Download as pdf or txt
You might also like
- Alberta Drivers HandbookDocument235 pagesAlberta Drivers HandbookHarsheen Kaur100% (1)
- 7E1 OperatingManualDocument2 pages7E1 OperatingManualSanjib Nath100% (1)
- OptiBlend System Operation and Installation ManualDocument9 pagesOptiBlend System Operation and Installation ManualVijendra PanwarNo ratings yet
- Philadelphia Distilling Cocktail MenuDocument1 pagePhiladelphia Distilling Cocktail MenuEaterNo ratings yet
- NGLRFWLR Facts 2015Document2 pagesNGLRFWLR Facts 2015Alex OnkenNo ratings yet
- Brain-Eating Amoeba Kills AgainDocument5 pagesBrain-Eating Amoeba Kills AgainIsaac KnarsNo ratings yet
- Brain Eating AmoebaDocument9 pagesBrain Eating AmoebaDr See Kin HaiNo ratings yet
- Naegleria Fowleri - AbstractDocument2 pagesNaegleria Fowleri - AbstractM3GA B0YNo ratings yet
- Free Living PDF MBCHB Amebae DR OtionoDocument31 pagesFree Living PDF MBCHB Amebae DR OtionoSante MunguyaNo ratings yet
- Entamoeba Coli: E. HistolyticaDocument15 pagesEntamoeba Coli: E. HistolyticaDavid Tritono Di BallastrossNo ratings yet
- Information On AmoebasDocument1 pageInformation On Amoebasbhuneshwar paswanNo ratings yet
- Naegleria FowleriDocument2 pagesNaegleria FowleriAnglophile123No ratings yet
- Brain-Eating Ameba (Naegleria)Document2 pagesBrain-Eating Ameba (Naegleria)gugicevdzoceNo ratings yet
- What Is Malaria?: World Health OrganizationDocument4 pagesWhat Is Malaria?: World Health OrganizationAko Si Vern ÖNo ratings yet
- Cours de MedcineDocument8 pagesCours de MedcineLAYLA AIZANo ratings yet
- PamidfsDocument3 pagesPamidfsapi-403838952No ratings yet
- What Is LeptospirosisDocument18 pagesWhat Is LeptospirosisLuphly TaluvtaNo ratings yet
- BrainDocument2 pagesBrainArshia ChandarkiNo ratings yet
- Naegleria Fowleri: Naegleria Fowleri Naegleria Fowleri, Colloquially Known As The "Brain-EatingDocument7 pagesNaegleria Fowleri: Naegleria Fowleri Naegleria Fowleri, Colloquially Known As The "Brain-EatingZied TrikiNo ratings yet
- Naegleria FowleriDocument18 pagesNaegleria FowlerijNo ratings yet
- Naegleria FowleriDocument18 pagesNaegleria Fowlerij100% (1)
- Naegleria ReviewDocument61 pagesNaegleria ReviewKʀɪsʜɴᴀ ϟNo ratings yet
- Opportunistic Amoeba Facultative ParasitesDocument25 pagesOpportunistic Amoeba Facultative ParasitesLizeth Querubin100% (10)
- Primary Amebic Meningoencephalitis (PAM)Document3 pagesPrimary Amebic Meningoencephalitis (PAM)Nur SeftihaniNo ratings yet
- Red Tide & Severe Acute Respiratory Syndrome (Sars) : Submitted By: Navarro, Joel D. BSN IiiDocument6 pagesRed Tide & Severe Acute Respiratory Syndrome (Sars) : Submitted By: Navarro, Joel D. BSN Iiijuel_navarroNo ratings yet
- MalariaDocument6 pagesMalariacris_itd100% (1)
- Primary Amoebic Meningoencephalitis: Fact Sheet - June 2010Document1 pagePrimary Amoebic Meningoencephalitis: Fact Sheet - June 2010Feyris TanNo ratings yet
- Parasite BlogDocument2 pagesParasite Blogapi-383716401No ratings yet
- The Problem and Its SettingsDocument2 pagesThe Problem and Its Settingsroneldayo62No ratings yet
- Typhoid FeverDocument47 pagesTyphoid FeverSujatha J Jayabal100% (2)
- Naegleris FowleriDocument21 pagesNaegleris FowleriAmanda PuspadewiNo ratings yet
- Climate Change & Waterborne Disease Climate Change & Waterborne DiseaseDocument16 pagesClimate Change & Waterborne Disease Climate Change & Waterborne DiseasetanishaNo ratings yet
