Download as pdf or txt
You might also like
- Test Bank For Principles of Macroeconomics 6th Canadian Edition by Sayre PDFDocument49 pagesTest Bank For Principles of Macroeconomics 6th Canadian Edition by Sayre PDFHemant BhatnagarNo ratings yet
- MCQ Companion To The Eye Basic Sciences in PracticeDocument139 pagesMCQ Companion To The Eye Basic Sciences in PracticeАнагаахын ОрчуулгаNo ratings yet
- TropocellsDocument6 pagesTropocellsIsrael Exporter100% (1)
- Clinical Outcomes of Vertical Bone Augmentation To Enable Dental Implant Placement: A Systematic ReviewDocument13 pagesClinical Outcomes of Vertical Bone Augmentation To Enable Dental Implant Placement: A Systematic Reviewvanessa_werbickyNo ratings yet
- Gramática AwáDocument422 pagesGramática AwáJaghu San100% (1)
- Injectable Platelet Rich Fibrin (i-PRF) : Opportunities in Regenerative Dentistry?Document9 pagesInjectable Platelet Rich Fibrin (i-PRF) : Opportunities in Regenerative Dentistry?RENATO SUDATINo ratings yet
- Injectable Platelet Rich Fibrin (i-PRF) : Opportunities in Regenerative Dentistry?Document9 pagesInjectable Platelet Rich Fibrin (i-PRF) : Opportunities in Regenerative Dentistry?Bruno MañonNo ratings yet
- Improved Growth Factor Delivery and Cellular Activity Using Concentrated Platelet-Rich Fibrin (C-PRF) When Compared With Traditional Injectable (i-PRF) ProtocolsDocument11 pagesImproved Growth Factor Delivery and Cellular Activity Using Concentrated Platelet-Rich Fibrin (C-PRF) When Compared With Traditional Injectable (i-PRF) Protocolsxiaoxin zhangNo ratings yet
- Clinicalusesofplatelet-Rich Fibrininoraland MaxillofacialsurgeryDocument13 pagesClinicalusesofplatelet-Rich Fibrininoraland MaxillofacialsurgeryCBMF UPCHNo ratings yet
- Biologicals: Mito Kobayashi, Tomoyuki Kawase, Makoto Horimizu, Kazuhiro Okuda, Larry F. Wolff, Hiromasa YoshieDocument7 pagesBiologicals: Mito Kobayashi, Tomoyuki Kawase, Makoto Horimizu, Kazuhiro Okuda, Larry F. Wolff, Hiromasa YoshieVijay Prabu GNo ratings yet
- PRF PeriodontiaDocument8 pagesPRF PeriodontiaDANIELA MARTINS LEITENo ratings yet
- Huda Ragheb - PRP - CosmeticsDocument7 pagesHuda Ragheb - PRP - Cosmeticsraghebhuda4No ratings yet
- Role of PRF in ProsthodonticsDocument11 pagesRole of PRF in ProsthodonticsAkshayaa BalajiNo ratings yet
- Microneedling and PRP For Acne Scars: A New Tool in Our ArsenalDocument3 pagesMicroneedling and PRP For Acne Scars: A New Tool in Our ArsenalThaís SagratzhiNo ratings yet
- JCD Platelet-Rich Plasma, The Ultimate Secret For Youthful Skin RADDocument8 pagesJCD Platelet-Rich Plasma, The Ultimate Secret For Youthful Skin RADyellowbieNo ratings yet
- Ijdr 12414Document5 pagesIjdr 12414Ahmed BadrNo ratings yet
- Telomere Length and Genetic Variations Affecting TelomereDocument6 pagesTelomere Length and Genetic Variations Affecting TelomereNathaliaNo ratings yet
- Bioengineering 09 00405Document14 pagesBioengineering 09 00405Rozalina LoebisNo ratings yet
- Biological Characterization of An Injectable Platelet-Rich Fibrin Mixture Consisting of Autologous Albumin Gel and Liquid Platelet-Rich Fibrin (Alb-PRF)Document9 pagesBiological Characterization of An Injectable Platelet-Rich Fibrin Mixture Consisting of Autologous Albumin Gel and Liquid Platelet-Rich Fibrin (Alb-PRF)xiaoxin zhangNo ratings yet
