesthetics, Values, Functions and DurabilityDocument9 pagesShift from Traditional to Modern Building Concepts and Designs in Ringim Town: A Comparative Study of Aesthetics, Values, Functions and DurabilityInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Fuzzy based Tie-Line and LFC of a Two-Area Interconnected SystemDocument6 pagesFuzzy based Tie-Line and LFC of a Two-Area Interconnected SystemInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- An Explanatory Sequential Study of Public Elementary School Teachers on Deped Computerization Program (DCP)Document7 pagesAn Explanatory Sequential Study of Public Elementary School Teachers on Deped Computerization Program (DCP)International Journal of Innovative Science and Research TechnologyNo ratings yet
- Dynamic Analysis of High-Rise Buildings for Various Irregularities with and without Floating ColumnDocument3 pagesDynamic Analysis of High-Rise Buildings for Various Irregularities with and without Floating ColumnInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- AI Robots in Various SectorDocument3 pagesAI Robots in Various SectorInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Intrusion Detection and Prevention Systems for Ad-Hoc NetworksDocument8 pagesIntrusion Detection and Prevention Systems for Ad-Hoc NetworksInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Geotechnical Assessment of Selected Lateritic Soils in Southwest Nigeria for Road Construction and Development of Artificial Neural Network Mathematical Based Model for Prediction of the California Bearing RatioDocument10 pagesGeotechnical Assessment of Selected Lateritic Soils in Southwest Nigeria for Road Construction and Development of Artificial Neural Network Mathematical Based Model for Prediction of the California Bearing RatioInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- The Effects of Liquid Density and Impeller Size with Volute Clearance on the Performance of Radial Blade Centrifugal Pumps: An Experimental ApproachDocument16 pagesThe Effects of Liquid Density and Impeller Size with Volute Clearance on the Performance of Radial Blade Centrifugal Pumps: An Experimental ApproachInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- A Novel Approach to Template Filling with Automatic Speech Recognition for Healthcare ProfessionalsDocument6 pagesA Novel Approach to Template Filling with Automatic Speech Recognition for Healthcare ProfessionalsInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Innovative Mathematical Insights through Artificial Intelligence (AI): Analysing Ramanujan Series and the Relationship between e and π\piDocument8 pagesInnovative Mathematical Insights through Artificial Intelligence (AI): Analysing Ramanujan Series and the Relationship between e and π\piInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Integration of Information Communication Technology, Strategic Leadership and Academic Performance in Universities in North Kivu, Democratic Republic of CongoDocument7 pagesIntegration of Information Communication Technology, Strategic Leadership and Academic Performance in Universities in North Kivu, Democratic Republic of CongoInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Importance of Early Intervention of Traumatic Cataract in ChildrenDocument5 pagesImportance of Early Intervention of Traumatic Cataract in ChildrenInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Comparison of JavaScript Frontend Frameworks - Angular, React, and VueDocument8 pagesComparison of JavaScript Frontend Frameworks - Angular, React, and VueInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Diode Laser Therapy for Drug Induced Gingival Enlaregement: A CaseReportDocument4 pagesDiode Laser Therapy for Drug Induced Gingival Enlaregement: A CaseReportInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Organizational Factors That Influence Information Security in Smes: A Case Study of Mogadishu, SomaliaDocument10 pagesOrganizational Factors That Influence Information Security in Smes: A Case Study of Mogadishu, SomaliaInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Breaking Down Barriers To Inclusion: Stories of Grade Four Teachers in Maintream ClassroomsDocument14 pagesBreaking Down Barriers To Inclusion: Stories of Grade Four Teachers in Maintream ClassroomsInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Occupational Safety: PPE Use and Hazard Experiences Among Welders in Valencia City, BukidnonDocument11 pagesOccupational Safety: PPE Use and Hazard Experiences Among Welders in Valencia City, BukidnonInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Analysis of Factors Obstacling Construction Work in The Tojo Una-Una Islands RegionDocument9 pagesAnalysis of Factors Obstacling Construction Work in The Tojo Una-Una Islands RegionInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- The Influence of Artificial Intelligence On Employment Trends in The United States (US)Document5 pagesThe Influence of Artificial Intelligence On Employment Trends in The United States (US)International Journal of Innovative Science and Research TechnologyNo ratings yet
- Disseminating The Real-World Importance of Conjunct Studies of Acculturation, Transculturation, and Deculturation Processes: Why This Can Be A Useful Technique To Analyze Real-World ObservationsDocument15 pagesDisseminating The Real-World Importance of Conjunct Studies of Acculturation, Transculturation, and Deculturation Processes: Why This Can Be A Useful Technique To Analyze Real-World ObservationsInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Environmental Health-A Branch of Public Second StrategyDocument7 pagesEnvironmental Health-A Branch of Public Second StrategyhelloaNo ratings yet
- Hospital Guide Better Being ThailandDocument7 pagesHospital Guide Better Being ThailandNenad PavlovićNo ratings yet
- Scientific Research Journal of India SRJI Vol-3 Issue-3 Year 2014Document209 pagesScientific Research Journal of India SRJI Vol-3 Issue-3 Year 2014Dr. Krishna N. SharmaNo ratings yet
- The Fountain of Youth? The Quest For Aging TherapiesDocument5 pagesThe Fountain of Youth? The Quest For Aging TherapiesRichaRd MetcalfeNo ratings yet
- Natural History of DiseaseDocument9 pagesNatural History of DiseaseAan Sucitra Hollan Fm'sNo ratings yet
- Materi Sistem ImunDocument23 pagesMateri Sistem ImunsahabatrumahsakitNo ratings yet
- Childhood Obesity in The Rio Grande ValleyDocument6 pagesChildhood Obesity in The Rio Grande ValleydjwickedNo ratings yet
- Ec Creating Energy CirclesDocument10 pagesEc Creating Energy CirclesRadhika Goel100% (1)
- English For Physiotherapists - Angielski Dla FizjoterapiiDocument112 pagesEnglish For Physiotherapists - Angielski Dla FizjoterapiiSabina RuszkowskaNo ratings yet
- USHC ReviewDocument119 pagesUSHC ReviewArman DhillonNo ratings yet
- KCR Full 10-11-17Document20 pagesKCR Full 10-11-17Ryan CronkNo ratings yet
- Global Health and Scientific Research (Flory, 2004)Document30 pagesGlobal Health and Scientific Research (Flory, 2004)Faz RahmanNo ratings yet
- 4th Quarter Pointers To ReviewDocument1 page4th Quarter Pointers To Review박소민No ratings yet
- ASC Code of Ethics Updated 2010Document28 pagesASC Code of Ethics Updated 2010Ganch Aguas50% (2)
- Micro MicrobiotaDocument7 pagesMicro MicrobiotaJustinNo ratings yet
- TE Chapter 1Document45 pagesTE Chapter 1tooba khanNo ratings yet
- OPD Form IhealthcareDocument2 pagesOPD Form IhealthcareSanjay PatilNo ratings yet
- Disability Studies and The Academy-Past, Present, and FutureDocument10 pagesDisability Studies and The Academy-Past, Present, and FutureMicahNo ratings yet
- Vaccine Development, From The Lab To The Clinic (Jim Tartaglia)Document14 pagesVaccine Development, From The Lab To The Clinic (Jim Tartaglia)National Press FoundationNo ratings yet
- DO 010 s.2023Document4 pagesDO 010 s.2023Gladys BiscochoNo ratings yet
- Case Management Assessment FormDocument13 pagesCase Management Assessment FormDiksha PadamNo ratings yet
- Homeopathy Questionnaire 2Document30 pagesHomeopathy Questionnaire 2SanjeevNo ratings yet
- We Are Like Co WifesDocument9 pagesWe Are Like Co WifesTricianne Merielle S. Bano-oyNo ratings yet
- Endosulfan Tragedy in Kasaragod - Did It Really Happen?Document18 pagesEndosulfan Tragedy in Kasaragod - Did It Really Happen?K.m.SreekumarNo ratings yet























































































































Volume 8, Issue 11, November 2023 International Journal of Innovative Science and Research Technology
ISSN No:-2456-2165
Prevalence of Personality Disorders
Masood Ahmad Naushad. Fazel Rahman Hashir.
