Download as pdf or txt
You might also like
- Maxillofacial Prosthodontics CourseDocument98 pagesMaxillofacial Prosthodontics CourseFBI LUC1FeR80% (10)
- Peat 1Document42 pagesPeat 1Steve Colbert100% (3)
- Management Febrile NeutropeniaDocument21 pagesManagement Febrile NeutropeniaJayanthi Mandasari NasutionNo ratings yet
- Wound Closure ManualDocument125 pagesWound Closure Manualtotaleclipse0202100% (1)
- ICON 2016 Febrile Neutropenia GuidelinesDocument34 pagesICON 2016 Febrile Neutropenia GuidelinesTor Ja100% (1)
- Case Study Neonatal SepsisDocument21 pagesCase Study Neonatal SepsisLenjun0% (1)
- Laporan Jaga Murai 26 Nov, 29 Nov, 2 DesDocument9 pagesLaporan Jaga Murai 26 Nov, 29 Nov, 2 DesAnonymous K2ddMg0miNo ratings yet
- Braz Jr. Infect Dis 2021Document4 pagesBraz Jr. Infect Dis 2021cdsaludNo ratings yet
- TuberculosisDocument5 pagesTuberculosislittlecandiesNo ratings yet
- Vincent J 2020Document11 pagesVincent J 2020Kala PatharNo ratings yet
- Autoantibodies in Autoimmune Rheumatic DiseaseDocument6 pagesAutoantibodies in Autoimmune Rheumatic DiseaseVictor Roman LazarteNo ratings yet
- Budd ChiariDocument10 pagesBudd ChiariJuan Carlos Reyes BozaNo ratings yet
- Elevated Cytomegalovirus and Epstein-Barr Virus BuDocument5 pagesElevated Cytomegalovirus and Epstein-Barr Virus BuMostafa SalahNo ratings yet
- Water Er 2011Document5 pagesWater Er 2011Jaya Semara PutraNo ratings yet
- Evaluation of Viral Load in Patients With Ebola VIDocument10 pagesEvaluation of Viral Load in Patients With Ebola VISeanNo ratings yet
- Diagnostic Testing and Interpretation of Tests ForDocument10 pagesDiagnostic Testing and Interpretation of Tests ForPuri RahmawatiNo ratings yet
- The University Texas Health Science Center at Sun Antonio RangeDocument3 pagesThe University Texas Health Science Center at Sun Antonio Rangesaadsffggeettrgbfbfbftggrg ergrtertererefrerrNo ratings yet
- Basic Problems of Serological Laboratory DiagnosisDocument37 pagesBasic Problems of Serological Laboratory DiagnosisSuzan MatarNo ratings yet
- BM 2.3 Bambang SudarmantoDocument46 pagesBM 2.3 Bambang SudarmantoAbdullah ShiddiqNo ratings yet
- Idsa GuidelinesDocument34 pagesIdsa GuidelinesROSEN NNo ratings yet
- PCR y PCTDocument12 pagesPCR y PCTRicardo PazNo ratings yet
- IDSA Nec FascDocument34 pagesIDSA Nec FascShameen KhanNo ratings yet
- 12 OA Evaluation of Febrile Thrombocytopenia CasesDocument5 pages12 OA Evaluation of Febrile Thrombocytopenia CasesVimal NishadNo ratings yet
- Meningitis PDFDocument8 pagesMeningitis PDFrizeviNo ratings yet
- Ability of Procalcitonin To Predict Bacterial MeningitisDocument20 pagesAbility of Procalcitonin To Predict Bacterial MeningitisGeorge WinchesterNo ratings yet
- Simon 2004Document12 pagesSimon 2004mr_curiousityNo ratings yet
- Wood-2016-Cytometry Part B: Clinical CytometryDocument7 pagesWood-2016-Cytometry Part B: Clinical CytometryWalter Jhon Delgadillo AroneNo ratings yet
- Case Studies: Recurrent Fever, Chills, and Malaise in A 53-Year-Old ManDocument2 pagesCase Studies: Recurrent Fever, Chills, and Malaise in A 53-Year-Old Mansreeja maragoniNo ratings yet
- 46-Year-Old Man With Fevers, Chills, and PancytopeniaDocument4 pages46-Year-Old Man With Fevers, Chills, and PancytopeniaDr Manoranjan MNo ratings yet
- Daftar Pustaka No 6Document11 pagesDaftar Pustaka No 6Efti WeaslyNo ratings yet
- Clase 23. Neutropenia FebrilDocument17 pagesClase 23. Neutropenia FebriljuanpbagurNo ratings yet
- Pi Is 1083879118313909Document2 pagesPi Is 1083879118313909Ljc JaslinNo ratings yet
- Viral Exanthems: An Update On Laboratory Testing of The Adult PatientDocument14 pagesViral Exanthems: An Update On Laboratory Testing of The Adult PatientEinjel PearlNo ratings yet
