Download as pdf or txt
You might also like
- ACE Personal Training Manual 4th EditionDocument47 pagesACE Personal Training Manual 4th EditionJoão Pinheiro60% (15)
- Study Guide NREMTDocument4 pagesStudy Guide NREMTdebbiemedic355740% (5)
- Care Enhancement Qualities of Health Workers in Community SettingDocument3 pagesCare Enhancement Qualities of Health Workers in Community SettingJon Eric74% (19)
- Clinical Teaching PlanDocument12 pagesClinical Teaching PlanEden Natividad100% (3)
- Nihms 1688237Document20 pagesNihms 1688237Mohammed KhalidNo ratings yet
- Nutritional Status As Cancer Diagnosis PredictorDocument13 pagesNutritional Status As Cancer Diagnosis Predictornutri.analuxavierNo ratings yet
- Ans 92 1638Document6 pagesAns 92 1638Mohammed KhalidNo ratings yet
- Lung Cancer - 2021Document20 pagesLung Cancer - 2021Gilbert LazarusNo ratings yet
- Diabetes Mellitus and Pyogenic Liver Abscess: Risk and PrognosisDocument8 pagesDiabetes Mellitus and Pyogenic Liver Abscess: Risk and PrognosisJeanetteNo ratings yet
- 2019 Article 701Document6 pages2019 Article 701Mohammed KhalidNo ratings yet
- Bestpracticesin Surveillanceforbarrett'S Esophagus: Joseph R. Triggs,, Gary W. FalkDocument17 pagesBestpracticesin Surveillanceforbarrett'S Esophagus: Joseph R. Triggs,, Gary W. FalkduranaxelNo ratings yet
- Risk Factors For Early Onset Colorectal CancerDocument17 pagesRisk Factors For Early Onset Colorectal Cancerbarbara liuva chia policarpoNo ratings yet
- 2016 Article 2832Document11 pages2016 Article 2832nimaelhajjiNo ratings yet
- Manejo de Neoplasia Intraepitelial AnalDocument10 pagesManejo de Neoplasia Intraepitelial AnalLibertad DíazNo ratings yet
- Interval Colorectal Cancers in Inflammatory Bowel Disease: The Grim Statistics and True StoriesDocument12 pagesInterval Colorectal Cancers in Inflammatory Bowel Disease: The Grim Statistics and True StoriespancholarpancholarNo ratings yet
- MEHU130 U2 T74 Colorectal CancerDocument14 pagesMEHU130 U2 T74 Colorectal CancerStefani AtlleNo ratings yet
- Beta-Blocker Drug Use and Survival Among Patients With Pancreatic AdenocarcinomaDocument9 pagesBeta-Blocker Drug Use and Survival Among Patients With Pancreatic AdenocarcinomaHao LiuNo ratings yet
- Ca EndometriumDocument51 pagesCa Endometriumoktaviany810No ratings yet
- Association Between Diabetes Mellitus and TBDocument15 pagesAssociation Between Diabetes Mellitus and TBMade NujitaNo ratings yet
- Guidelines For Prevention of NSAID-Related Ulcer ComplicationsDocument11 pagesGuidelines For Prevention of NSAID-Related Ulcer ComplicationsPeet UpNo ratings yet
- Role of Bacterial Infections in Pancreatic Cancer: ReviewDocument5 pagesRole of Bacterial Infections in Pancreatic Cancer: ReviewZilbran BerontaxNo ratings yet
- Kuipers 2015Document25 pagesKuipers 2015Fahmi RizalNo ratings yet
- INFLAMMATORY Breast CancerDocument20 pagesINFLAMMATORY Breast CancerbencleeseNo ratings yet
- Ax1 BSP FinalDocument18 pagesAx1 BSP FinalSofia Krylova-SmithNo ratings yet
- Increased Risk of Microscopic Colitis With Use of Proton Pump Inhibitors and Non-Steroidal Anti-In Ammatory DrugsDocument11 pagesIncreased Risk of Microscopic Colitis With Use of Proton Pump Inhibitors and Non-Steroidal Anti-In Ammatory DrugsFabrizzio BardalesNo ratings yet
- International Incidence and Mortality Trends of Liver Cancer: A Global ProfileDocument9 pagesInternational Incidence and Mortality Trends of Liver Cancer: A Global ProfileNovita ApramadhaNo ratings yet
- Narrative Review SampleDocument10 pagesNarrative Review SampleSvt Mscofficial2No ratings yet
- Shifts in The Proportion of Colorectal CancerDocument8 pagesShifts in The Proportion of Colorectal CancerprimaNo ratings yet
- Crohn's DiseaseDocument15 pagesCrohn's DiseaseManuel alexanderNo ratings yet
- Prognostic JournalDocument6 pagesPrognostic JournalElpida WNo ratings yet
- Cancers 15 03509Document23 pagesCancers 15 03509Mohammed KhalidNo ratings yet
