Download as pdf or txt
You might also like
- Report For Experiment #7 Work and Energy On An Air Track: Meghan LumnahDocument13 pagesReport For Experiment #7 Work and Energy On An Air Track: Meghan LumnahMuhammad Usman MalikNo ratings yet
- UEENEEI157A+Inotech Controls+Handbook - V2 - 3Document142 pagesUEENEEI157A+Inotech Controls+Handbook - V2 - 3Kim N Lewis100% (3)
- Susan David - The Gift and Power of Emotional Courage - TED TalkDocument11 pagesSusan David - The Gift and Power of Emotional Courage - TED TalkFlorentina SuduNo ratings yet
- Pinto pm2 Ism ch10Document40 pagesPinto pm2 Ism ch10Jesha Carl JotojotNo ratings yet
- Excel Formulas & FunctionsDocument74 pagesExcel Formulas & FunctionsStefos Pepes100% (1)
- Cable Profile For Prestressing and Calculation of Eccentricities of Substiture CableDocument4 pagesCable Profile For Prestressing and Calculation of Eccentricities of Substiture Cablerabindra choudhary0% (1)
- Test Name: Determination of Tensile Properties of Geotextile Using Wide Strip ScopeDocument3 pagesTest Name: Determination of Tensile Properties of Geotextile Using Wide Strip ScopeSwapan PaulNo ratings yet
- Simple PendulumDocument13 pagesSimple Pendulumthelmamusonda60No ratings yet
- BS-5467 1Document2 pagesBS-5467 1Yazhar MuhammedNo ratings yet
- Report Test Tensile GP 11Document24 pagesReport Test Tensile GP 11syabaniah khipliNo ratings yet
- Objectives:: What Does Resistance Depend On?Document4 pagesObjectives:: What Does Resistance Depend On?Rodrigo TavarezNo ratings yet
- Least-Squares Estimation Using Lagrange Multipliers: Home Search Collections Journals About Contact Us My IopscienceDocument2 pagesLeast-Squares Estimation Using Lagrange Multipliers: Home Search Collections Journals About Contact Us My Iopsciencenauji_kNo ratings yet
- Diffraction GratingDocument8 pagesDiffraction GratingClintDoesMusicNo ratings yet
- 110.2.final ExerciseDocument2 pages110.2.final Exercise李欣純No ratings yet
- Certificate of Analysis: National Institute of Standards & TechnologyDocument7 pagesCertificate of Analysis: National Institute of Standards & TechnologyCesar BarretoNo ratings yet
- 35321Document10 pages35321Hany ShoushaNo ratings yet
- Member Name: P1: 1. General InformationDocument6 pagesMember Name: P1: 1. General Informationvijay kumar yadavNo ratings yet
- Air PropertyDocument1 pageAir PropertyDawit WaleNo ratings yet
- CineonDocument25 pagesCineonzcreamNo ratings yet
- Dos 772 Service Learning Journal II EmployerDocument5 pagesDos 772 Service Learning Journal II Employerapi-530270156No ratings yet
- BCS-CRM 161 - 4 Sep2015Document2 pagesBCS-CRM 161 - 4 Sep2015Ishmael WoolooNo ratings yet
- BCS-CRM 113 Mar2014Document3 pagesBCS-CRM 113 Mar2014Ishmael WoolooNo ratings yet
- Specific Heat Capacities of AirDocument13 pagesSpecific Heat Capacities of AirNguyen ChuyenNo ratings yet
- Experiment 4 OrificeDocument17 pagesExperiment 4 OrificeAnis Nurfarahanim Abdul HalimNo ratings yet
- SS-CRM No. 493/3 High Manganese Steel: Certificate of AnalysisDocument2 pagesSS-CRM No. 493/3 High Manganese Steel: Certificate of Analysislehdruk7100No ratings yet
- Generic TST Protocol Distributed Annexes KNCVDocument14 pagesGeneric TST Protocol Distributed Annexes KNCVtheresiaNo ratings yet
- Delsa™ Nano: (D) (NM) (P.I.) (D) (CM /sec)Document2 pagesDelsa™ Nano: (D) (NM) (P.I.) (D) (CM /sec)Rahmah IdrisNo ratings yet
- Copy of Mektan 13Document40 pagesCopy of Mektan 13M AminudinNo ratings yet
- ° C Kpa X 0.005 M X 0.058 M X 0.109 M: Results and Data AnalysisDocument18 pages° C Kpa X 0.005 M X 0.058 M X 0.109 M: Results and Data AnalysisjojoNo ratings yet
- 10m Unipole - Sungai AbongDocument26 pages10m Unipole - Sungai Abongatokku50% (2)
