Download as pdf or txt
You might also like
- Bolens Lawn Tractor RepairDocument46 pagesBolens Lawn Tractor Repairdakehi1188342157% (7)
- Conservative Management of Perforated Peptic UlcerDocument4 pagesConservative Management of Perforated Peptic UlcerAfiani JannahNo ratings yet
- TM46 BDocument24 pagesTM46 BMekaNo1D100% (1)
- Interfacing A VOR/LOC/Glideslope Indicator byDocument17 pagesInterfacing A VOR/LOC/Glideslope Indicator byeumesmo222No ratings yet
- Overview of Functions and Operations BSPDocument2 pagesOverview of Functions and Operations BSPKarla GalvezNo ratings yet
- 1 s2.0 S009082580095995X MainDocument3 pages1 s2.0 S009082580095995X Maintamhujin456No ratings yet
- Se Hacía Biopsia A Los Tres Meses. Estudio Pequeño ADocument5 pagesSe Hacía Biopsia A Los Tres Meses. Estudio Pequeño Aouf81No ratings yet
- 4451 FullDocument4 pages4451 FullSukhvinder Singh RanaNo ratings yet
- Ulcerative ColitisDocument8 pagesUlcerative Colitisfidah12012000No ratings yet
- Early Ercp and Papillotomy Compared With Conservative Treatment For Acute Biliary PancreatitisDocument6 pagesEarly Ercp and Papillotomy Compared With Conservative Treatment For Acute Biliary PancreatitisRT_BokNo ratings yet
- CA180-274 Synopsis RedactedDocument7 pagesCA180-274 Synopsis RedactedAnonymous jjdtnLrxaNo ratings yet
- 28-Year-Old Man With Crohn Disease and Hematuria: Residents ' ClinicDocument5 pages28-Year-Old Man With Crohn Disease and Hematuria: Residents ' ClinicDesi HutapeaNo ratings yet
- Moskovitz 2005Document5 pagesMoskovitz 2005DavorIvanićNo ratings yet
- Docetaxel, Ifosfamide and Cisplatin (DIP) in Squamous Cell Carcinoma of The Head and NeckDocument6 pagesDocetaxel, Ifosfamide and Cisplatin (DIP) in Squamous Cell Carcinoma of The Head and NeckSukhvinder Singh RanaNo ratings yet
- Medicine 1Document2 pagesMedicine 1ÇağlaNo ratings yet
- Esophageal CancerDocument21 pagesEsophageal CancerYogesh ShindeNo ratings yet
- Management of Neoplastic Pericardial EffusionsDocument4 pagesManagement of Neoplastic Pericardial EffusionsMamamia DonchanNo ratings yet
- Thyroid Suppression Test With L-Thyroxine and TC) PertechnetateDocument7 pagesThyroid Suppression Test With L-Thyroxine and TC) PertechnetatejeffsunilNo ratings yet
- 2867 FullDocument5 pages2867 FullAhmad FauzanNo ratings yet
- Tanum1991 (Biopsia A Todos)Document5 pagesTanum1991 (Biopsia A Todos)ouf81No ratings yet
- Azithromycin and Gentamicin Therapy For The Treatment of Humans With BrucellosisDocument4 pagesAzithromycin and Gentamicin Therapy For The Treatment of Humans With BrucellosisveroarujogonzalesNo ratings yet
- 74 FullDocument3 pages74 FullNoel Saúl Argüello SánchezNo ratings yet
- 551 PDFDocument5 pages551 PDFfaidgustisyarifNo ratings yet
- Articulo 3Document12 pagesArticulo 3JOSE MONTERONo ratings yet
- Tocilizumab Appraisal GRP 9Document5 pagesTocilizumab Appraisal GRP 9Kurt CabahugNo ratings yet
- Appropriate Antibiotics For Peritonsillar Abscess - A 9 Month CohortDocument5 pagesAppropriate Antibiotics For Peritonsillar Abscess - A 9 Month CohortSiti Annisa NurfathiaNo ratings yet