- Retrospective Cohort - Wu, 2021Document10 pagesRetrospective Cohort - Wu, 2021Khusnul KhotimahNo ratings yet
- Long-Term Kidney Function of Childhood Cancer Survivors-Who Needs To Be Monitored?Document4 pagesLong-Term Kidney Function of Childhood Cancer Survivors-Who Needs To Be Monitored?Irawati Eka PutriNo ratings yet
- The Oncologist 2003 Weinstein 278 92Document15 pagesThe Oncologist 2003 Weinstein 278 92Josne J. PaezNo ratings yet
- Case Control 2003 UTSDocument6 pagesCase Control 2003 UTSpatientengagement.mhgNo ratings yet
- Albayrak 2016Document7 pagesAlbayrak 2016DavorIvanićNo ratings yet
- Kuipersetal CRC NRDP2015Document26 pagesKuipersetal CRC NRDP2015Robert ChristevenNo ratings yet
- Colorectal Cancer Screening in An Equal Access Healthcare SystemDocument11 pagesColorectal Cancer Screening in An Equal Access Healthcare SystemTri Rahma Yani YawatiNo ratings yet
- Intl Journal of Cancer - 2023 - Jiang - Association Between Antibiotic Use During Early Life and Early Onset ColorectalDocument10 pagesIntl Journal of Cancer - 2023 - Jiang - Association Between Antibiotic Use During Early Life and Early Onset ColorectalMohammed KhalidNo ratings yet
- Clinical Predictors of ExtenionDocument7 pagesClinical Predictors of ExtenionyaswanthkpNo ratings yet
- Ca Colon 2Document19 pagesCa Colon 2Tob JurNo ratings yet
- Jurnal CarisoprodolDocument9 pagesJurnal CarisoprodolTegarrachman23No ratings yet
- Disparities in Periodontitis Prevalence Among Chronic Kidney Disease PatientsDocument5 pagesDisparities in Periodontitis Prevalence Among Chronic Kidney Disease PatientsKristelle HernandezNo ratings yet
- Association Between Immune-Related Adverse Event TDocument8 pagesAssociation Between Immune-Related Adverse Event TAndrew FincoNo ratings yet
- Lingen Et Al-2011-Oral DiseasesDocument16 pagesLingen Et Al-2011-Oral DiseasesSAMUEL ESCARESNo ratings yet
- Review of Cancer CachexiaDocument46 pagesReview of Cancer CachexiahuwainannisaNo ratings yet
- Risk Factors For Necrotizing Enterocolitis Associated MortalityDocument7 pagesRisk Factors For Necrotizing Enterocolitis Associated MortalityvaleriaNo ratings yet
- JCM 11 02865Document9 pagesJCM 11 02865Andrio PalayukanNo ratings yet
- Seminar: Joana Torres, Saurabh Mehandru, Jean-Frédéric Colombel, Laurent Peyrin-BirouletDocument15 pagesSeminar: Joana Torres, Saurabh Mehandru, Jean-Frédéric Colombel, Laurent Peyrin-BirouletKaren ojedaNo ratings yet
- Healthmed 15 1 Damir SecicDocument6 pagesHealthmed 15 1 Damir SecicEdoHNo ratings yet
- Accepted Manuscript: Digestive and Liver DiseaseDocument28 pagesAccepted Manuscript: Digestive and Liver DiseaseMuhammad AdithiaNo ratings yet
- Non Steroidal Anti-Inflammatory Drugs As Anticancer Agents Mechanistic, Pharmacologic and Clinical IssuesDocument15 pagesNon Steroidal Anti-Inflammatory Drugs As Anticancer Agents Mechanistic, Pharmacologic and Clinical IssuesAlex Bastos BaptistaNo ratings yet
- Cancers 13 02025 v2Document23 pagesCancers 13 02025 v2Sha AbdulaNo ratings yet
- Preventive Medicine: Contents Lists Available atDocument5 pagesPreventive Medicine: Contents Lists Available atYenza FaheraNo ratings yet
- Early Life Body Fatness and Risk of Colon CancerDocument17 pagesEarly Life Body Fatness and Risk of Colon CancerNilufar K.No ratings yet
- Lectura 1 PDFDocument5 pagesLectura 1 PDFCarmen Castillo RequenaNo ratings yet
- Endoscopicscreeningfor Barrett'Sesophagusand EsophagealadenocarcinomaDocument15 pagesEndoscopicscreeningfor Barrett'Sesophagusand EsophagealadenocarcinomaduranaxelNo ratings yet
- Research Article: Characterization of Pediatric Acute Lymphoblastic Leukemia Survival Patterns by Age at DiagnosisDocument10 pagesResearch Article: Characterization of Pediatric Acute Lymphoblastic Leukemia Survival Patterns by Age at DiagnosisAnonymous aH8gCZ7zjNo ratings yet
- Clinical Progression JapanDocument6 pagesClinical Progression JapanyaswanthkpNo ratings yet
- Jurnal Radio 2Document9 pagesJurnal Radio 2Wahyu ApriantoNo ratings yet