- JMM 70 286Document5 pagesJMM 70 286ธรรมธรรศ นิลธรNo ratings yet
- Efficacy and Safety of Ceftazidime/avibactam: A Systematic Review and Meta-AnalysisDocument9 pagesEfficacy and Safety of Ceftazidime/avibactam: A Systematic Review and Meta-AnalysisNattawat TeerawattanapongNo ratings yet
- Monografia MeningitisDocument4 pagesMonografia MeningitisJulian GomezNo ratings yet
- Practice Guidelines For The Diagnosis and Management of Skin and Soft-Tissue InfectionsDocument34 pagesPractice Guidelines For The Diagnosis and Management of Skin and Soft-Tissue InfectionsNatalia MoranNo ratings yet
- CHAPTER-17 NUERO MergedDocument17 pagesCHAPTER-17 NUERO MergedRyn ShadowNo ratings yet
- Consideration of Some Other Specific Indications: BacteremiaDocument18 pagesConsideration of Some Other Specific Indications: BacteremiaMOHAMMAD JOFA RACHMAN PUTERANo ratings yet
- CMV A Troll in ICUDocument11 pagesCMV A Troll in ICUMajd ShakerNo ratings yet
- Labo en A. ComplicadaDocument7 pagesLabo en A. ComplicadaMiluska Torrico CanoNo ratings yet
- Work-Upforfeverduring Neutropeniaforboththe Stemcelltransplantrecipient Andthehematologicmalignancy PatientDocument17 pagesWork-Upforfeverduring Neutropeniaforboththe Stemcelltransplantrecipient Andthehematologicmalignancy PatiententannabilakasdyNo ratings yet
- Serum Procalcitonin and C-Reactive Protein Levels As Markers of Bacterial Infection: A Systematic Review and Meta-AnalysisDocument12 pagesSerum Procalcitonin and C-Reactive Protein Levels As Markers of Bacterial Infection: A Systematic Review and Meta-AnalysissyahputriNo ratings yet
- Clinical Diagnostic Testing For Human CytomegalovirusDocument12 pagesClinical Diagnostic Testing For Human Cytomegalovirusdossantoselaine212No ratings yet
- tmpD1AB TMPDocument9 pagestmpD1AB TMPFrontiersNo ratings yet
- Int J Lab Hematology - 2023 - Adir - The Role of Blood Inflammatory Markers in The Preoperative Diagnosis of AcuteDocument5 pagesInt J Lab Hematology - 2023 - Adir - The Role of Blood Inflammatory Markers in The Preoperative Diagnosis of AcuteOncología CdsNo ratings yet
- Journal 8Document7 pagesJournal 8margareth silaenNo ratings yet
- Procalcitonin Levels in Surgical Patients at Risk of CandidemiaDocument6 pagesProcalcitonin Levels in Surgical Patients at Risk of CandidemiaKeziaNo ratings yet
- Caso 6Document6 pagesCaso 6Valeria Yamilet Piedra RomeroNo ratings yet
- Corrected Lucidchart Week17 18 Group2 Cluster2Document15 pagesCorrected Lucidchart Week17 18 Group2 Cluster2Roan-Lhieyne Sagli Diad VenancioNo ratings yet
- Best Practice & Research Clinical Obstetrics and GynaecologyDocument14 pagesBest Practice & Research Clinical Obstetrics and GynaecologySaúl Alberto Kohan BocNo ratings yet
- Sepsis 1Document17 pagesSepsis 1lizzie clavijoNo ratings yet
- 1113-Article Text-3878-1-10-20220623Document5 pages1113-Article Text-3878-1-10-20220623sadiq. aljabha.2014No ratings yet
- 25 KarlisDocument3 pages25 KarlisFaisal JamshedNo ratings yet
- EASL Clinical Practice Guidelines: Vascular Diseases of The Liver Q PDFDocument24 pagesEASL Clinical Practice Guidelines: Vascular Diseases of The Liver Q PDFMihaela PăvăleanNo ratings yet
- Artrite ReumatoideDocument14 pagesArtrite ReumatoideAndreNo ratings yet
- Yield of Blood Cultures in Children Presenting With Febrile Illness in A Tertiary Care HospitalDocument5 pagesYield of Blood Cultures in Children Presenting With Febrile Illness in A Tertiary Care Hospitalfaraz.mirza1No ratings yet
- Bmjopen 2017 019611Document8 pagesBmjopen 2017 019611Anonymous K2ddMg0miNo ratings yet