- Naegleria Fowleri, The Causative Agent Of: Primary Amoebic MeningoencephalitisDocument10 pagesNaegleria Fowleri, The Causative Agent Of: Primary Amoebic MeningoencephalitisgugicevdzoceNo ratings yet
- And-Asses-At-Spring-Break-Pt-1-3/?from VBWN: LeptospirosisDocument8 pagesAnd-Asses-At-Spring-Break-Pt-1-3/?from VBWN: LeptospirosisEjie Boy IsagaNo ratings yet
- Primary Amebic Meningoencephalitis by Naegleria Fowleri: 15201010101083@students - Unej.ac - IdDocument2 pagesPrimary Amebic Meningoencephalitis by Naegleria Fowleri: 15201010101083@students - Unej.ac - IdKamila RahmaNo ratings yet
- PedrosDocument24 pagesPedroslorella_abejuelaNo ratings yet
- TyphoidDocument67 pagesTyphoidArnel L. SanicoNo ratings yet
- Naegleria Fowleri: The Brain-Eating AmoebaDocument1 pageNaegleria Fowleri: The Brain-Eating AmoebaAl Brelzhiv SarsalejoNo ratings yet
- Vibrio CholeraeDocument121 pagesVibrio CholeraemarkosfoxNo ratings yet
- Typhoid Fever March 10Document62 pagesTyphoid Fever March 10mirandadaNo ratings yet
- Lepto Spiros IsDocument7 pagesLepto Spiros IslansoprazoleNo ratings yet
- Typhoid Fever-Patho PhysiologyDocument6 pagesTyphoid Fever-Patho PhysiologyJohn Ervin AgenaNo ratings yet
- Microbes Present in Water and MilkDocument12 pagesMicrobes Present in Water and MilkMAHJABEENKHALILNo ratings yet
- Malaria: Ahmednagar Homoeopathic Medical College & Hospital AhmednagarDocument12 pagesMalaria: Ahmednagar Homoeopathic Medical College & Hospital AhmednagarSuhas IngaleNo ratings yet
- An Introduction of MalariaDocument19 pagesAn Introduction of MalariaSomesh GuptaNo ratings yet
- Malaria: Symptoms When Symptoms AppearDocument6 pagesMalaria: Symptoms When Symptoms AppearrbacaracNo ratings yet
- Food Borne DiseasesDocument9 pagesFood Borne DiseasesaringkinkingNo ratings yet
- FINAL Redtide & RABIES PPT KoDocument41 pagesFINAL Redtide & RABIES PPT KoLily CentenoNo ratings yet
- Malaria Is An Acute and Chronic Parasitic Disease: Etiologic AgentDocument6 pagesMalaria Is An Acute and Chronic Parasitic Disease: Etiologic AgentStephanie Rae BaccayNo ratings yet
- What Is Malaria?Document6 pagesWhat Is Malaria?Nikka MarieNo ratings yet
- Dengue: and Mosquito ControlDocument14 pagesDengue: and Mosquito ControlDeny KurniawanNo ratings yet
- Vibrio Cholerae Cholera AttackDocument1 pageVibrio Cholerae Cholera AttackAlexandra DolhăscuNo ratings yet
- Heartwater: OIE Terrestrial Manual 2008 217Document14 pagesHeartwater: OIE Terrestrial Manual 2008 217WormInchNo ratings yet
- Campy Lob ActerDocument2 pagesCampy Lob Acterkarenkaren09No ratings yet
- Vibrio CholeraeDocument5 pagesVibrio CholeraebloodstoragecentersuryaNo ratings yet
- Flavivirus, Family Flaviviridae Which Has Four Serotypes Are DEN-1, DEN-2Document26 pagesFlavivirus, Family Flaviviridae Which Has Four Serotypes Are DEN-1, DEN-2William Hartanto RusliNo ratings yet
- Naegleria Factsheet508cDocument2 pagesNaegleria Factsheet508cMustixaNo ratings yet
- TYPHOIDDocument13 pagesTYPHOIDnaceyjj33No ratings yet
- Medical Biology 2Document32 pagesMedical Biology 2Malik MohamedNo ratings yet
- Malaria Is A Mosquito-Borne Infectious Disease Caused by A Eukaryotic Protist of The GenusDocument5 pagesMalaria Is A Mosquito-Borne Infectious Disease Caused by A Eukaryotic Protist of The GenusMichael PadamaNo ratings yet
- Drought Awareness Newsletter by SlidesgoDocument61 pagesDrought Awareness Newsletter by SlidesgovetNo ratings yet