- Thorax 2010 Ralph 863 9Document8 pagesThorax 2010 Ralph 863 9Alvita DewiNo ratings yet
- Edbk 159244Document11 pagesEdbk 159244ayuNo ratings yet
- Prevalensi Dan Faktor AsosiasiDocument11 pagesPrevalensi Dan Faktor Asosiasisahama2508No ratings yet
- Nihms 1768792Document35 pagesNihms 1768792Mohammed KhalidNo ratings yet
- Patrick TB ch15 Practice QuestionsDocument7 pagesPatrick TB ch15 Practice QuestionsMohammed KhalidNo ratings yet
- CNS McqsDocument54 pagesCNS McqsMohammed KhalidNo ratings yet
- Cadd Question Bank 8 SemDocument8 pagesCadd Question Bank 8 SemMohammed KhalidNo ratings yet
- REMIMAZOLA1Document2 pagesREMIMAZOLA1Mohammed KhalidNo ratings yet
- 2018 08 13 (一) 「醫療器材法規與實務」講座系列課程十二Document84 pages2018 08 13 (一) 「醫療器材法規與實務」講座系列課程十二Dr.Sivakumar SelvarajNo ratings yet
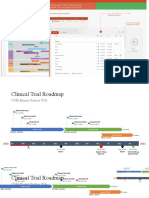
- Clinical Trial Roadmap Template - WsDocument4 pagesClinical Trial Roadmap Template - WsDaniel AlejandroNo ratings yet
- Jadwal Pir MalangDocument4 pagesJadwal Pir MalangAbraham BayuNo ratings yet
- Elizabeth Kiger Journal 11Document3 pagesElizabeth Kiger Journal 11api-556937362No ratings yet
- Salinas Perez Integrated Mapping Local MH Systems Central Chile 2018Document13 pagesSalinas Perez Integrated Mapping Local MH Systems Central Chile 2018xvhybfuNo ratings yet
- Episiotomy RcogDocument1 pageEpisiotomy RcogAisha RizwanNo ratings yet
- 3Rd Annual Transformational Ophthalmology Symposium: Saturday, OCTOBER 6, 2018 8:00 AM - 4:00 PMDocument5 pages3Rd Annual Transformational Ophthalmology Symposium: Saturday, OCTOBER 6, 2018 8:00 AM - 4:00 PMyos_peace86No ratings yet
- Smart 24-04-22Document78 pagesSmart 24-04-22humbleNo ratings yet
- Hospital-Bill-Form DDocument2 pagesHospital-Bill-Form Ddeharemmanuel64No ratings yet
- PUERPERAL SEPSIS CoverDocument9 pagesPUERPERAL SEPSIS CoverKerpersky LogNo ratings yet
- Sample Home Visit PlanDocument2 pagesSample Home Visit PlanCastallia LascuñaNo ratings yet
- Employee Performance Appraisal Instructions: PlanningDocument10 pagesEmployee Performance Appraisal Instructions: PlanningMylz MendozaNo ratings yet
- Types of Theories in NursingDocument12 pagesTypes of Theories in NursingEarl Von Giese Coniconde78% (9)
- Modeling Infectious Diseases in Humans and Animals: BookreviewsDocument3 pagesModeling Infectious Diseases in Humans and Animals: BookreviewsMORA CUEVAS NICOLE EDITHNo ratings yet
- Hep B Vaccine Drug StudyDocument2 pagesHep B Vaccine Drug StudyFrian MariñasNo ratings yet
- Penatalaksanaan Impaksi Caninus Permanen Rahang atDocument6 pagesPenatalaksanaan Impaksi Caninus Permanen Rahang atBinta Bhirawa AnoragaNo ratings yet
- Tamaraw PDFDocument2 pagesTamaraw PDFGab MolinaNo ratings yet
- Dasa Naadi: Clinical and Scientific ExplorationDocument3 pagesDasa Naadi: Clinical and Scientific ExplorationohanimiNo ratings yet
- The Different Types of IV Sets and Their UsesDocument1 pageThe Different Types of IV Sets and Their UsesPatricia VasquezNo ratings yet
- Course Name: Recruitment and SelectionDocument19 pagesCourse Name: Recruitment and SelectionZainab AsadNo ratings yet
- Aptirmiki: Error in Filling Death Certification On HIV Cases at A Teaching HospitalDocument5 pagesAptirmiki: Error in Filling Death Certification On HIV Cases at A Teaching HospitalAwalNo ratings yet
- Anesth Analg-1970-ALDRETE-924-34 PDFDocument11 pagesAnesth Analg-1970-ALDRETE-924-34 PDFYudiSiswantoWijaya100% (2)
- Head and Neck CancerDocument20 pagesHead and Neck CancerDartalina Sidauruk67% (3)
- ANNEX C Matrix of Devolved Basic Services and Facilities Based On LGC 1991Document9 pagesANNEX C Matrix of Devolved Basic Services and Facilities Based On LGC 1991Badeth AblaoNo ratings yet
- Literature Review Pressure Ulcer PreventionDocument7 pagesLiterature Review Pressure Ulcer Preventionc5r3aep1100% (1)
- Pharmaceuticals Executive Summary PDFDocument10 pagesPharmaceuticals Executive Summary PDFPaes C. MarceloNo ratings yet