- NPCDocument8 pagesNPCArsy Mira PertiwiNo ratings yet
- Miller1991 (Justifica PQ Biopsia A Todos)Document4 pagesMiller1991 (Justifica PQ Biopsia A Todos)ouf81No ratings yet
- Block G Pre Proff KGMC 2022-PrintDocument23 pagesBlock G Pre Proff KGMC 2022-PrintF ParikhNo ratings yet
- 1 s2.0 S0090825805007328 MainDocument6 pages1 s2.0 S0090825805007328 Maintamhujin456No ratings yet
- TMC 207 (Bedaquiline) : A New Weapon Against MDR and XDR-TB: Presented by Mohit Kumar Dwivedi Ms - Pharm 1 SEM BiotechnologyDocument19 pagesTMC 207 (Bedaquiline) : A New Weapon Against MDR and XDR-TB: Presented by Mohit Kumar Dwivedi Ms - Pharm 1 SEM BiotechnologyMahesh T MadhavanNo ratings yet
- JCO 2003 Lin 631 7Document7 pagesJCO 2003 Lin 631 7Adhika Manggala DharmaNo ratings yet
- Critically Ill 75 Year Old Man With ComplicationsDocument20 pagesCritically Ill 75 Year Old Man With ComplicationssummiyaNo ratings yet
- NejmoaDocument9 pagesNejmoamangosidNo ratings yet
- Pharmacokinetic & Clinical Studies On CefuroximeDocument9 pagesPharmacokinetic & Clinical Studies On CefuroximeMary Duane A. PranzaNo ratings yet
- Colovesical FistulaDocument4 pagesColovesical FistulaNisaNo ratings yet
- ARTIGO1Document9 pagesARTIGO1jtnylsonNo ratings yet
- JOURNAL Treating Acute Urinary Tract InfectionsDocument5 pagesJOURNAL Treating Acute Urinary Tract InfectionsKhayelee PalosNo ratings yet
- C122 Early Post TURB Instillational Treatment in Ta, T1 Bladder CancersDocument1 pageC122 Early Post TURB Instillational Treatment in Ta, T1 Bladder CancersOkki Masitah Syahfitri NasutionNo ratings yet
- Capecitabine Monotherapy For Recurrent and Metastatic Nasopharyngeal CancerDocument6 pagesCapecitabine Monotherapy For Recurrent and Metastatic Nasopharyngeal Cancertrifamonika23No ratings yet
- S. GALLOON, M.D., CH.B., F.F.A.R.C.S. : e T AlDocument14 pagesS. GALLOON, M.D., CH.B., F.F.A.R.C.S. : e T AlLani Munawir Holis HolisNo ratings yet
- 8Document8 pages8Sandu AlexandraNo ratings yet
- JCO 2005 Low 2726 34Document9 pagesJCO 2005 Low 2726 34Donny Artya KesumaNo ratings yet
- Klebsiella Pneumoniae Case ReportDocument3 pagesKlebsiella Pneumoniae Case ReportMaria Chacón CarbajalNo ratings yet
- General Surgery: Ruptured Liver Abscess: A Novel Surgical TechniqueDocument3 pagesGeneral Surgery: Ruptured Liver Abscess: A Novel Surgical TechniqueRahul SinghNo ratings yet
- Tipton 2006Document5 pagesTipton 2006Patricia BezneaNo ratings yet
- Treatment of Toxic Epidermal Necrolysis With Intravenous ImmunoglobulinDocument5 pagesTreatment of Toxic Epidermal Necrolysis With Intravenous ImmunoglobulinUbaidillah HafidzNo ratings yet
- Scientific Letter: Archivos de Bronconeumología 58 (2022) T457-T460Document4 pagesScientific Letter: Archivos de Bronconeumología 58 (2022) T457-T460johannaNo ratings yet
- Erbitux MonotherapyDocument7 pagesErbitux MonotherapyMaulik PatelNo ratings yet
- 3908 FullDocument7 pages3908 FullJavier MedinaNo ratings yet
- 1 s2.0 S0007091217447246 MainDocument5 pages1 s2.0 S0007091217447246 MainFani LiyaraniNo ratings yet