- Clinical Parasitology - Lecture (Report)Document41 pagesClinical Parasitology - Lecture (Report)Ezekiel Mark AdduruNo ratings yet
- Malaria: Biology Investigatory ProjectDocument21 pagesMalaria: Biology Investigatory ProjectAnonymous 5quBUnmvm1No ratings yet
- Macrophages in Immunoregulation and Therapeutics: Signal Transduction and Targeted TherapyDocument35 pagesMacrophages in Immunoregulation and Therapeutics: Signal Transduction and Targeted TherapygugicevdzoceNo ratings yet
- Evaluation of Classical, Alternative, and Regulatory Functions of Bone Marrow-Derived MacrophagesDocument11 pagesEvaluation of Classical, Alternative, and Regulatory Functions of Bone Marrow-Derived MacrophagesgugicevdzoceNo ratings yet
- Pathogenesis of Systemic Lupus Erythematosus: Risks, Mechanisms and Therapeutic TargetsDocument16 pagesPathogenesis of Systemic Lupus Erythematosus: Risks, Mechanisms and Therapeutic TargetsgugicevdzoceNo ratings yet
- Brain-Eating Ameba (Naegleria)Document2 pagesBrain-Eating Ameba (Naegleria)gugicevdzoceNo ratings yet
- Macrophages in Health and Disease: ReviewDocument21 pagesMacrophages in Health and Disease: ReviewgugicevdzoceNo ratings yet
- Mermh1Atotogp.: SbectionDocument1 pageMermh1Atotogp.: SbectiongugicevdzoceNo ratings yet
- Impact of Systemic Lupus Erythematosus On Oral Health-Related Quality of LifeDocument7 pagesImpact of Systemic Lupus Erythematosus On Oral Health-Related Quality of LifegugicevdzoceNo ratings yet
- The Pathogenesis of Psoriasis: Insight Into A Complex "Mobius Loop" Regulation ProcessDocument6 pagesThe Pathogenesis of Psoriasis: Insight Into A Complex "Mobius Loop" Regulation ProcessgugicevdzoceNo ratings yet
- Current Concepts in The Pathogenesis of Periodontitis: From Symbiosis To DysbiosisDocument20 pagesCurrent Concepts in The Pathogenesis of Periodontitis: From Symbiosis To DysbiosisgugicevdzoceNo ratings yet
- Urticarial Vasculitis Associated With Essential THDocument3 pagesUrticarial Vasculitis Associated With Essential THgugicevdzoceNo ratings yet
- EeeeDocument2 pagesEeeegugicevdzoceNo ratings yet
- The Effects of Atropine and Neostigmine On Heart Rate and RhythmDocument9 pagesThe Effects of Atropine and Neostigmine On Heart Rate and RhythmgugicevdzoceNo ratings yet
- 1Document22 pages1gugicevdzoceNo ratings yet
- Advances in The Pathogenesis and Treatment of Systemic Lupus ErythematosusDocument23 pagesAdvances in The Pathogenesis and Treatment of Systemic Lupus ErythematosusgugicevdzoceNo ratings yet
- 2Document23 pages2gugicevdzoceNo ratings yet
- Rheumatoid Arthritis: Pathogenesis, Clinical Features, and TreatmentDocument37 pagesRheumatoid Arthritis: Pathogenesis, Clinical Features, and TreatmentgugicevdzoceNo ratings yet
- A Short History of Japanese Historical Seismology: Past and The PresentDocument15 pagesA Short History of Japanese Historical Seismology: Past and The PresentgugicevdzoceNo ratings yet
- HHHHDocument5 pagesHHHHgugicevdzoceNo ratings yet
- Periodontal Disease and Its Association With Systemic DiseaseDocument5 pagesPeriodontal Disease and Its Association With Systemic DiseasegugicevdzoceNo ratings yet
- Guideline On The Use of Pharmacokinetics and Pharmacodynamics in The Development of Antimicrobial Medicinal ProductsDocument17 pagesGuideline On The Use of Pharmacokinetics and Pharmacodynamics in The Development of Antimicrobial Medicinal ProductsgugicevdzoceNo ratings yet