- Febrile NeutropeniaDocument43 pagesFebrile NeutropeniaKirr DiNo ratings yet
- Neutropenia KankerDocument7 pagesNeutropenia Kankeranisa rachmitaNo ratings yet
- Plateletcrit: A Possible Biomarker of Inflammation in Hepatitis A InfectionDocument4 pagesPlateletcrit: A Possible Biomarker of Inflammation in Hepatitis A InfectionAbdul Rahman Al IdrisNo ratings yet
- Baker Et Al. - 2022 - Acute Hepatitis and Adenovirus Infection Among ChiDocument3 pagesBaker Et Al. - 2022 - Acute Hepatitis and Adenovirus Infection Among ChiCaleb HeNo ratings yet
- Daftar PustakaDocument4 pagesDaftar PustakaSantalia SeramNo ratings yet
- Gastric CáncerDocument206 pagesGastric CáncerjorgehogNo ratings yet
- Journal of Dermatology ResearchDocument5 pagesJournal of Dermatology ResearchAthenaeum Scientific PublishersNo ratings yet
- Identification of Candida Sp. Fungus in The Water of Toilet Tube at Tour Places at Kediri With Centrifugation MethodDocument10 pagesIdentification of Candida Sp. Fungus in The Water of Toilet Tube at Tour Places at Kediri With Centrifugation MethodMeysifa NNo ratings yet
- Mha 101Document4 pagesMha 101NIHUGBH KOLKATANo ratings yet
- Pathway LeukemiaDocument2 pagesPathway LeukemiaAmbar RahmanNo ratings yet
- Cepheid GeneXpert System Menu Flyer CE IVD 0293 EnglishDocument2 pagesCepheid GeneXpert System Menu Flyer CE IVD 0293 EnglishTchouala DentrishNo ratings yet
- Hypertensive Cardiovascular DiseaseDocument2 pagesHypertensive Cardiovascular DiseaseYna AcerdenNo ratings yet
- Breast Cancer Staging PDFDocument12 pagesBreast Cancer Staging PDFDanu BagoesNo ratings yet
- Maternal Quiz NotesDocument79 pagesMaternal Quiz NotesPasay Trisha Faye Y.No ratings yet
- Mri Request FormDocument2 pagesMri Request Formraad_alghamdi_1No ratings yet
- Anusha Article IJIRMFDocument5 pagesAnusha Article IJIRMFAnusha SampathNo ratings yet
- Essentialsof Practical Panchakarma TherapyDocument10 pagesEssentialsof Practical Panchakarma TherapyravibasarihalliNo ratings yet
- 'OET' SAMPLE READING NEW DR TANJIM OVEE 2020Document19 pages'OET' SAMPLE READING NEW DR TANJIM OVEE 2020AHMED TANJIMUL ISLAMNo ratings yet
- Delirium in Older Adults in Associated With Development of New DementiaDocument11 pagesDelirium in Older Adults in Associated With Development of New DementiaIrvin MarcelNo ratings yet
- Suctioning ProcedureDocument42 pagesSuctioning ProcedureAkshata Bansode100% (4)
- 111 144 2 PB PDFDocument9 pages111 144 2 PB PDFAnisa SeptianaNo ratings yet
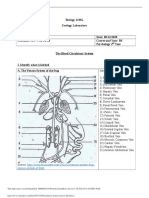
- Circulatory System Answer SheetDocument4 pagesCirculatory System Answer SheetMarlie TobiseNo ratings yet
- For Normal Findings and For Abnormal FindingsDocument4 pagesFor Normal Findings and For Abnormal FindingsNicaericka ReyesNo ratings yet
- Nephrotic Syndrom WardDocument49 pagesNephrotic Syndrom WardHelene AlawamiNo ratings yet
- Sleep Wake DisordersDocument68 pagesSleep Wake DisordersRashed ShatnawiNo ratings yet
- Prevention - DressingDocument10 pagesPrevention - DressingDaniel OctavianusNo ratings yet
- Your Pulse and Your Target Heart RateDocument3 pagesYour Pulse and Your Target Heart RateKhaled Bin SalamNo ratings yet
- Malignant Soft Tissue TumorsDocument21 pagesMalignant Soft Tissue TumorsEva GustianiNo ratings yet
- No. 3 - June 2018 - A Second Special Issue On EMDR in PTSD and Other Psychopathological ConditionsDocument2 pagesNo. 3 - June 2018 - A Second Special Issue On EMDR in PTSD and Other Psychopathological ConditionsYolanda BallesterosNo ratings yet
- IMMUNIZATION LecDocument77 pagesIMMUNIZATION LecKavya ReddyNo ratings yet
- ConcussionDocument6 pagesConcussionradziah_mohdNo ratings yet