MD. MPH, Lecturer in the Medical faculty of Mirwais MD, Dean and lecturer of the Medical faculty of Mirwais
Neeka Institute of Higher Education, Neeka Institute of Higher Education,
Kandahar, Afghanistan Kandahar, Afghanistan
Abstract:- Globally the concept of personality disorder It is impossible to comprehend personality problems
was not clearly defined in the mental health until the apart from healthy personalities, nevertheless. Personality
1980s,Later, the DSM fully defined personality disorders are a variation of a normal, healthy personality as
disorders, and a new challenge to the world was born in everyone has a personality (even if not everyone
the field of mental health.There has not been much experiences epileptic seizures). In the same way that a
researches on the subject of personality disorder, square is a specific example of the more general construct of
especially on the occurrence of personality disorder. a rectangle, so too does a personality disorder exist as a
However, there are many types of personality disorder special case of a normal, healthy personality. For this
and each type has its own symptoms and signs, that is reason, it is helpful if we start talking about personality
why researchers are not interested in this topic.On the disorders by talking about the more generic, larger concept
other hand, the occurrence of this disorder is increasing of personality.
day by day, and this disorder is often found in a person
as comorbid with other mental illnesses (depression, The permanent characteristics of a person that manifest
Anxiety, Mood disorder).But in any case, an effort has in their behavior under a range of conditions are referred to
been made in this study to be able to understand the as their personality (Oxford Textbook of Psychiatry, 2018).
definition and types of personality disorder by review of A personality disorder is defined as a persistent pattern of
other studies in globally pattern. And also, through this inner experience and behavior that significantly deviates
research, we can fully understand the causes of from the expectations of the person's culture. It begins in
personality differences, of course, these causes are adolescence or early adulthood, is pervasive and unyielding,
related to geographical locations in the world.Through remains stable over time, and causes distress or functional
this study, we have obtained complete information about impairment. (DSM-5, 18 May 2013, Diagnostic and
the prevalence of personality disorders in the world, Statistical Manual of Mental Disorders, Fifth Edition).
USA and India.
II. BACKGROUND
Keywords:- Personality disorders, prevalence, clusters.
Based on the research that has been done, mental
I. INTRODUCTION illnesses are among the most significant and crucial aspects
of the total burden of diseases. According to the 2015 global
A person with a "personality disorder" is said to have a burden of diseases report, one of the primary causes of the
personality that is not quite right. But the term "personality global burden of illnesses is mental disorders.(Oxford
disorder" only designates a diagnostic group of mental Textbook of Psychiatry, 2018).
illnesses that are marked by a persistent, rigid, and
maladaptive way of interacting with the outside world. How It is estimated that approximately 900 million people
someone thinks, feels, and acts is clearly indicative of this in the world suffer from mental illnesses, accounting for
maladaptive habit. Negative effects on interpersonal 19% of the world's total population. The personality
interactions are the most prominent and noteworthy disorders are the most important and significant components
characteristic of these diseases. connections with others are of psychiatric disorders. (Oxford Textbook of Psychiatry,
seldom long-lasting, fulfilling, and meaningful for an 2018).
individual with an untreated personality disorder, and the
connections they do have are frequently troubled by issues Since the fourth century BC, philosophers have been
and challenges. trying to understand what it is that makes ‘us’ what we are.
A "personality disorder" diagnosis does not imply that The term ‘personality’ has been used since the
a person is a freak of nature or that their personality is eighteenth century to label distinguishing qualities of a
gravely defective. These diseases are really rather prevalent, person. (Quality of physical health care among patients with
and people who are diagnosed with them experience intense personality disorder)
pain and distress. It is estimated that 10% of individuals may Over the past half-century, personality disorders have
have a personality disorder, according to studies on the gained enough recognition and knowledge to be treated on
incidence of personality disorders conducted in various an equal footing with other mental illnesses. (Oxford
nations and among various groups (Torgersen, 2005). A full Textbook of Psychiatry, 2018).
and entire departure from normal and healthy functioning is
indicative of many different types of diseases (e.g.,
epilepsy).
IJISRT23NOV1396 www.ijisrt.com 2530
Volume 8, Issue 11, November 2023 International Journal of Innovative Science and Research Technology
ISSN No:-2456-2165
Before the 1960s, personality disorder was seen as an socioeconomic level, renting, and residing in an urban
inaccurate diagnostic with little to no clinical utility, with location.
the probable exception of the antisocial group. after then,
nevertheless, there has been a growing awareness that Using DSM-IV diagnostic criteria, Grant et al. (2004)
personality disorder may be accurately defined and graded, reported on a national epidemiological study (n=43,093) of
even in spite of several flaws in its categorization, especially prevalence and correlates in the US. They state that 14.79%
after the release of DSM-III in 1980. When present as a of people suffered from a personality disorder. The most
comorbid disease, personality disorder has been common personality disorder was obsessive compulsive
demonstrated to have a significant impact on the course of disorder (7.8%); women were substantially more likely than
other mental disorders and may benefit from specialized males to have avoidant, dependent, and paranoid personality
therapy. (The Cost of Mental Health Care for Personality disorders (p<.05), whereas men were significantly more
Disorders, 2008). likely to have antisocial personality disorder (p<.05).
Generally speaking, risk factors included being Black or
III. LITERATURE REVIEW Native American, being a young adult, having a poor
socioeconomic level, having been widowed, divorced,
A study of the literature on the prevalence and results separated, or never married. Using DSM-IV diagnostic
of personality disorders was conducted. We conducted a criteria, Lenzenweger et al. (2007) reported on a National
literature search using the following terms, both alone and in Comorbidity Survey Replication (NCS-R) of prevalence and
combination, on CINAHL, Medline, PsycINFO, and Google correlates (n=5692) in the US.