- Structural Design of Mo-P-Dr2Document35 pagesStructural Design of Mo-P-Dr2sudhirkumarsharma1966No ratings yet
- CH31007 Mechanical Operations MA 2016Document2 pagesCH31007 Mechanical Operations MA 2016Nitin MauryaNo ratings yet
- Lucrare ASTR 2017Document9 pagesLucrare ASTR 2017Gillich Gilbert-RainerNo ratings yet
- Practical Considerations For Conductivity and Total Dissolved Solids MeasurementDocument5 pagesPractical Considerations For Conductivity and Total Dissolved Solids MeasurementVarun KumarNo ratings yet
- Fabry PEROT Interferometer by Pankaj YadavDocument16 pagesFabry PEROT Interferometer by Pankaj YadavPankaj YadavNo ratings yet
- SL-T - Sanarya DashtiDocument16 pagesSL-T - Sanarya DashtiPRATEEK SHARMANo ratings yet
- Truss MetalDocument9 pagesTruss MetalRia SusantiNo ratings yet
- Supplementary Material For Pressure-Dependent Transport Characteristic of Methane Gas in Slit NanoporesDocument7 pagesSupplementary Material For Pressure-Dependent Transport Characteristic of Methane Gas in Slit NanoporessaeedNo ratings yet
- Lecture 2 - ME460 Renewable Energy ResourcesDocument125 pagesLecture 2 - ME460 Renewable Energy ResourcessaadNo ratings yet
- Jac M6SF-3-1Document2 pagesJac M6SF-3-1lorens moraNo ratings yet
- GeoVES - V1 VES SoftwareDocument5 pagesGeoVES - V1 VES SoftwareAurangzeb JadoonNo ratings yet
- Geology LabDocument7 pagesGeology LabAtubrah PrinceNo ratings yet
- SCRM No. 666/12 Ductile (Nodular) Iron: L Certificate of AnalysisDocument2 pagesSCRM No. 666/12 Ductile (Nodular) Iron: L Certificate of AnalysisPeterson SudlabNo ratings yet
- Job 4 SDocument4 pagesJob 4 SShah zaib UmerNo ratings yet
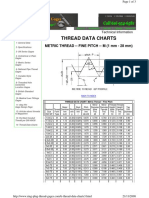
- Thread Data Charts: Metric Thread - Fine Pitch - M (1 MM - 28 MM)Document3 pagesThread Data Charts: Metric Thread - Fine Pitch - M (1 MM - 28 MM)BetoBluesNo ratings yet
- Topic 5 PAVEMENT DESIGNDocument71 pagesTopic 5 PAVEMENT DESIGNChin Tiong LeeNo ratings yet
- A Decision Tree Model For Accurate Prediction of Sand Erosion inDocument15 pagesA Decision Tree Model For Accurate Prediction of Sand Erosion ink.zaripova.hNo ratings yet
- Tensile Testing of Metals Lab ReportDocument8 pagesTensile Testing of Metals Lab ReportEmıły Wınıfred100% (1)
- Kelessidis and Mpandelis (2004) : N) P S 3 3 DDocument1 pageKelessidis and Mpandelis (2004) : N) P S 3 3 DDiane de OcampoNo ratings yet
- Harmonic #: A1 A2 A3 A4 DC Amplitude PhaseDocument3 pagesHarmonic #: A1 A2 A3 A4 DC Amplitude PhaseZokiNo ratings yet
- Surface Roughness Value ConversionsDocument2 pagesSurface Roughness Value Conversionsnick10686No ratings yet
- UCS Tanah HarbinDocument2 pagesUCS Tanah HarbinHarbin SimbolonNo ratings yet
- Tugas Besar Banjir RencanaDocument9 pagesTugas Besar Banjir RencanaMahardikaNo ratings yet
- Hydrothermal Alteration Map Fron Lansat-8 DataDocument12 pagesHydrothermal Alteration Map Fron Lansat-8 DataDavid PradaNo ratings yet
- ET 310 Lab 4Document19 pagesET 310 Lab 4DylanNo ratings yet
- 1995Document13 pages1995Cheuk Yin NGNo ratings yet
- China-US Workshop' 2009, Changzhou, Jiangshu, China, 091017Document15 pagesChina-US Workshop' 2009, Changzhou, Jiangshu, China, 091017Materials Research InstituteNo ratings yet
- PETR 3134 Codes and Specifications in The Petroleum IndustryDocument18 pagesPETR 3134 Codes and Specifications in The Petroleum IndustrynuvanNo ratings yet
- Consolidation PDFDocument113 pagesConsolidation PDFalnisNo ratings yet
- Physics Student Experiment: ABRAHAM, Aneeta (Aabra64) Year 11 PhysicsDocument14 pagesPhysics Student Experiment: ABRAHAM, Aneeta (Aabra64) Year 11 PhysicsAneeta ann abrahamNo ratings yet
- HY8Report - ALCANTARILLA TRIPLE 1.5Document8 pagesHY8Report - ALCANTARILLA TRIPLE 1.5IVAN ANDRES VELANDIA ACEVEDONo ratings yet