- Ellis Maitland Jones 1932 Mikulicz S SyndromeDocument1 pageEllis Maitland Jones 1932 Mikulicz S SyndromegugicevdzoceNo ratings yet
- Myxo 1Document8 pagesMyxo 1gugicevdzoceNo ratings yet
- Porter Et Al 1998 Recurrent Aphthous StomatitisDocument16 pagesPorter Et Al 1998 Recurrent Aphthous StomatitisgugicevdzoceNo ratings yet
- Acute Viral Encephalitis: Review ArticleDocument10 pagesAcute Viral Encephalitis: Review ArticlegugicevdzoceNo ratings yet
- What Are Alfalfa SproutsDocument4 pagesWhat Are Alfalfa SproutsPaul SagunNo ratings yet
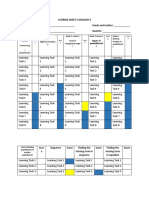
- Pivot Assessment and Scoring SheetDocument5 pagesPivot Assessment and Scoring SheetElaineVidalRodriguezNo ratings yet
- UNIT#2 Power SourceDocument49 pagesUNIT#2 Power SourceRTPS CCRNo ratings yet
- A0054M80021-Wiring Diagrams and Component LocationsDocument1,982 pagesA0054M80021-Wiring Diagrams and Component LocationsJameson Powers100% (1)
- Christina H. Parks: Magna Cum Laude, Chemistry HonorsDocument2 pagesChristina H. Parks: Magna Cum Laude, Chemistry HonorsTim BrownNo ratings yet
- Theory and Measurement of Bacterial GrowthDocument11 pagesTheory and Measurement of Bacterial GrowthBi Anh100% (1)
- Orif ReportDocument5 pagesOrif ReportduypalaNo ratings yet
- Safety of Microneedles For Transdermal Drug DeliveryDocument2 pagesSafety of Microneedles For Transdermal Drug DeliveryHiep X NguyenNo ratings yet
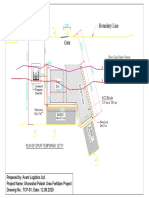
- Boundary Line: Plan of Gpuff Temporary JettyDocument1 pageBoundary Line: Plan of Gpuff Temporary Jettyshafiq_05No ratings yet
- Basic Aviation Medicine: DR Firman Rachman Masjhur SPKP 17 November 2014Document43 pagesBasic Aviation Medicine: DR Firman Rachman Masjhur SPKP 17 November 2014sunarniNo ratings yet
- Sda Church History 1863-1888Document17 pagesSda Church History 1863-1888Tawonga RushambwaNo ratings yet
- Curriculum Vitae DR SumitDocument3 pagesCurriculum Vitae DR SumitdrsumitpuriNo ratings yet
- Exercise LMTDocument4 pagesExercise LMTapi-276845347No ratings yet
- Bata Bata Pano Ka GinawaDocument1 pageBata Bata Pano Ka GinawaVivien BernosNo ratings yet
- Section 12 Welding Hardfacing266 27351Document69 pagesSection 12 Welding Hardfacing266 27351manuel_plfNo ratings yet
- Collocation With Common VerbsDocument2 pagesCollocation With Common VerbsKat_23No ratings yet
- Causes of MeanderingDocument1 pageCauses of MeanderingBalagopal V50% (2)
- CHEM0414ra ManilaDocument21 pagesCHEM0414ra ManilaangelomercedeblogNo ratings yet
- Experiment No. 2: "To Demonstrate The Validity of Bernoulli's Equation WhenDocument7 pagesExperiment No. 2: "To Demonstrate The Validity of Bernoulli's Equation WhenumairNo ratings yet
- Karakteristik Ekosistem Mangrove Di Kawasan Pesisi PDFDocument7 pagesKarakteristik Ekosistem Mangrove Di Kawasan Pesisi PDFAdilNo ratings yet
- Nuvance Health Strategic PlanDocument7 pagesNuvance Health Strategic Planfranjo bacicNo ratings yet
- Stability CosmeticDocument47 pagesStability CosmeticAgustin E SetiowatiNo ratings yet
- ISO 14001-Claus-4.4.1Document2 pagesISO 14001-Claus-4.4.1Navnath TamhaneNo ratings yet
- The Nature of DreamsDocument2 pagesThe Nature of DreamsWesternLNo ratings yet
- Walang Rape Sa Bontoc ReactionDocument4 pagesWalang Rape Sa Bontoc ReactionJed HernandezNo ratings yet
- Foremans Topic V2 78F Classes of FireDocument2 pagesForemans Topic V2 78F Classes of FireAnonymous 5PsGXCNo ratings yet