Scholar: personality disorder, prevalence pharmacological,
psychotherapy, therapeutic connection, and alliance. Our 9.1% of people had at least one personality disorder,
search for literature was restricted to research on with the following clusters having the highest incidence
pharmaceutical and psychological interventions. Throughout rates: A (5.7%), B (1.5%), and C (6%). Antisocial
the 1990s, the incidence of personality disorders in general personality disorder was generally less common in women;
populations remained mostly unknown and impossible to unemployment was positively correlated with borderline
adequately measure (Lenzenweger, 2008). Numerous personality disorder (39%) while age and education were
studies are constrained by their dependence on self- inversely correlated with cluster B disorders. Each cluster's
reporting, clinician interviews, telephone interviews, members (A =25%, B =49.1%, and C =29%) reported
unrepresentative sample, and control groups from other having had treatment for either drug abuse or mental health
research, and have lacked rigorous epidemiological rigor concerns in the 12 months before.Prevalence studies vary in
(Coid et al., 2006). Nonetheless, a number of foreign their findings; in the United States, one research found that
research have contributed to the body of knowledge about around 1 in 10 persons, in Australia, 1 in 15 people, and in
prevalence rates. Using ICD-10 diagnostic criteria, Jackson Great Britain, 1 in 20 people met the criteria for personality
and Burgess (2000) carried out a national epidemiological disorder.
assessment of personality disorder in Australia (n=10,641).
Using weighted replicate weights to represent population Rather than being related to population demographics,
demographics, it was estimated that 6.5% of Australians these discrepancies are most likely the result of various
suffered from at least one personality disorder, of which 704 sample techniques, various diagnostic tools, and the quantity
respondents had at least one. Male, younger, and single of disordered categories covered (Coid et al., 2006). These
individuals were more likely to suffer from personality studies provide insight into the significant frequency of
disorders. personality disorders in society, with 5–10% of people
possibly suffering from the condition.
Using DSM-IV diagnostic criteria, Coid et al. (2006)
reported on a nationwide assessment of personality disorder In clinical settings for mental health, prevalence and
prevalence and correlates (n=626) in Great Britain. Men had comorbidity Due to the paucity of published research in this
a greater weighted prevalence (5.4%) than women (3.4%), field, it is challenging to determine the precise frequency of
with a weighted prevalence of 4.4%. There were no reports personality disorder in mental health clinical settings;
of narcissistic or histrionic personality disorders, and the nonetheless, estimates range from 36% to 67% (National
weighted total prevalence of individual illnesses ranged Institute for Mental Health in England, 2003).
from 0.06% to 1.9%. Obsessive compulsive personality
disorder was the most common (1.9%). The most common Personality disorder is highly comorbid with a variety
cluster of personality disorders was cluster C (2.6%), of axis I disorders, according to the literature (Jackson &
followed by cluster A (1.6%) and cluster B (1.2%). People Burgess, 2000; Leichsenring & Leibing, 2003;
with a cluster B diagnosis were more likely to have served Lenzenweger, 2008). As a result, people with personality
time in prison, have a criminal record, or have been in disorder frequently use a wide range of primary care and
institutional or local authority care; people with a cluster C mental health services. In the NCS-R, Lenzenweger et al.
diagnosis were more likely to have received psychotropic (2007) discovered that 39% of participants had received
medication and counseling. Individuals with a cluster A treatment for a mental health or substance addiction issue in
diagnosis were three times more likely to have been in local the year prior, and that this correlation was highest with
authority care as a minor. According to Coid et al. (2006), cluster B illnesses. In an American research (n=664),
impacted people were primarily male, older, single or Bender et al. (2001) discovered that 81% of the participants
divorced, jobless or economically inactive, from a lower in the four representative personality disorder groups
IJISRT23NOV1396 www.ijisrt.com 2531
Volume 8, Issue 11, November 2023 International Journal of Innovative Science and Research Technology
ISSN No:-2456-2165
(schizotypal, borderline, avoidant, and obsessive- Cluster C: Anxious, fearful, controlling
compulsive personality disorder) had taken psychotropic behaviorsAvoidant, Dependent, Obsessive-Compulsive
medication, and 96% had undergone psychotherapy. In Disorders
therapeutic settings, personality disorder is underdiagnosed
despite its high comorbid frequency, and its detrimental Other Personality Disorders
effects on treatment results are not well understood (Bender Personality changes due to a medical condition-
et al., 2001). Disturbance due to the direct physiological effects of a
medical condition (e.g., frontal lobe lesion).
IV. METHODOLOGY Other Specified or unspecified personality disorders-
The personality pattern meets the criteria for a
A review of the literature on personality disorders' personality disorder, or there are qualities present that
prevalence, risk factors, and outcomes is being done as might be associated with many personality disorders but
library research. The following keywords, both alone and in do not fit the criteria for a particular personality disorder.
combination, were used to search for this work using Or the person is thought to suffer from a personality
CINAHL, Medline, PsycINFO, Google Scholar, and Oxford disorder that isn't covered by the DSM 5 (such as
Textbook of Psychiatry: personality disorder, prevalence, depressed or passive-aggressive personality disorders,
etiology, pharmacology, psychotherapy, therapeutic which were classified differently in the DSM IV).
connection, and alliance. Our search for literature was
restricted to research on pharmaceutical and psychological A. Cluster A - Paranoid, Schizoid, Schizotypal Disorders
interventions. Gender: more common in males
Be mindful of how other cultures view certain
A. Objectives
behaviors.
To identify behaviors associated with personality
Onset – This type of conduct typically manifests in
disorders.
childhood and adolescence, and it is marked by
To know the prevalence of personality disorders.
isolation, strained peer relationships, academic
To identify the risk factors of personality disorders underachievement, and being teased. People view
globally. individuals as strange or eccentric.
To distinguish the symptoms of different personality Etiology - Neurophysiology, genetics
disorders.
Familial pattern: increased prevalence of schizophrenia
To describe the available options of treatment for and delusional disorders in family system.
personality disorders.
Schizotypal Disorder patients
B. Finding
“Ideas of reference”- believes others are talking about
This research has a library basis. After studying the
them, even the TV and songs on the radio are about
journals and books under the title of personality disorder,
them, and often feels others stare at them.
we have achieved such a finding. Based on these findings,
Believe they receive special messages, have experiences
we are able to explain the definition of personality
with the supernatural and can make things happen by
disorder and its types in detail. And also, with the help of
wishing (magical thinking).
these findings, we can now correctly clarify the etiology,
epidemiology, and prevention methods and treatment Their behavior or appearance is odd, eccentric or
types of personality disorders in the world, which will be peculiar.
fully understood in the next pages. Affect is constricted or inappropriate.
No close friends or confidants.
C. Key features in personality disorders Excessive social anxiety.
The individual approaches relationships and the
environment in a rigid and dysfunctional way. The person's Paranoid Personality Disorder
demands, views, and behaviors frequently create vicious Suspicious,Feelings unfounded suspicion that others are
loops that support unhealthy practices and elicit unfavorable taking advantage of, hurting, or misleading them;
responses from others. When put in difficult conditions, the distrustful of others.
individual lacks resilience and has erratic and fragile coping tenacious in holding grudges and slow to forgive those
mechanisms. who may have offended them.
Unable to form intimate relationships, and when they do,
V. THREE CLUSTERS OF PERSONALITY often suspect partner has been unfaithful
DISORDERS Usually distant or irrationally furious and violent,
especially when they feel insulted.
