Download as xls, pdf, or txt
You might also like
- Basic Course in Biomedical Research Q-Bank (CYCLE 1-5) : by - Dr.N.G.Pradeep Kumar Bangalore Medical CollegeDocument211 pagesBasic Course in Biomedical Research Q-Bank (CYCLE 1-5) : by - Dr.N.G.Pradeep Kumar Bangalore Medical Collegekesav sudabattula100% (1)
- Database Design Project Solution: Oracle Baseball League Store DatabaseDocument3 pagesDatabase Design Project Solution: Oracle Baseball League Store DatabaseListi emi100% (1)
- 20 ĐỀ THI THỬ TỐT NGHIỆP THPT NĂM 2021 MÔN TIẾNG ANH BÁM SÁT VÀ PHÁT TRIỂN ĐỀ MINH HỌA CỦA BỘ GD&ĐT CÓ ĐÁP ÁNDocument161 pages20 ĐỀ THI THỬ TỐT NGHIỆP THPT NĂM 2021 MÔN TIẾNG ANH BÁM SÁT VÀ PHÁT TRIỂN ĐỀ MINH HỌA CỦA BỘ GD&ĐT CÓ ĐÁP ÁNPhung Thuy71% (7)
- Editable Retail Loan Application - ApplicantDocument10 pagesEditable Retail Loan Application - Applicantmadhukar sahayNo ratings yet
- Civil Plan SetDocument24 pagesCivil Plan SetSinclair Broadcast Group - EugeneNo ratings yet
- HEMP-005 Excavation Manual & Mechanical Rev.2Document9 pagesHEMP-005 Excavation Manual & Mechanical Rev.2saravana.bNo ratings yet
- Application For EHS Induction and Gate Pass ID - Rev1Document3 pagesApplication For EHS Induction and Gate Pass ID - Rev1Imran KhuraishiNo ratings yet
- U.S. Nonresident Alien Income Tax Return: Filing StatusDocument2 pagesU.S. Nonresident Alien Income Tax Return: Filing StatustonywolfaceveNo ratings yet
- 2021revised PYSPESO 11 BTEC Form B Skills Registry System Rev 01Document1 page2021revised PYSPESO 11 BTEC Form B Skills Registry System Rev 01Janna AlardeNo ratings yet
- Tenant Info SheetDocument1 pageTenant Info Sheetnddeguzman.kcsNo ratings yet
- RegisterDocument5 pagesRegisterashutoshthakur100No ratings yet
- ApplicationFromat 29Document2 pagesApplicationFromat 29s.sanfia404No ratings yet
- BIMA BBS RegisterDocument47 pagesBIMA BBS Registeraminamin.200029No ratings yet
- PEMI Account Update FormDocument1 pagePEMI Account Update FormJun GomezNo ratings yet
- APTB VisaMasterCard 130721 0ec5ef2c 48fc 4ce8 A523 43c802f141d2Document3 pagesAPTB VisaMasterCard 130721 0ec5ef2c 48fc 4ce8 A523 43c802f141d2thanaptttNo ratings yet
- CBC - Converter - HDMF 1.3 - 2020Document4 pagesCBC - Converter - HDMF 1.3 - 2020joshuamathewgonzalesNo ratings yet
- Disbursement VoucherDocument2 pagesDisbursement VoucherCeasar Ryan AsuncionNo ratings yet
- Annex 10 - Accreditation Assessors FormsDocument10 pagesAnnex 10 - Accreditation Assessors FormsKen FerrolinoNo ratings yet
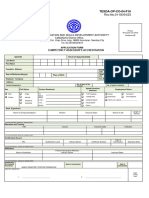
- TESDA-OP-CO-04 - Accreditation - Assessors FormsDocument4 pagesTESDA-OP-CO-04 - Accreditation - Assessors FormsLoralee BragatNo ratings yet
- Know Your Client (KYC) Application Form (For Non-Individuals Only)Document2 pagesKnow Your Client (KYC) Application Form (For Non-Individuals Only)rajatmaheshwariNo ratings yet
- Form ADocument2 pagesForm APrateek BaruahNo ratings yet
- KYC Non IndividualDocument2 pagesKYC Non Individualapi-3849142No ratings yet
- SBMA ID Card Infosheet (RENEWAL)Document1 pageSBMA ID Card Infosheet (RENEWAL)Renan Roque100% (1)
- Final Retirement Pay Calculator Tinainmanila - Com 4Document2 pagesFinal Retirement Pay Calculator Tinainmanila - Com 4Martin SandersonNo ratings yet
- TESDA OP CO 04 Accreditation Assessors FormsDocument10 pagesTESDA OP CO 04 Accreditation Assessors FormsAnonymous hb0K4oqNo ratings yet
- Kutei BasinDocument9 pagesKutei BasinAdina Dwi LathifaNo ratings yet
- Online Application - KVS 2014 PDFDocument3 pagesOnline Application - KVS 2014 PDFashwaniNo ratings yet
- Attendance Register Cum PayslipDocument51 pagesAttendance Register Cum PayslipProfessional PartnerzNo ratings yet
- Registration Form Oct-Nov 2020Document1 pageRegistration Form Oct-Nov 2020Anita SetyaNo ratings yet
- CBC - Converter - HDMF 1.7 - CONTRI MP2Document3 pagesCBC - Converter - HDMF 1.7 - CONTRI MP2CICOSAT COLLEGES INC.No ratings yet
- What Makes You Happy: ©2015 Nyali Peder Etholm-Idsoe ChartDocument2 pagesWhat Makes You Happy: ©2015 Nyali Peder Etholm-Idsoe ChartYuvash VaidyaNo ratings yet
- Income Tax Calculator 2018-2019Document1 pageIncome Tax Calculator 2018-2019Muhammad Hanif SuchwaniNo ratings yet
- (Overseas Trained Applicants) Registration/ Registration Certificate/ Practising Licence ApplicationDocument2 pages(Overseas Trained Applicants) Registration/ Registration Certificate/ Practising Licence ApplicationJohan VargasNo ratings yet
- Pemi Additional FormDocument1 pagePemi Additional FormJun GomezNo ratings yet
- Wages Code Form IV Employee RegisterDocument1 pageWages Code Form IV Employee RegisterAsma SethiNo ratings yet
- 5025 ITP Precast Panel InstallationDocument8 pages5025 ITP Precast Panel InstallationdjzaiyuanyeNo ratings yet
- DFo 4 1 ProjectDocument3 pagesDFo 4 1 Projectjilekj.ita20No ratings yet
- Price Quotation Form: Technical Education & Skills Development AuthorityDocument1 pagePrice Quotation Form: Technical Education & Skills Development AuthorityKarl Juma JaclaNo ratings yet
- 港人免費申請加拿大開放工作簽證!如何做學歷認證、費用及需時? JobsDB Hong KongDocument1 page港人免費申請加拿大開放工作簽證!如何做學歷認證、費用及需時? JobsDB Hong Kongstephanie siuNo ratings yet
- TSMS Musthyala L4 Practical ManjulaDocument5 pagesTSMS Musthyala L4 Practical ManjulamodernhospitaldubaggaNo ratings yet
- BPTS Offboarding Checklist v2023.Document6 pagesBPTS Offboarding Checklist v2023.Samantha DomingoNo ratings yet
- Marquez Bryan TDocument1 pageMarquez Bryan TMae Ann LacbayoNo ratings yet
- HDFC Common Application FormDocument3 pagesHDFC Common Application FormTirthGanatraNo ratings yet
- Miscellaneous Visa Fee Form Im41Document1 pageMiscellaneous Visa Fee Form Im41sandykaruppaiahNo ratings yet
- Estate AccountDocument15 pagesEstate AccountVasishtha Teeluckdharry100% (2)
- Contributions Payment Form: Social Security SystemDocument6 pagesContributions Payment Form: Social Security SystemRemy Rose Planta MagnoNo ratings yet
- Attendance FormDocument1 pageAttendance Formaida syehiraNo ratings yet
- Instruction For Trust Account: Aristocapital New Account ContactDocument11 pagesInstruction For Trust Account: Aristocapital New Account ContactАлександр ЛебедевNo ratings yet
- Sole / First Applicant Second Applicant Third ApplicantDocument2 pagesSole / First Applicant Second Applicant Third ApplicantAnkur KaushikNo ratings yet
- Non Individual KYCDocument2 pagesNon Individual KYCapi-3833582No ratings yet
- Nde Personel FormDocument1 pageNde Personel Formrizki projectNo ratings yet
- CIF Opening Form I 02082018Document4 pagesCIF Opening Form I 02082018GAYATHRINo ratings yet
- A-BD-11-Project LOGDocument1 pageA-BD-11-Project LOGIrfan BiradarNo ratings yet
- New CCFormsDocument2 pagesNew CCFormsSouvik BanerjeeNo ratings yet
- Application Form For Registration of Professional DevelopersDocument11 pagesApplication Form For Registration of Professional DevelopersDINESH100% (5)
- Carpentry NC Ii Request For QuotationDocument1 pageCarpentry NC Ii Request For QuotationKhael Angelo Zheus JaclaNo ratings yet
- Revised PYSPESO 10 BTEC Form A BTEC Monthly Report Rev 01 2021-1-1Document1 pageRevised PYSPESO 10 BTEC Form A BTEC Monthly Report Rev 01 2021-1-1Janna AlardeNo ratings yet
- Updated Assessors' Application FormDocument1 pageUpdated Assessors' Application FormLieza MarianoNo ratings yet
- Job Application Form: Page 2 of 2Document2 pagesJob Application Form: Page 2 of 2Salmaan RaafiQqNo ratings yet
- New Combined ESIC PF ChallanDocument1 pageNew Combined ESIC PF Challansagar_rajputNo ratings yet
- Vitiligo Iranian TreatmentDocument3 pagesVitiligo Iranian Treatmentsawaira khanNo ratings yet
- Case Study: Attention Deficit Hyperactivity Disorder (ADHD) : I. Executive SummaryDocument5 pagesCase Study: Attention Deficit Hyperactivity Disorder (ADHD) : I. Executive SummaryJenipe CodiumNo ratings yet
- Human Karyotyping Lab #: Name: Date of Lab: Lab Partner/s: Due Date of LabDocument9 pagesHuman Karyotyping Lab #: Name: Date of Lab: Lab Partner/s: Due Date of LabLouella ArtatesNo ratings yet
- NCP Acute PainDocument2 pagesNCP Acute PainMillicent Faye G. Gelit50% (2)
- Artificial Intelligence in Medicine: Virginie Felizardo, Nuno M. Garcia, Nuno Pombo, Imen MegdicheDocument15 pagesArtificial Intelligence in Medicine: Virginie Felizardo, Nuno M. Garcia, Nuno Pombo, Imen MegdicheShujian ZhaoNo ratings yet
- Clinical ExperienceDocument2 pagesClinical Experienceapi-509074425No ratings yet
- The Social Media Amidst The PandemicDocument22 pagesThe Social Media Amidst The PandemicHans Jedh Carlos J. AnzuresNo ratings yet
- PranithaDocument15 pagesPranithaKumar VijayNo ratings yet
- Portrayal of Psychopathy in The MoviesDocument7 pagesPortrayal of Psychopathy in The MoviesAshish ChandNo ratings yet
- Wrist Joint Special TestDocument38 pagesWrist Joint Special Testcamy bhagatNo ratings yet
- Safety Data Sheet Acetylene, Solvent FreeDocument14 pagesSafety Data Sheet Acetylene, Solvent FreeGEINER ANDRES OSSA GALVIS100% (1)
- 2003 Jarup Hazards of Heavy Metal ContaminationDocument16 pages2003 Jarup Hazards of Heavy Metal ContaminationTiago Silva AroucheNo ratings yet
- Basic First AidDocument16 pagesBasic First AidDanica DolorNo ratings yet
- Week 1: Community Health Nursing (RLE) Midterm PeriodDocument13 pagesWeek 1: Community Health Nursing (RLE) Midterm PeriodAndrea AputenNo ratings yet
- Case Study Ufc FPDocument11 pagesCase Study Ufc FPMicah MagallanoNo ratings yet
- Improving Skills in Correcting Astigmastism (Dr. Putri Hartini, Sp. M.)Document33 pagesImproving Skills in Correcting Astigmastism (Dr. Putri Hartini, Sp. M.)Nisaa DwityarahmaNo ratings yet
- C1. Proficiency Template From Anglia ExaminationsDocument12 pagesC1. Proficiency Template From Anglia ExaminationsMarcos ChiappiniNo ratings yet
- ACOG Opinion On IAIDocument13 pagesACOG Opinion On IAIGladys GarciaNo ratings yet
- PTSD Test PDFDocument8 pagesPTSD Test PDFLady A MontgomeryNo ratings yet
- Lapkas Hymen ImperforataDocument27 pagesLapkas Hymen ImperforataKhairida Hafni LbsNo ratings yet
- The Holistic Cancer SolutionDocument10 pagesThe Holistic Cancer SolutionromalfioNo ratings yet
- 17n. Premarital SexDocument23 pages17n. Premarital SexFileScanNo ratings yet
- Pcrs Handbook For PharmacistsDocument100 pagesPcrs Handbook For Pharmacistsapmcintyre69No ratings yet
- Genetic Engineering ResearchDocument4 pagesGenetic Engineering Researchapi-668534088No ratings yet
- 480-Article Text-4010-1-10-20201031Document8 pages480-Article Text-4010-1-10-20201031Rini FebriantiNo ratings yet
- Geeta's Guide To Woman's Yoga PracticeDocument376 pagesGeeta's Guide To Woman's Yoga PracticePatrícia Franchi de FreitasNo ratings yet
- LN Inspire Broch - Filtered - z021918Document6 pagesLN Inspire Broch - Filtered - z021918benjaminNo ratings yet