- 1 s2.0 S2214442022002121 MainDocument3 pages1 s2.0 S2214442022002121 MainGregory AssonitisNo ratings yet
- 1097 0142 28197611 2938 3A5 3C1909 3A 3aaid cncr2820380507 3e3.0.co 3B2 QDocument8 pages1097 0142 28197611 2938 3A5 3C1909 3A 3aaid cncr2820380507 3e3.0.co 3B2 QLata DeshmukhNo ratings yet
- Pre-Operative Albendazole Therapy For Hydatid Cyst: 10 of ofDocument2 pagesPre-Operative Albendazole Therapy For Hydatid Cyst: 10 of ofIbtissam BelehssenNo ratings yet
- Treatment Outcomes of Inmates With Pulmonary Tuberculosis in Baquba Penitentiary: A Follow-Up StudyDocument5 pagesTreatment Outcomes of Inmates With Pulmonary Tuberculosis in Baquba Penitentiary: A Follow-Up StudyTengku Reza MaulanaNo ratings yet
- Fibrinogen Catabolism in Systemic Erythematosus: LupusDocument4 pagesFibrinogen Catabolism in Systemic Erythematosus: LupusRazvanNo ratings yet
- 2 PDFDocument5 pages2 PDFBangladesh Academy of SciencesNo ratings yet
- BJC 2013230Document6 pagesBJC 2013230Abraham OsunaNo ratings yet
- Gemcitabine 4 PDFDocument3 pagesGemcitabine 4 PDFhestiNo ratings yet
- Efficacy of The anti-TNF-a Antibody Infliximab Against Refractory Systemic Vasculitides: An Open Pilot Study On 10 PatientsDocument7 pagesEfficacy of The anti-TNF-a Antibody Infliximab Against Refractory Systemic Vasculitides: An Open Pilot Study On 10 Patientsutkarsh PromotiomNo ratings yet
- 2000 - Frankel - Re Radical Prostatectomy For Localized Prostate Cancer Provides Durable Cancer Control With Excellent Quality of Life A STRDocument2 pages2000 - Frankel - Re Radical Prostatectomy For Localized Prostate Cancer Provides Durable Cancer Control With Excellent Quality of Life A STRPoljarLijanNo ratings yet
- Tagraxofuso Followed by Combined Azacitidine and Venetoclax in Blastic Plasmacytoid Dendritic Cell Neoplasm - A Case Report and Literature ReviewDocument6 pagesTagraxofuso Followed by Combined Azacitidine and Venetoclax in Blastic Plasmacytoid Dendritic Cell Neoplasm - A Case Report and Literature ReviewZedodurexNo ratings yet
- Concurrent Radiotherapy and Weekly Paclitaxel For Locally Advanced Squmous Cell Carcinoma of Uterine Cervix-Treated Patients at Rural Centre in IndiaDocument5 pagesConcurrent Radiotherapy and Weekly Paclitaxel For Locally Advanced Squmous Cell Carcinoma of Uterine Cervix-Treated Patients at Rural Centre in IndiaIjsrnet EditorialNo ratings yet
- Top Trials in Gastroenterology & HepatologyFrom EverandTop Trials in Gastroenterology & HepatologyRating: 4.5 out of 5 stars4.5/5 (7)
- Dindo2009 PDFDocument6 pagesDindo2009 PDFDavorIvanićNo ratings yet
- Fujiwara 2019Document6 pagesFujiwara 2019DavorIvanićNo ratings yet
- Arends 2016Document7 pagesArends 2016DavorIvanićNo ratings yet
- Lehman 2004Document7 pagesLehman 2004DavorIvanićNo ratings yet
- Luna 1973Document2 pagesLuna 1973DavorIvanićNo ratings yet
- Konety 2020Document1 pageKonety 2020DavorIvanićNo ratings yet
- Lammers 2014Document9 pagesLammers 2014DavorIvanićNo ratings yet
- Sexual ReproductionDocument6 pagesSexual ReproductionAlyssa Margareth SorianoNo ratings yet