- PRP 1Document6 pagesPRP 1irvinaldi9No ratings yet
- Etm 19 4 3024 PDFDocument7 pagesEtm 19 4 3024 PDFEstetika MedikNo ratings yet
- Comparatie PRF - PRP - PRGF 4 Pagini Intr-O CarteDocument4 pagesComparatie PRF - PRP - PRGF 4 Pagini Intr-O CarteZelinschi Dragos ChristianNo ratings yet
- 10.1007@s00403 019 01936 7Document4 pages10.1007@s00403 019 01936 7Ananda SantosNo ratings yet
- Use of PRP, PRF and CGF in Periodontal Regeneration andDocument23 pagesUse of PRP, PRF and CGF in Periodontal Regeneration andmaria teresa pertuz rondonNo ratings yet
- Shantipriya Reddy, Enhancing Palatal Wound HealingDocument3 pagesShantipriya Reddy, Enhancing Palatal Wound Healingdimiz77No ratings yet
- IJD15183119Document10 pagesIJD15183119Estetika MedikNo ratings yet
- Jop 2012 110705Document9 pagesJop 2012 110705Mandy ConnerNo ratings yet
- A Review of Platelet-Rich Plasma: History, Biology, Mechanism of Action, and ClassificationDocument7 pagesA Review of Platelet-Rich Plasma: History, Biology, Mechanism of Action, and ClassificationPoppyA.NamiraNo ratings yet
- Sclafani PRFM For FPS Clinics FPSDocument11 pagesSclafani PRFM For FPS Clinics FPSdanielagonzalezt5No ratings yet
- 10 11607@jomi 6604Document7 pages10 11607@jomi 6604Daniel GorgaNo ratings yet
- LPRF IntroduccionDocument12 pagesLPRF IntroduccionbezinlizeNo ratings yet
- Apexa No 5Document3 pagesApexa No 5Apexa YadavNo ratings yet
- Sclafani 2011Document5 pagesSclafani 2011dimiz77No ratings yet
- Histological Comparison of Platelet Rich Fibrin Clots Prepared by Fixed-Angle Versus Horizontal CentrifugationDocument8 pagesHistological Comparison of Platelet Rich Fibrin Clots Prepared by Fixed-Angle Versus Horizontal Centrifugationxiaoxin zhangNo ratings yet
- Evaluation of Platelet-Rich Plasma and MicroneedliDocument8 pagesEvaluation of Platelet-Rich Plasma and MicroneedliRamya DivyaNo ratings yet
- Anthony P. Sclafani, MD, PRFM, FacialDocument5 pagesAnthony P. Sclafani, MD, PRFM, Facialdimiz77No ratings yet
- Masuki2016 Article GrowthFactorAndPro-InflammatorDocument6 pagesMasuki2016 Article GrowthFactorAndPro-InflammatorRENATO SUDATINo ratings yet
- Advanced Platelet-Rich Fibrin A New Concept For Cell-Based Tissue Engineering by Means of Inflammatory CellsDocument11 pagesAdvanced Platelet-Rich Fibrin A New Concept For Cell-Based Tissue Engineering by Means of Inflammatory CellsmaxNo ratings yet
- Wang2017 PDFDocument9 pagesWang2017 PDFRENATO SUDATINo ratings yet
- PRP in Facial Rejuvenation - Dras. Rawashdeh y TorricoDocument68 pagesPRP in Facial Rejuvenation - Dras. Rawashdeh y TorricoDra. Andrea Jiménez BelloNo ratings yet
- PRP Hyperpigmentatino - Uysal2017Document1 pagePRP Hyperpigmentatino - Uysal2017BiraimaNo ratings yet
- Platelet Rich Plasma (PRP) For Facial RejuvenationDocument48 pagesPlatelet Rich Plasma (PRP) For Facial RejuvenationnageenthrenNo ratings yet
- Adj 12754Document12 pagesAdj 12754Irfan HussainNo ratings yet
- Utility of Platelet-Rich Plasma in Aesthetics: Ryan C. Kelm, MD, Omer Ibrahim, MDDocument10 pagesUtility of Platelet-Rich Plasma in Aesthetics: Ryan C. Kelm, MD, Omer Ibrahim, MDDubraska SuárezNo ratings yet