Cluster A: Odd, eccentric behaviorsParanoid, Schizoid
& Schizotypal . Schizoid Personality Disorder
Neither wants nor appreciates being in close ties, such as
Cluster B: Dramatic, erratic, emotional
a family.
behaviorsAntisocial, Borderline, Histrionic, Narcissistic
almost usually opts for alone pursuits.
Disorders
has little desire to engage in sexual activity with another
individual.
IJISRT23NOV1396 www.ijisrt.com 2532
Volume 8, Issue 11, November 2023 International Journal of Innovative Science and Research Technology
ISSN No:-2456-2165
Unaffected by compliments or disapproval. Antisocial Personality Disorder
Flattened affect: the belief that few things truly bring Must be at least age 18, but there is evidence of Conduct
them joy and that nothing truly makes them happy or Disorder with onset before age 15, includes:
unhappy. Fighting, bullying, weapons use including a bat, sticks,
broken bottle, bricks, rocks, knife or gun.
B. Cluster B - Antisocial, Borderline, Histrionic, Deliberately cause suffering, pain or torture to other
Narcissistic people or animals.
Gender Stole while confronting victim such as mugging, purse
Male - Antisocial PD snatching, extortion or armed robbery.
Female - Borderline PD, Histrionic PD Forced someone into sexual activity.
Age – All diagnosed after age 18 and may see Set fires or vandalized or broke into property.
some decrease in symptoms at midlife. Stole items of nontrivial value while shoplifting, theft,
Etiology - Neurophysiology, genetics forgery.
High rates of depression, substance abuse Ran away from home at least twice while living in
parental or parental surrogate home.
Borderline Personality Disorder
Staying out very late at night despite parental
Frantic efforts to avoid real or imagined abandonment.
prohibitions or often skipping school before the age of
Extreme ups and downs in relationships.
13.
Identity disturbance, frequently changing beliefs and
goals. C. Cluster C- Avoidant, Dependent, Obsessive-Compulsive
Impulsivity can include unsafe sex, substance abuse, Gender
spending, eating or driving reckless. Male - OCPD 2:1
Suicidal gestures and/or self-mutilation common. Female - Dependent
Sudden mood changes, temper outbursts and feeling Etiology - Genetic, environment
empty inside.
Avoidant Personality Disorder
Developmental Factors: Borderline Personality Avoids jobs or tasks that involve interpersonal contact
Disorder because of fear of criticism, disapproval or rejection.
Developmental theory suggests that the borderline Unwilling to take initiative or become involved with
person fails to achieve object constancy during the someone unless certain that they will be liked.
separation-individuation stage of psychosocial Find it very difficult to be honest about thoughts and
development (the period between 18 months &3 years of feelings with anyone out of fear of being ridiculed.
age). Fail to complete separation from primary caretaker Fear about being criticized in social situations.
& fail to achieve autonomy in childhood. Believes that they are not as good, smart, attractive as
Often emotionally, physically or sexually abused. 25% most other people.
also have diagnosis of PTSD (Stuart, 2013). Reluctant to try new activities or meet new people.
Histrionic Personality Disorder Dependent Personality Disorder
Likes to be the center of attention and feels Needs advice or reassurance before making everyday
uncomfortable when not. decisions like what to wear or what to order at a
Sexually provocative, inappropriately seductive. restaurant.
Tries to draw attention to self by the way they dress or Depends on others to handle responsibilities such as
look and displays dramatic emotions. finances, childcare, living arrangements.
Suggestible, often changing their mind about things Finds it difficult to disagree with others even when you
based on things they’ve read or seen on TV. think they are wrong, wanting their approval.
Considers relationships to be more intimate than they Finds it difficult to start or work on tasks if no one is
really are (lots of very close friends?) there to help, due to lack of self-confidence.
Narcissistic Personality Disorder Will volunteer to do unpleasant tasks solely to gain
approval from others.
Grandiose sense of self-importance, exaggerates
achievements and talents. Preoccupied fears of being left alone or being unable to
take care of one’s self if relationship ends.
Preoccupation with fantasies of success, power, fame,
brilliance, beauty or ideal love. Obsessive-Compulsive Personality Disorder
Feels special, entitled and deserves privilege and that Preoccupied with details, lists, order, rules, organization
there are few people worth their attention. or schedules, to the extent that the major point of the
Exploitive- takes advantage of others to achieve own activity is lost.
desires “steps on toes”. Shows perfectionism to the point of having trouble
Not interested in other people’s feelings or problems, finishing tasks because the spend so much time trying to
lacking empathy. get things exactly right.
Often envious of others or believes others are envious of So devoted to school or work, never taking time to just
them. have fun or spend money on self or others.
IJISRT23NOV1396 www.ijisrt.com 2533
Volume 8, Issue 11, November 2023 International Journal of Innovative Science and Research Technology
ISSN No:-2456-2165
Inflexible on matters of morality, ethics, or values. VII. FACTORS IN THE DEVELOPMENT OF
Unable to discard items, even if space is cluttered. PERSONALITY IN INDIA
Stubborn and rigid with others and reluctant to delegate
tasks out of fear they won’t do it right. The majority of social scientists believe that a
combination of social contextual factors and genetics
VI. ETIOLOGY determines an individual's personality and social conduct.
They think that environmental influences have the most
There are no conclusively established causes for impact. According to social scientists, the main elements
personality disorders, according to Whiteford HA, Ferrari determining personality and behavior are birth order,
AJ, Degenhardt L, Feigin V, Vos T. The global burden of parents, cultural environment, and heredity. The personality
mental, World Health Organization, Health WHODoM, of children is shaped by their parents. The growth of
Abuse S, Health WHODoM, Health SAM, Organization children can be influenced by the parent's age. The
WH, Evidence WHOMH, et al. Mental Health Atlas 2005. educational attainment, religious affiliation, occupation,
But there are a lot of established risk factors and potential economic standing, and cultural background of parents are
causes. Overall, research indicates that factors such as additional factors that might impact a child's social conduct
genetic predisposition and traumatic or abusive childhood and personality. (Indian j psychiatry , 2010)Culture has a
events are important in the development of personality strong influence on personality development. Culture has a
disorders, for example.Neglect and maltreatment of children big impact on how people form their personalities. The
are persistent risk factors for the emergence of personality fundamental personality types that exist in a civilization are
disorders in adults. (Hakkaart-van Roijen, Soeteman DI) determined by its cultural surroundings. Every culture
Another possible contributing factor to personality disorders produces a set of model personalities, or personality
has been considered to be socioeconomic position. qualities that are common to everyone in that
Personality disorder symptoms are strongly correlated with community.(Indian j psychiatry , 2010).
poor parental/neighborhood socioeconomic level. (Oxford
Textbook of Psychiatry, 2018). VIII. EPIDEMIOLOGY
Research indicates that parental personality problems Personality disorder is a relatively new notion, and not
may be the genesis of personality disorders. Because of this, much study has been done on it globally or in Afghanistan
the kid faces challenges of their own as an adult, including up to this point. Although the study in India takes a clinical
obstacles to completing their further education, finding form, I will discuss both global and Indian epidemiology in
employment, and establishing trustworthy relationships. this session.
There is currently a dearth of genetic studies to help
understand how personality problems emerge. Nonetheless, Before surveys began to be conducted in the 1990s, it
certain potential risk factors are still being investigated. was mainly unclear how common personality disorders were
(Quality of physical health care among patients with in the general population. A median incidence of 10.6% was
personality disorder) calculated in 2008 for diagnosable Parkinson's disease (PD)
based on six large studies conducted in three countries.
Attachment theory: "The basic tenet of attachment Mark F. Lenzenweger (2008).
research on human infants is that an infant with secure
attachment is one in which the parent responds to the According to a 2009 World Health Organization
infant's needs in a sensitive manner, while an infant with screening study conducted in 13 countries using DSM-IV
insecure attachment lacks such sensitive responding." criteria, personality disorders were estimated to affect 6.1%
of the population. The rate was occasionally influenced by
Throughout infancy and youth, insecure attachment socioeconomic and demographic characteristics, and co-
can cause issues with trust and emotional control. occurring mental problems contributed to the explanation of
Establishing and preserving wholesome connections over functional impairment.The prevalence of around one in ten
the course of a lifetime may be quite difficult. cases, particularly when linked to heavy cocaine use, is
deemed a serious public health issue that has to be addressed
by scientists and medical professionals.
IJISRT23NOV1396 www.ijisrt.com 2534
Volume 8, Issue 11, November 2023 International Journal of Innovative Science and Research Technology
ISSN No:-2456-2165
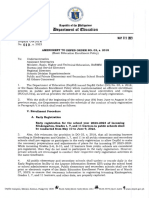
Fig. 1: Comparison by Country
In the US, the overall population prevalence of interviews with a subgroup of respondents. Co-occurring
personality disorders was estimated to be about 7.9% based mental illnesses (Axis I in the DSM) proved to be primarily
on screening data from the National Comorbidity Survey responsible for the functional handicap associated with the
Replication conducted between 2010 and 2013 and diagnosis.
Fig. 2: Personality Disorders Prevalent in American Adults
Indian Journal of Psychiatry (2010) reports that IX. PROBLEM STATEMENT
Chandrashekar, Reddy, and Chandrasekaran et al. performed
a meta-analysis of thirteen epidemiological studies from Personality disorder is a new concept in Afghanistan
various regions of India. Seven studies evaluated the and even the people are still not familiar with this disorder,
prevalence of personality disorders; the weighted prevalence so this topic is very important in Afghanistan to conduct
rate was 0.6%, and the rate ranged from 0 to 2.8%. In studies and research related to these disorders in order to
community research, there was a substantial correlation find a well-designed way to prevent these disorders. Also,
found between the diagnosis of personality disorder and standard guidelines should be established for treatment
male gender. personality disorder. On the other hand, not a single study
has been undertaken to date on personality disorder in
Prevalence rates ranging from 0.3 to 1.6% were found Afghanistan, especially in Kandahar, so it is a problem in
in early research on clinical samples from India (which did itself and creates a constraint for the current study.
not use operationalized criteria or diagnostic equipment).
Special demographics, such as college students (19.1%), X. TREATMENT MODALITIES
criminals (7.3–33.3%), patients with substance use problems
(20–55%), and patients who tried suicide (47.8–62.2%), had Psychotherapy
greater rates, however. Milieu therapy
Group therapy
IJISRT23NOV1396 www.ijisrt.com 2535
Volume 8, Issue 11, November 2023 International Journal of Innovative Science and Research Technology
ISSN No:-2456-2165
Cognitive/Behavioral Therapy Psychopharmacology The World Health Organization reported in 2009 a
prevalence estimates of around 6.1% for personality
XI. DISCUSSION disorders in the world.The National Comorbidity Survey,
indicated a population prevalence of around 7.9% for
The primary aim the study was to identify behaviors personality disorders in the U.S.A.
associated with personality disordersThrough the findings of
this research, we were able to fully identify any behavioral XIII. RECOMMENDATIONS
changes associated with personality disorderfor example
cluster A (solitariness, poor peer relationships, In Afghanistan obviously a need for better and more
underachievement in school and subject of teasing. studies in relation to personality disorders on methodology
Individual is seen as odd or eccentric) cluster B (High rates and epidemiology (particularly community studies), and also
of depression, substance abuse Sudden mood changes, on cultural and classificatory issues.
temper outbursts and feeling empty inside Extreme ups and
downs in relationships) cluster C (fear of criticism, Further research is required to fill in the wide gaps in
disapproval or rejection, depends on others to handle the field regarding the etiology, clinical features,
responsibilities such as finances, preoccupied with details, assessment, management, course, and outcome. It is also
lists, order, rules, organization or schedules, to the extent necessary to address the various debates that characterize
that the major point of the activity is lost). A secondary aim personality disorders, such as the validity of personality
was to know the prevalence of personality disorders.We disorders as currently defined, the distinctions between
were able to determine the prevalence of personality personality disorders and mental state disorders, and the
disorder worldwide thanks to the research's findings. categorization or dimension of personality disorders.
Actually, the goal was to determine the prevalence of
REFERENCES
personality disorders in Afghanistan and its surrounding
countries (Iran, Pakistan), but sadly, no single study has [1]. (n.d.). In M. S. Sanatinia R, Quality of physical health
been done about this topic. state the date Nevertheless, a care among patients with personality disorder.
World Health Organization screening study conducted in 13 [2]. (n.d.). In M. A. Narud K, Quality of life in patients
countries using DSM-IV criteria revealed in 2009 that the with personality disorders seen at an ordinary
prevalence of personality disorders was estimated to be psychiatric outpatient clinic.
about 6.1%. In the US, the overall population prevalence of [3]. 18 May 2013). In A. P. Association, Diagnostic and
personality disorders was estimated to be about 7.9% based Statistical Manual of Mental Disorders, 5th Edition:
on screening data from the National Comorbidity Survey DSM-5. Washington, DC American.
Replication conducted between 2010 and 2013 and [4]. (2008). In H.-v. R. Soeteman DI, The economic burden
interviews with a subgroup of respondents. The third aim of personality disorders in mental health care. J Clin
was to identify the risk factors of personality disorders Psychiatry.
globally.Through the findings of this research, we were able [5]. (2010). In C. e. al, Indian j psychiatry .(2018). In p. C.
to identify the risk factors of personality disorder in the Paul Harrsion, Oxford Textbook of Psychiatry.
world (genetic disposition and life experiences, such as New York, U.S.A: OXFORD University Press.
trauma and abuse, Socioeconomic status, Insecure [6]. How is a personality disorder treated? (n.d.). Retrieved
attachment in infancy, culture). The fourth aim was to from www.healthline.com:
distinguish the symptoms of different personality disorders. https://www.healthline.com/health/personality-
Through the findings of this research, we were able to disorders#diagnosis.
distinguish between the symptoms of all types of personality [7]. Personality disorders. (n.d.). Retrieved from
disorders. Through the findings of this research, we were www.mind.org.uk:
able to distinguish between the symptoms of all types of https://www.mind.org.uk/information-support/types-
personality disorders. The mention of the symptoms has of-mental-health-problems/personality-disorders/for-
been explained in the above pages, so examples and friends-family/
mentions are not necessary. [8]. Personality disorders are a group of a 10 mental health
conditions that involve long-lasting, disruptive patterns
XII. CONCLUSION
of thinking, behavior, mood and relating to others.
In Asia, particularly in Afghanistan, personality People with personality disorders often don’t realize
disorders are still in their infancy as a field. There is their thoughts and behaviors are pr. (n.d.). Retrieved
currently a stream of publications in India that are especially from my.clevelandclinic.org:
about personality disorder, compared to nearly none in the https://my.clevelandclinic.org/health/diseases/9636-
1980s. Still, it makes sense that the focus has been solely on personality-disorders-overview#symptoms-and-causes.
clinical epidemiology thus far. Despite the paucity of [9]. Type of personality disorder. (n.d.). Retrieved from
methodologically sound studies, the growing body of www.wikiwand.com:
knowledge in the discipline and its many methodological https://www.wikiwand.com/en/Personality_disorder
intricacies bodes well for the future. Genetic predisposition, [10]. www.psychiatry.org. (n.d.). Retrieved from Personality
trauma and abuse, and socioeconomic level are risk factors Disorders: https://www.psychiatry.org/patients-
for personality disorders. families/personality-disorders/what-are-personality-
disorders.
IJISRT23NOV1396 www.ijisrt.com 2536
You might also like
- Stuvia 1115751 Test Bank Varcarolis Foundations of Psychiatric Mental Health Nursing 8th Edition 1Document499 pagesStuvia 1115751 Test Bank Varcarolis Foundations of Psychiatric Mental Health Nursing 8th Edition 1Pesiflora100% (7)
- Mymaxicare Revised Brochure 2023Document15 pagesMymaxicare Revised Brochure 2023Engilbert MaqueraNo ratings yet
- MIDTERM Community Nursing 2Document24 pagesMIDTERM Community Nursing 2Will Garcia100% (2)
- Prometric Oman Sample MCQDocument10 pagesPrometric Oman Sample MCQibrahim 120% (1)
- Fundamentals of EpidemiologyDocument584 pagesFundamentals of EpidemiologyapoomamaNo ratings yet
- Biocibernetica y DolorDocument17 pagesBiocibernetica y DolorSarapzmNo ratings yet
- Personality Disorder 1: SeriesDocument10 pagesPersonality Disorder 1: SeriesJosé Ignacio SáezNo ratings yet
- Tyrer, Reed - Crawford - 2015Document10 pagesTyrer, Reed - Crawford - 2015Cynthia Barrios ArriagadaNo ratings yet
- Personality Disorder 1: SeriesDocument10 pagesPersonality Disorder 1: SeriesYasser AlghrafyNo ratings yet
- PersonalityDocument27 pagesPersonalityVineetha Valsa KumarNo ratings yet
- Dissociative Identity Disorder Research Paper TopicsDocument5 pagesDissociative Identity Disorder Research Paper TopicsqwgqavvhfNo ratings yet
- Inflexibility Processes As Predictors of Social Functioning in Chronic PsychosisDocument12 pagesInflexibility Processes As Predictors of Social Functioning in Chronic PsychosisifclarinNo ratings yet
- Chapter 14 &15Document73 pagesChapter 14 &15baconhaterNo ratings yet
- Autism. TL 2014Document15 pagesAutism. TL 2014jujucastellNo ratings yet
- Af Firming Gender Identity of Patients With Serious Mental IllnessDocument3 pagesAf Firming Gender Identity of Patients With Serious Mental IllnessdelandrethNo ratings yet
- Social Anxiety Disorder in Review: Two Decades of ProgressDocument20 pagesSocial Anxiety Disorder in Review: Two Decades of ProgressResidentes INPRFMNo ratings yet
- Depression Research PaperDocument8 pagesDepression Research Paperapi-312817381100% (1)
- AQUINOFAVIS FinalDraft DAYZERO PDFDocument37 pagesAQUINOFAVIS FinalDraft DAYZERO PDFTurtle WildNo ratings yet
- DepressionDocument5 pagesDepressionapi-356602462100% (1)
- 10 - ASD, Lord 2018Document53 pages10 - ASD, Lord 2018Grijisha ChandranNo ratings yet
- Mental Health Is Biological Health. Why Tackling Diseases of The Mind Is An Imperative For Biological Anthropology in The 21st CenturyDocument31 pagesMental Health Is Biological Health. Why Tackling Diseases of The Mind Is An Imperative For Biological Anthropology in The 21st CenturyWalter VillalobosNo ratings yet
- The Impact of Mental Illness Stigma PDFDocument34 pagesThe Impact of Mental Illness Stigma PDFJuan David SanzNo ratings yet
- Depression and Trauma A Transgenerational Psychoanalytic PerspectiveDocument20 pagesDepression and Trauma A Transgenerational Psychoanalytic PerspectiveAnonymous 18EBcIw2C100% (1)
- cpn-12-171 (171-179) PDFDocument9 pagescpn-12-171 (171-179) PDFRiski Wahyudi LasarikaNo ratings yet
- Literature Review of Effective Treatment For Dissociative Identity DisorderDocument7 pagesLiterature Review of Effective Treatment For Dissociative Identity Disorderc5t6h1q5No ratings yet
- Personality DisordersDocument5 pagesPersonality DisordersFabianNo ratings yet
- Research DossierDocument24 pagesResearch Dossierapi-300458195No ratings yet
- Suicide Prevention in Psychiatric PatientsDocument11 pagesSuicide Prevention in Psychiatric PatientsDaniela DiazNo ratings yet
- Intelligence and Personality As PredictorsDocument96 pagesIntelligence and Personality As PredictorsTrifan DamianNo ratings yet
- The Social Construction and Reframing of ADHDDocument13 pagesThe Social Construction and Reframing of ADHDJustin M.100% (1)
- Pyc1512 Unit 2Document21 pagesPyc1512 Unit 2maciabhenguNo ratings yet
- Vass 2015Document9 pagesVass 2015Amina LabiadhNo ratings yet
- Day 1 Intro RV Rushed Version For 2018Document30 pagesDay 1 Intro RV Rushed Version For 2018api-391411195No ratings yet
- The Antisocial Personality Disorder and Its Characteristics, Changes and Advances: A ChallengeDocument8 pagesThe Antisocial Personality Disorder and Its Characteristics, Changes and Advances: A ChallengeMerritaNo ratings yet
- An Overview of Autism Spectrum Disorder, Heterogeneity and Treatment OptionsDocument11 pagesAn Overview of Autism Spectrum Disorder, Heterogeneity and Treatment OptionsMaria Clara FeitosaNo ratings yet
- Themisconceptionsofmentalillness and Thestigmathatfollows Mini Ethnographyoriginaldraft2Document13 pagesThemisconceptionsofmentalillness and Thestigmathatfollows Mini Ethnographyoriginaldraft2api-437840816No ratings yet
- Paper 7Document31 pagesPaper 7DrAqeel AshrafNo ratings yet
- Jasminem Miniethno FinalversionDocument16 pagesJasminem Miniethno Finalversionapi-437840816No ratings yet
- Journal of Affective Disorders: Social Anxiety and Depression Stigma Among AdolescentsDocument10 pagesJournal of Affective Disorders: Social Anxiety and Depression Stigma Among AdolescentsPutri Indah PermataNo ratings yet
- JOURNAL CLUB NewDocument61 pagesJOURNAL CLUB Newaastha panthNo ratings yet
- The Lead-In : "List of People With Bipolar Disorder.")Document13 pagesThe Lead-In : "List of People With Bipolar Disorder.")api-321363387No ratings yet
- 1-Transidentities and Autism Spectrum Disorder A Systematic ReviewDocument14 pages1-Transidentities and Autism Spectrum Disorder A Systematic ReviewpietrovbhpNo ratings yet
- Chapter 22. SomatizationDocument14 pagesChapter 22. SomatizationDiego Francesco MacaliNo ratings yet
- An Overview of Autism Spectrum Disorder, Heterogeneity and Treatment OptionsDocument11 pagesAn Overview of Autism Spectrum Disorder, Heterogeneity and Treatment OptionsDiego CampillayNo ratings yet
- Psychopathology in Women: Incorporating Gender Perspective into Descriptive PsychopathologyFrom EverandPsychopathology in Women: Incorporating Gender Perspective into Descriptive PsychopathologyMargarita Sáenz-HerreroNo ratings yet
- Ansiedade SocialDocument12 pagesAnsiedade Socialvemec31798No ratings yet
- Ijpher: Research ArticleDocument9 pagesIjpher: Research ArticlePremier PublishersNo ratings yet
- Research Paper FinalDocument10 pagesResearch Paper Finalapi-300458195No ratings yet
- JAMWA Article - HopenwasserDocument24 pagesJAMWA Article - HopenwasserSex & Gender Women's Health CollaborativeNo ratings yet
- Mental Health Literacy and Anxiety Disorder PDFDocument11 pagesMental Health Literacy and Anxiety Disorder PDFShabrina Patriavy BennaradictaNo ratings yet
- Depression Taj Article 201116 Widdowson FinalDocument15 pagesDepression Taj Article 201116 Widdowson Finalvince yumulNo ratings yet
- Health Impact Framework - CollinsDocument12 pagesHealth Impact Framework - Collinsapi-355764752No ratings yet
- Mental Illness StigmaDocument27 pagesMental Illness StigmaAneehNo ratings yet
- Anthropology Research ReportDocument15 pagesAnthropology Research ReportSyeda Ramsha RizviNo ratings yet
- Livingwithschizophrenia KMDocument9 pagesLivingwithschizophrenia KMapi-285356333No ratings yet
- Demographic and Clinical Correlates of Suicidality in Adolescents Attending A Specialist Community Mental Health Service: A Naturalistic StudyDocument6 pagesDemographic and Clinical Correlates of Suicidality in Adolescents Attending A Specialist Community Mental Health Service: A Naturalistic StudyAna Paula Soares GondimNo ratings yet
- Final Research PaperDocument17 pagesFinal Research Paperapi-451460387No ratings yet
- Prac2 CpsirDocument30 pagesPrac2 CpsirSrishti GaurNo ratings yet
- HHS Public Access: Social Epidemiology of Depression and Anxiety by Gender IdentityDocument12 pagesHHS Public Access: Social Epidemiology of Depression and Anxiety by Gender Identitychoi yeontteomeokNo ratings yet
- Research Paper Topics Mental IllnessDocument5 pagesResearch Paper Topics Mental Illnessafmcueagg100% (1)
- Primer: Autism Spectrum DisorderDocument23 pagesPrimer: Autism Spectrum DisorderMakanudo.No ratings yet
- Final Honours Thesis-10Document23 pagesFinal Honours Thesis-10api-288362330No ratings yet
- Depression and Trauma - A Transgenerational Psychoanalytic PerspectiveDocument20 pagesDepression and Trauma - A Transgenerational Psychoanalytic PerspectiveCarlos DevotoNo ratings yet
- Final PaperDocument25 pagesFinal Paperapi-495169810No ratings yet
- Borderline Personality Disorder EssayDocument7 pagesBorderline Personality Disorder Essayapi-574298740No ratings yet
- Stress in AutismDocument38 pagesStress in Autismmatt lordNo ratings yet
- Design and Analysis of Various Formwork SystemsDocument6 pagesDesign and Analysis of Various Formwork SystemsInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Reintegration of Dairy in Daily American Diets: A Biochemical and Nutritional PerspectiveDocument1 pageReintegration of Dairy in Daily American Diets: A Biochemical and Nutritional PerspectiveInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Nurturing Corporate Employee Emotional Wellbeing, Time Management and the Influence on FamilyDocument8 pagesNurturing Corporate Employee Emotional Wellbeing, Time Management and the Influence on FamilyInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Occupational Injuries among Health Care Workers in Selected Hospitals in Ogbomosho, Oyo StateDocument6 pagesOccupational Injuries among Health Care Workers in Selected Hospitals in Ogbomosho, Oyo StateInternational Journal of Innovative Science and Research Technology100% (1)
- Appraisal of Nursing Care Received and it’s Satisfaction: A Case Study of Admitted Patients in Afe Babalola Multisystem Hospital, Ado Ekiti, Ekiti StateDocument12 pagesAppraisal of Nursing Care Received and it’s Satisfaction: A Case Study of Admitted Patients in Afe Babalola Multisystem Hospital, Ado Ekiti, Ekiti StateInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Evaluation of Lateral and Vertical Gingival Displacement Produced by Three Different Gingival Retraction Systems using Impression Scanning: An in-Vivo Original StudyDocument6 pagesEvaluation of Lateral and Vertical Gingival Displacement Produced by Three Different Gingival Retraction Systems using Impression Scanning: An in-Vivo Original StudyInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Salivary Diagnostics in Oral and Systemic Diseases - A ReviewDocument5 pagesSalivary Diagnostics in Oral and Systemic Diseases - A ReviewInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Prevalence of Microorganisms in UTI and Antibiotic Sensitivity Pattern among Gram Negative Isolates: A Cohort StudyDocument4 pagesPrevalence of Microorganisms in UTI and Antibiotic Sensitivity Pattern among Gram Negative Isolates: A Cohort StudyInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Biometric Security Systems Enhanced by AI: Exploring Concerns with AI Advancements in Facial Recognition and Other Biometric Systems have Security Implications and VulnerabilitiesDocument5 pagesBiometric Security Systems Enhanced by AI: Exploring Concerns with AI Advancements in Facial Recognition and Other Biometric Systems have Security Implications and VulnerabilitiesInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- MSMEs and Rural Prosperity: A Study of their Influence in Indonesian Agriculture and Rural EconomyDocument6 pagesMSMEs and Rural Prosperity: A Study of their Influence in Indonesian Agriculture and Rural EconomyInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Shift from Traditional to Modern Building Concepts and Designs in Ringim Town: A Comparative Study of Aesthetics, Values, Functions and DurabilityDocument9 pagesShift from Traditional to Modern Building Concepts and Designs in Ringim Town: A Comparative Study of Aesthetics, Values, Functions and DurabilityInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Fuzzy based Tie-Line and LFC of a Two-Area Interconnected SystemDocument6 pagesFuzzy based Tie-Line and LFC of a Two-Area Interconnected SystemInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- An Explanatory Sequential Study of Public Elementary School Teachers on Deped Computerization Program (DCP)Document7 pagesAn Explanatory Sequential Study of Public Elementary School Teachers on Deped Computerization Program (DCP)International Journal of Innovative Science and Research TechnologyNo ratings yet
- Dynamic Analysis of High-Rise Buildings for Various Irregularities with and without Floating ColumnDocument3 pagesDynamic Analysis of High-Rise Buildings for Various Irregularities with and without Floating ColumnInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- AI Robots in Various SectorDocument3 pagesAI Robots in Various SectorInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Intrusion Detection and Prevention Systems for Ad-Hoc NetworksDocument8 pagesIntrusion Detection and Prevention Systems for Ad-Hoc NetworksInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Geotechnical Assessment of Selected Lateritic Soils in Southwest Nigeria for Road Construction and Development of Artificial Neural Network Mathematical Based Model for Prediction of the California Bearing RatioDocument10 pagesGeotechnical Assessment of Selected Lateritic Soils in Southwest Nigeria for Road Construction and Development of Artificial Neural Network Mathematical Based Model for Prediction of the California Bearing RatioInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- The Effects of Liquid Density and Impeller Size with Volute Clearance on the Performance of Radial Blade Centrifugal Pumps: An Experimental ApproachDocument16 pagesThe Effects of Liquid Density and Impeller Size with Volute Clearance on the Performance of Radial Blade Centrifugal Pumps: An Experimental ApproachInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- A Novel Approach to Template Filling with Automatic Speech Recognition for Healthcare ProfessionalsDocument6 pagesA Novel Approach to Template Filling with Automatic Speech Recognition for Healthcare ProfessionalsInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Innovative Mathematical Insights through Artificial Intelligence (AI): Analysing Ramanujan Series and the Relationship between e and π\piDocument8 pagesInnovative Mathematical Insights through Artificial Intelligence (AI): Analysing Ramanujan Series and the Relationship between e and π\piInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Integration of Information Communication Technology, Strategic Leadership and Academic Performance in Universities in North Kivu, Democratic Republic of CongoDocument7 pagesIntegration of Information Communication Technology, Strategic Leadership and Academic Performance in Universities in North Kivu, Democratic Republic of CongoInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Importance of Early Intervention of Traumatic Cataract in ChildrenDocument5 pagesImportance of Early Intervention of Traumatic Cataract in ChildrenInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Comparison of JavaScript Frontend Frameworks - Angular, React, and VueDocument8 pagesComparison of JavaScript Frontend Frameworks - Angular, React, and VueInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Diode Laser Therapy for Drug Induced Gingival Enlaregement: A CaseReportDocument4 pagesDiode Laser Therapy for Drug Induced Gingival Enlaregement: A CaseReportInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Organizational Factors That Influence Information Security in Smes: A Case Study of Mogadishu, SomaliaDocument10 pagesOrganizational Factors That Influence Information Security in Smes: A Case Study of Mogadishu, SomaliaInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Breaking Down Barriers To Inclusion: Stories of Grade Four Teachers in Maintream ClassroomsDocument14 pagesBreaking Down Barriers To Inclusion: Stories of Grade Four Teachers in Maintream ClassroomsInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Occupational Safety: PPE Use and Hazard Experiences Among Welders in Valencia City, BukidnonDocument11 pagesOccupational Safety: PPE Use and Hazard Experiences Among Welders in Valencia City, BukidnonInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Analysis of Factors Obstacling Construction Work in The Tojo Una-Una Islands RegionDocument9 pagesAnalysis of Factors Obstacling Construction Work in The Tojo Una-Una Islands RegionInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- The Influence of Artificial Intelligence On Employment Trends in The United States (US)Document5 pagesThe Influence of Artificial Intelligence On Employment Trends in The United States (US)International Journal of Innovative Science and Research TechnologyNo ratings yet
- Disseminating The Real-World Importance of Conjunct Studies of Acculturation, Transculturation, and Deculturation Processes: Why This Can Be A Useful Technique To Analyze Real-World ObservationsDocument15 pagesDisseminating The Real-World Importance of Conjunct Studies of Acculturation, Transculturation, and Deculturation Processes: Why This Can Be A Useful Technique To Analyze Real-World ObservationsInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Environmental Health-A Branch of Public Second StrategyDocument7 pagesEnvironmental Health-A Branch of Public Second StrategyhelloaNo ratings yet
- Hospital Guide Better Being ThailandDocument7 pagesHospital Guide Better Being ThailandNenad PavlovićNo ratings yet
- Scientific Research Journal of India SRJI Vol-3 Issue-3 Year 2014Document209 pagesScientific Research Journal of India SRJI Vol-3 Issue-3 Year 2014Dr. Krishna N. SharmaNo ratings yet
- The Fountain of Youth? The Quest For Aging TherapiesDocument5 pagesThe Fountain of Youth? The Quest For Aging TherapiesRichaRd MetcalfeNo ratings yet
- Natural History of DiseaseDocument9 pagesNatural History of DiseaseAan Sucitra Hollan Fm'sNo ratings yet
- Materi Sistem ImunDocument23 pagesMateri Sistem ImunsahabatrumahsakitNo ratings yet
- Childhood Obesity in The Rio Grande ValleyDocument6 pagesChildhood Obesity in The Rio Grande ValleydjwickedNo ratings yet
- Ec Creating Energy CirclesDocument10 pagesEc Creating Energy CirclesRadhika Goel100% (1)
- English For Physiotherapists - Angielski Dla FizjoterapiiDocument112 pagesEnglish For Physiotherapists - Angielski Dla FizjoterapiiSabina RuszkowskaNo ratings yet
- USHC ReviewDocument119 pagesUSHC ReviewArman DhillonNo ratings yet
- KCR Full 10-11-17Document20 pagesKCR Full 10-11-17Ryan CronkNo ratings yet
- Global Health and Scientific Research (Flory, 2004)Document30 pagesGlobal Health and Scientific Research (Flory, 2004)Faz RahmanNo ratings yet
- 4th Quarter Pointers To ReviewDocument1 page4th Quarter Pointers To Review박소민No ratings yet
- ASC Code of Ethics Updated 2010Document28 pagesASC Code of Ethics Updated 2010Ganch Aguas50% (2)
- Micro MicrobiotaDocument7 pagesMicro MicrobiotaJustinNo ratings yet
- TE Chapter 1Document45 pagesTE Chapter 1tooba khanNo ratings yet
- OPD Form IhealthcareDocument2 pagesOPD Form IhealthcareSanjay PatilNo ratings yet
- Disability Studies and The Academy-Past, Present, and FutureDocument10 pagesDisability Studies and The Academy-Past, Present, and FutureMicahNo ratings yet
- Vaccine Development, From The Lab To The Clinic (Jim Tartaglia)Document14 pagesVaccine Development, From The Lab To The Clinic (Jim Tartaglia)National Press FoundationNo ratings yet
- DO 010 s.2023Document4 pagesDO 010 s.2023Gladys BiscochoNo ratings yet
- Case Management Assessment FormDocument13 pagesCase Management Assessment FormDiksha PadamNo ratings yet
- Homeopathy Questionnaire 2Document30 pagesHomeopathy Questionnaire 2SanjeevNo ratings yet
- We Are Like Co WifesDocument9 pagesWe Are Like Co WifesTricianne Merielle S. Bano-oyNo ratings yet
- Endosulfan Tragedy in Kasaragod - Did It Really Happen?Document18 pagesEndosulfan Tragedy in Kasaragod - Did It Really Happen?K.m.SreekumarNo ratings yet