- Aster: User's GuideDocument20 pagesAster: User's GuideosamazpNo ratings yet
- Fundamentals of Oral and Maxillofacial RadiologyFrom EverandFundamentals of Oral and Maxillofacial RadiologyRating: 4 out of 5 stars4/5 (1)
- Infertility: DR Somsubhra deDocument32 pagesInfertility: DR Somsubhra deInspirasi Hidupku100% (1)
- Acc Area-03Document5 pagesAcc Area-03Zj FerrerNo ratings yet
- Troubleshooting For Rb433R3, Rb433Ur2: No Power, Blue Led Isn'T LitDocument7 pagesTroubleshooting For Rb433R3, Rb433Ur2: No Power, Blue Led Isn'T LitJoseAugustoOsteicoechea100% (1)
- Chapter 10 (Epjj)Document59 pagesChapter 10 (Epjj)syuhadaNo ratings yet
- Methodology in The New MillenniumDocument15 pagesMethodology in The New Millenniumerzsebetkacso67% (3)
- Steam Air Ejector Performance and Its Dimensional ParametersDocument296 pagesSteam Air Ejector Performance and Its Dimensional ParametersGuru Raja Ragavendran NagarajanNo ratings yet
- Working Memory Model of Memory QuestionsDocument26 pagesWorking Memory Model of Memory QuestionssophiaNo ratings yet
- Worlds Beyond Our Ice Wall Isoa4Document10 pagesWorlds Beyond Our Ice Wall Isoa4hujankopiairNo ratings yet
- Read The Following Passage and Mark The Letter A, B, C or D On Your Answer The Correct Answer To Each of The Following QuestionsDocument16 pagesRead The Following Passage and Mark The Letter A, B, C or D On Your Answer The Correct Answer To Each of The Following QuestionsGVTrần Thị Phương ThảoNo ratings yet
- 2300 SIGE 2016 FinalDocument6 pages2300 SIGE 2016 FinalCarlos JuniorNo ratings yet
- Department of Electronics and Communication Engineering: Subject: Vlsi Signal ProcessingDocument8 pagesDepartment of Electronics and Communication Engineering: Subject: Vlsi Signal ProcessingRaja PirianNo ratings yet
- This Is A Book For Survivors of Unspeakable Loss - The Suicide of A Loved OneDocument13 pagesThis Is A Book For Survivors of Unspeakable Loss - The Suicide of A Loved OnenatasaknezNo ratings yet
- Digital Bangladesh PresentationDocument16 pagesDigital Bangladesh PresentationMd. Zahid HossainNo ratings yet
- BUET Undergraduate Admission Test 2019-2020: Department Allocation (6th Run) of Admitted Candidates (Engineering & URP)Document20 pagesBUET Undergraduate Admission Test 2019-2020: Department Allocation (6th Run) of Admitted Candidates (Engineering & URP)AnasNo ratings yet
- Design of Sequential Circuits - Example 1.3Document3 pagesDesign of Sequential Circuits - Example 1.3MD Saifuzzaman SohanNo ratings yet
- Kao LC - Portafolio de ProductosDocument2 pagesKao LC - Portafolio de ProductosBadri Rached100% (1)
- Revised Syllabus B.arch R 2021Document108 pagesRevised Syllabus B.arch R 2021MANIMEGALAI PRASANNANo ratings yet
- Latest Earliest CitiesDocument3 pagesLatest Earliest CitiesnasrideviNo ratings yet
- Algebra 2005Document40 pagesAlgebra 2005Yb Andik Adi CahyonoNo ratings yet
- The Difference Between Sports and GamesDocument3 pagesThe Difference Between Sports and GamesKrishan Kumar DattaNo ratings yet
- Wizard S AideDocument58 pagesWizard S AideKnightsbridge~No ratings yet
- Antenna RFI MonitoringDocument71 pagesAntenna RFI MonitoringmoannaNo ratings yet
- Neurological Development From Birth To Six YearsDocument143 pagesNeurological Development From Birth To Six YearsWaleska SakibNo ratings yet
- A Letter To God (1) Flow ChartDocument13 pagesA Letter To God (1) Flow Chartsudharoy2008No ratings yet
- Rural Marketing: Opportunities, Challenges & StrategiesDocument4 pagesRural Marketing: Opportunities, Challenges & StrategiesRajaRajeswari.LNo ratings yet
- Shift Report - November 25, 2023-2nd ShiftDocument4 pagesShift Report - November 25, 2023-2nd Shiftbobowapthree19No ratings yet