- LPRF PRGF CPBDocument8 pagesLPRF PRGF CPBbezinlizeNo ratings yet
- Use of Platelet-Rich Fibrin Membrane Following Treatment of Gingival Recession: A Randomized Clinical TrialDocument4 pagesUse of Platelet-Rich Fibrin Membrane Following Treatment of Gingival Recession: A Randomized Clinical TrialAurora Hadijah GodfriedNo ratings yet
- 1 s2.0 S246878551930165X MainDocument5 pages1 s2.0 S246878551930165X MainNurulhannanNo ratings yet
- Platelet Rich PlasmaDocument3 pagesPlatelet Rich PlasmaInternational Organization of Scientific Research (IOSR)100% (1)
- Article 1443718317Document9 pagesArticle 1443718317antariksha DodNo ratings yet
- Platelet-Rich Plasma As A Potential New Strategy in The Endometrium Treatment in Assisted Reproductive TechnologyDocument12 pagesPlatelet-Rich Plasma As A Potential New Strategy in The Endometrium Treatment in Assisted Reproductive TechnologyLuis Napoleón Castro Sanz100% (1)
- Platelt Rich FibrinDocument7 pagesPlatelt Rich FibrinCristina RusnacNo ratings yet
- PRP 3Document13 pagesPRP 3irvinaldi9No ratings yet
- Plasma Rico en Plaquetas para El Rejuvenecimiento FacialDocument5 pagesPlasma Rico en Plaquetas para El Rejuvenecimiento FacialHeidy IxcaraguaNo ratings yet
- A Comprehensive Review of Concentrated Growth Factors and Their Novel Applications in Facial Reconstructive and Regenerative MedicineDocument11 pagesA Comprehensive Review of Concentrated Growth Factors and Their Novel Applications in Facial Reconstructive and Regenerative MedicineHiktor TomNo ratings yet
- ArpfDocument8 pagesArpfTiruvalliUttamkumarNo ratings yet
- Applications of Platelet Rich Plasma PDFDocument6 pagesApplications of Platelet Rich Plasma PDFRamona MateiNo ratings yet
- Applications of Platelet Rich Plasma Fo PDFDocument6 pagesApplications of Platelet Rich Plasma Fo PDFRamona MateiNo ratings yet
- PRF 1) Introduction To PRFDocument4 pagesPRF 1) Introduction To PRFBakar123 ShimoNo ratings yet
- Enhancing Bone RegenerationDocument7 pagesEnhancing Bone RegenerationCarlosWaitforitNo ratings yet
- 7 Efect of Relative Centrifugal Force On The Biological Properties of LiquidDocument11 pages7 Efect of Relative Centrifugal Force On The Biological Properties of Liquidxiaoxin zhangNo ratings yet
- Thanasrisuebwong2019 PDFDocument10 pagesThanasrisuebwong2019 PDFRENATO SUDATINo ratings yet
- Applications of Leukocyte - and Platelet-Rich Plasma (L-PRP) in TraumaDocument12 pagesApplications of Leukocyte - and Platelet-Rich Plasma (L-PRP) in TraumaEdgar Pantoja100% (1)
- The Role of Autophagy in Skin Fibroblasts, Keratinocytes, Melanocytes, and Epidermal Stem CellsDocument7 pagesThe Role of Autophagy in Skin Fibroblasts, Keratinocytes, Melanocytes, and Epidermal Stem Cellsvanessa_werbickyNo ratings yet
- Rahe 2017Document6 pagesRahe 2017vanessa_werbickyNo ratings yet
- Treatment of Soft Tissue Filler Complications Expert Consensus RecommendationsDocument13 pagesTreatment of Soft Tissue Filler Complications Expert Consensus Recommendationsvanessa_werbickyNo ratings yet
- Cshperspectmed SKN A015339Document20 pagesCshperspectmed SKN A015339vanessa_werbickyNo ratings yet
- