
Download as pdf or txt
You might also like
- Nutrition Now 8th Edition Ebook PDFDocument41 pagesNutrition Now 8th Edition Ebook PDFvickie.neal389100% (46)
- Walker Pediatric Gastrointestinal Disease PDFDocument2,226 pagesWalker Pediatric Gastrointestinal Disease PDFMagaly Cornejo100% (1)
- Biochemistry of The GIT S1-10Document3 pagesBiochemistry of The GIT S1-10Kim RamosNo ratings yet
- BiochemistryDocument82 pagesBiochemistryAmritzz Paul83% (6)
- Biochem GitDocument54 pagesBiochem Gitmilerasmr881No ratings yet
- PDF Digestion and Absorption of Carbohydrate and ProteinDocument5 pagesPDF Digestion and Absorption of Carbohydrate and ProteinHhh HhhNo ratings yet
- UntitledDocument2 pagesUntitledTheresaNo ratings yet
- LOMER Et Al-2008-Alimentary Pharmacology & Therapeutics PDFDocument11 pagesLOMER Et Al-2008-Alimentary Pharmacology & Therapeutics PDFM SNo ratings yet
- GlycolysisDocument51 pagesGlycolysisKazar ProbusNo ratings yet
- Module 7Document17 pagesModule 7Shitty PieNo ratings yet
- Carbohydrate MetabolismDocument8 pagesCarbohydrate MetabolismKyle Andre De GraciaNo ratings yet
- Biochemistry CARBOHYDRATESDocument5 pagesBiochemistry CARBOHYDRATESPrincess M. De VeraNo ratings yet
- PBPN TOPIC3 CHOMETABOLISM APRILSEM 2019 StudentDocument120 pagesPBPN TOPIC3 CHOMETABOLISM APRILSEM 2019 StudentRaysonChooNo ratings yet
- 10 Cell MetabolismDocument11 pages10 Cell Metabolismecon finaNo ratings yet
- Glycogen Metabolism Index CardDocument3 pagesGlycogen Metabolism Index CardspringdingNo ratings yet
- GalactosemiaDocument6 pagesGalactosemiaakbar alituNo ratings yet
- Carbohydrate Metabolism Chandel 2021Document16 pagesCarbohydrate Metabolism Chandel 2021Luis C Ribon VNo ratings yet
- Metabolic Pathways of GlucoseDocument11 pagesMetabolic Pathways of GlucosemanikchawlaplusoneNo ratings yet
- MBG312 Chp22Document51 pagesMBG312 Chp22Baran KirdarNo ratings yet
- Carbohydrate Biosynthesis: Carbohydrate Biosynthesis:: Gluconeogenesis: The Universal Pathway For Synthesis of GlucoseDocument9 pagesCarbohydrate Biosynthesis: Carbohydrate Biosynthesis:: Gluconeogenesis: The Universal Pathway For Synthesis of GlucoseM Ziyad UlhaqNo ratings yet
- Biomedical Importance Glycolysis Can Function Under Anaerobic ConditionsDocument5 pagesBiomedical Importance Glycolysis Can Function Under Anaerobic ConditionsCatalina Denise Blaquera FloresNo ratings yet
- ObjectivesDocument19 pagesObjectivesAnirudh ShankarNo ratings yet
- Lectures 4,5,6,7 BiochemistryDocument4 pagesLectures 4,5,6,7 Biochemistryمحمد امينNo ratings yet
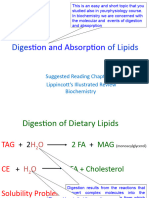
- Digestion and Absorption of Lipids 2020Document11 pagesDigestion and Absorption of Lipids 2020HaalaNo ratings yet
- GlycolysisDocument7 pagesGlycolysismoneth gerarmanNo ratings yet
- Cshperspect MBM A040568Document15 pagesCshperspect MBM A040568adhiningsihNo ratings yet
- (Biochem B) Overview of Metabolism-Viliran (Cheezus)Document10 pages(Biochem B) Overview of Metabolism-Viliran (Cheezus)bero beroNo ratings yet
- Chapter 19 - Gluconeogenesis & Amp The Control of Blood GlucoseDocument14 pagesChapter 19 - Gluconeogenesis & Amp The Control of Blood Glucoserenzo041199No ratings yet
- Carbohydrate Metabolism Presentation.Document27 pagesCarbohydrate Metabolism Presentation.ViragNo ratings yet
- Carbohydrate MetabolismDocument12 pagesCarbohydrate Metabolismbingbong2231No ratings yet
- Cold Spring Harb Perspect Biol-2021-Chandel-a040568Document16 pagesCold Spring Harb Perspect Biol-2021-Chandel-a040568Carissa satya NingtyasNo ratings yet
- BiologyDocument28 pagesBiologyleslieofori257No ratings yet
- Mtap421 CarbohydratesDocument4 pagesMtap421 CarbohydratesNhelomar ManlinconNo ratings yet
- Metabolic Adaptation During Prolonged StarvationDocument18 pagesMetabolic Adaptation During Prolonged StarvationThabrish rish1234No ratings yet
- LGIS CarbohyrateDocument30 pagesLGIS Carbohyratehasaanmushtaq98765No ratings yet
- (NOTES) Carbohydrates MetabolismDocument13 pages(NOTES) Carbohydrates MetabolismGabrielle SerranoNo ratings yet
- GLM Biochemistry of GastroenterologyDocument14 pagesGLM Biochemistry of GastroenterologyEaint BoNo ratings yet
- Interaccion Proteinas y ChosDocument5 pagesInteraccion Proteinas y ChosLuis Daniel Rodríguez EsquedaNo ratings yet
- Sinteza Si Depozitarea Carbohdratilor in Muschi Si FicatDocument17 pagesSinteza Si Depozitarea Carbohdratilor in Muschi Si FicatAnonymous UnVea6TnNo ratings yet
- Metabolic Pathways of GlucoseDocument31 pagesMetabolic Pathways of GlucoseLisandrea BrownNo ratings yet
- Mind Maps in Biochemistry - (Metabolism of Carbohydrates)Document23 pagesMind Maps in Biochemistry - (Metabolism of Carbohydrates)Gus LionsNo ratings yet
- Biochemistry of GITDocument108 pagesBiochemistry of GITgaserhany3No ratings yet
- BIOCHEM-Lipid Metabolism 1Document12 pagesBIOCHEM-Lipid Metabolism 1Std Dlshsi100% (1)
- Digestion Absorption 12 2019Document14 pagesDigestion Absorption 12 2019Karyan ShinNo ratings yet
- Cap 8 Appleton Homeostasis de GlucosaDocument14 pagesCap 8 Appleton Homeostasis de GlucosaMariandré OlmedoNo ratings yet
- Digestion BiochemDocument6 pagesDigestion Biochemmoneth gerarmanNo ratings yet
- Unit 2: Biological Molecules General Biology 1 1 Quarter: 1. Carbohydrates and LipidsDocument5 pagesUnit 2: Biological Molecules General Biology 1 1 Quarter: 1. Carbohydrates and LipidsSophia AbatayNo ratings yet
- GluconeogenesisDocument3 pagesGluconeogenesisClairyssa Myn D CaballeroNo ratings yet
- Disorder of The Body MassDocument2 pagesDisorder of The Body Massdwi yuniariNo ratings yet
- Carb Reference - CornellDocument2 pagesCarb Reference - CornellNIDHI DESAINo ratings yet
- Carbohydrate (Cho) Metabolism Glycolysis: A. 6-Carbon Stage (Energy-Consuming Stage)Document5 pagesCarbohydrate (Cho) Metabolism Glycolysis: A. 6-Carbon Stage (Energy-Consuming Stage)Andrea JosonNo ratings yet
- Carbohydrate DigestionDocument12 pagesCarbohydrate DigestionayeshaNo ratings yet
- Biochemistry - 2.08 - Gluconeogenesis and Blood Glucose ControlDocument9 pagesBiochemistry - 2.08 - Gluconeogenesis and Blood Glucose ControlJonathan Decena Jr.No ratings yet
- Glucose-6-Phosphate Is Also Known As A Central Metabolite Because It Can Enter A Lot of PathwaysDocument10 pagesGlucose-6-Phosphate Is Also Known As A Central Metabolite Because It Can Enter A Lot of PathwaysNica Lopez FernandezNo ratings yet
- Biochemistry M3 Pidlaoan AlexanderDocument5 pagesBiochemistry M3 Pidlaoan AlexanderPrincess M. De VeraNo ratings yet
- Metabolisme Karbohidrat: By: Dina Rahma FadlilahDocument22 pagesMetabolisme Karbohidrat: By: Dina Rahma FadlilahRIZKA FITRIANDINI 2020No ratings yet
- 14 - GluconeogenesisDocument6 pages14 - Gluconeogenesisashfaq ahmedNo ratings yet
- Gluconeogenesis PDFDocument8 pagesGluconeogenesis PDFBilly McleanNo ratings yet
- Digestion of C, P & LDocument12 pagesDigestion of C, P & LEba DadoughNo ratings yet
- Module 2.2 CarbohydratesDocument6 pagesModule 2.2 CarbohydratesZabelle BungarNo ratings yet
- Hepatobiliary TransDocument14 pagesHepatobiliary TransEricson CandelariaNo ratings yet
- Biochemistry Applied to the Brewing Processes - Fermentation and the Finished BeerFrom EverandBiochemistry Applied to the Brewing Processes - Fermentation and the Finished BeerRating: 5 out of 5 stars5/5 (1)
- I PUC/Class-XI/Jr - Inter NEET-Botany Vol-IIDocument28 pagesI PUC/Class-XI/Jr - Inter NEET-Botany Vol-IIMayuri chatpalliwarNo ratings yet
- University of Cambridge International Examinations General Certificate of Education Ordinary LevelDocument16 pagesUniversity of Cambridge International Examinations General Certificate of Education Ordinary LevelNOVASTAR222No ratings yet
- Experiment No. 2 CarbohydratesDocument5 pagesExperiment No. 2 CarbohydratesZheldinan Nicole CruzNo ratings yet
- Guidelines To R3337 Food Labeling Regulations Draft 1685509864Document109 pagesGuidelines To R3337 Food Labeling Regulations Draft 1685509864Cosmic Moon BabyNo ratings yet
- NCP Imbalanced Nutrition Less Than Body RequirementsDocument5 pagesNCP Imbalanced Nutrition Less Than Body Requirementsrusnani100% (1)
- Biochemistry Clinical Pathology Sample Paper by NoteskartsDocument6 pagesBiochemistry Clinical Pathology Sample Paper by Noteskartsarshu98172No ratings yet
- Zhu Et, Al. 2010Document9 pagesZhu Et, Al. 2010Yohannes AynieNo ratings yet
- KMU Foundation ModuleDocument20 pagesKMU Foundation ModuleShafiq Ur RahmanNo ratings yet
- Chem Investigatory ProjectDocument13 pagesChem Investigatory ProjectLolaa M HNo ratings yet
- Health Secrets-NEW9Document119 pagesHealth Secrets-NEW9Win CruzNo ratings yet
- 9chemistry Investigatory Project by Prakhar To Shivam On CarbohydrateDocument17 pages9chemistry Investigatory Project by Prakhar To Shivam On CarbohydratePRAKHAR SRIVASTAVANo ratings yet
- 3.1 Classes of FoodDocument28 pages3.1 Classes of FoodSERENE TEE ERN HUI MoeNo ratings yet
- Concept Paper About Health and NutritionDocument4 pagesConcept Paper About Health and NutritionLyka RebualosNo ratings yet
- 2 Biochemistry CarbohydratesDocument29 pages2 Biochemistry CarbohydratesKelvin ChipezeniNo ratings yet
- Simple and Complex CarbohydratesDocument78 pagesSimple and Complex CarbohydratesRonald GyezahoNo ratings yet
- Men Fat Loss Supplements GuideDocument6 pagesMen Fat Loss Supplements GuideMarcel Bejan0% (1)
- Stew Smith Lean Down Meal Options PDFDocument20 pagesStew Smith Lean Down Meal Options PDFCorey Mays67% (3)
- Effect of Concentration of Sargassum Polycystum and Fermentation Time On Thickness and Yield of Nata de SargassumDocument5 pagesEffect of Concentration of Sargassum Polycystum and Fermentation Time On Thickness and Yield of Nata de SargassumMamta AgarwalNo ratings yet
- Questions 1-25 PDFDocument6 pagesQuestions 1-25 PDFLuthfia PramikaNo ratings yet
- Manish Narayan Dhar Shivalika Singh: Luiza GharibyanDocument42 pagesManish Narayan Dhar Shivalika Singh: Luiza GharibyanSachi LakhyaniNo ratings yet
- Metabolism Nutrition Part 1 Crash Course AP 36Document8 pagesMetabolism Nutrition Part 1 Crash Course AP 36hwasawereNo ratings yet
- Module 3 BiomoleculesDocument30 pagesModule 3 BiomoleculesAlaine Paul GeronimoNo ratings yet
- Punjab Boards 11th Class Biology Book English Medium 6368073082448619590 PDFDocument455 pagesPunjab Boards 11th Class Biology Book English Medium 6368073082448619590 PDFNnc Saud KhanNo ratings yet
- Bio MoleculesDocument58 pagesBio MoleculesVetti VilladolidNo ratings yet
- Experiment 3 and 4 Carbohydrates PDFDocument3 pagesExperiment 3 and 4 Carbohydrates PDFIcey YoonNo ratings yet
- BeyondChemo WorkBookDocument42 pagesBeyondChemo WorkBookgreentree14No ratings yet
- [Forum of Nutrition_Bibliotheca Nutritio Et Dieta] Ibrahim Elmadfa - Diet Diversification and Health Promotion_ European Academy of Nutritional Sciences (EANS) Conference, Vienna, May 14-15, 2004 (2005, S. Karger AG (Switzerland)) - LiDocument183 pages[Forum of Nutrition_Bibliotheca Nutritio Et Dieta] Ibrahim Elmadfa - Diet Diversification and Health Promotion_ European Academy of Nutritional Sciences (EANS) Conference, Vienna, May 14-15, 2004 (2005, S. Karger AG (Switzerland)) - LiMarcosChamorroTrujilloNo ratings yet
- Osazone Test PDFDocument10 pagesOsazone Test PDFreddyNo ratings yet





















































































![[Forum of Nutrition_Bibliotheca Nutritio Et Dieta] Ibrahim Elmadfa - Diet Diversification and Health Promotion_ European Academy of Nutritional Sciences (EANS) Conference, Vienna, May 14-15, 2004 (2005, S. Karger AG (Switzerland)) - Li](https://imgv2-2-f.scribdassets.com/img/document/512520381/149x198/bb5e78426f/1624246064?v=1)