- Advanced 250 V Three-Phase BLDC Controller With Embedded STM32 MCUDocument32 pagesAdvanced 250 V Three-Phase BLDC Controller With Embedded STM32 MCUOne SpringNo ratings yet
- Abb 1677859211Document43 pagesAbb 1677859211Mohamed ElsayedNo ratings yet
- Change From The Inside Out Andersen en 45521Document6 pagesChange From The Inside Out Andersen en 45521AraceliDemetrioNo ratings yet
- The Wheel and The BobsleighDocument2 pagesThe Wheel and The BobsleighHarisNo ratings yet
- Audio CodecDocument3 pagesAudio CodecSandeep Kumar YadlapalliNo ratings yet
- Joseph D. Robinson - Mechanisms of Synaptic Transmission - Bridging The Gaps (1890-1990) (2001)Document468 pagesJoseph D. Robinson - Mechanisms of Synaptic Transmission - Bridging The Gaps (1890-1990) (2001)Pablo EspinosaNo ratings yet
- CH # 4 AudioDocument55 pagesCH # 4 AudioHamza Nazir Hamza NazirNo ratings yet
- A Study On The Effect of Welding Sequence in Fabrication of Large Stiffened Plate Panels (Paper)Document8 pagesA Study On The Effect of Welding Sequence in Fabrication of Large Stiffened Plate Panels (Paper)pal_malayNo ratings yet
- Class 4 GK WorksheetDocument21 pagesClass 4 GK WorksheetJayesh Shukla0% (1)
- Module 11Document64 pagesModule 11Andrew Dela CruzNo ratings yet
- FractureDocument16 pagesFractureps4haris.ch3534No ratings yet
- Germany Import ExportDocument12 pagesGermany Import Exporttariquekhan143No ratings yet
- CBSE Class 10 History Chapter 3 SolutionsDocument5 pagesCBSE Class 10 History Chapter 3 SolutionsVeeresh KaranamNo ratings yet
- Tabatana 2023 ReportDocument15 pagesTabatana 2023 ReportKudakwashe Pride ChirendaNo ratings yet
- Learning Module 1 1Document16 pagesLearning Module 1 1BConstantino, Jan Louie Z.No ratings yet
- ASSOCHAM Aviotech Study On Aerospace and Defence Manufacturing in IndiaDocument23 pagesASSOCHAM Aviotech Study On Aerospace and Defence Manufacturing in IndiarahulgangalNo ratings yet
- Belt Reeler BrochureDocument4 pagesBelt Reeler BrochureRestuNo ratings yet
- Thesis Statement For One Hundred Years of SolitudeDocument6 pagesThesis Statement For One Hundred Years of Solitudegxirgjwff100% (2)
- Math 241 Section 2.1 (3-2-2021)Document20 pagesMath 241 Section 2.1 (3-2-2021)H ANo ratings yet
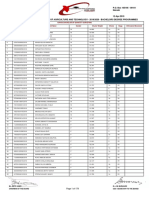
- JKUAT Bachelors Degree Placement ListDocument179 pagesJKUAT Bachelors Degree Placement ListDiana WangamatiNo ratings yet
- 100 Korean Proverbs With Meanings For TOPIK 2Document19 pages100 Korean Proverbs With Meanings For TOPIK 2Rumah Sakit Bhakti NugrahaNo ratings yet
- Expt - 11: JFET CharacteristicsDocument8 pagesExpt - 11: JFET CharacteristicssamarthNo ratings yet
- The Statistical Distribution of The Maxima of A Random Function by Cartwright and Longuet HigginsDocument22 pagesThe Statistical Distribution of The Maxima of A Random Function by Cartwright and Longuet Higginsadaniliu13No ratings yet
- Emily Gerard Transylvanian SuperstitionsDocument4 pagesEmily Gerard Transylvanian SuperstitionsErzsebet HeghyekNo ratings yet
- 5070 s17 Ms 31 PDFDocument4 pages5070 s17 Ms 31 PDFAl-Qayyuum T.G1753No ratings yet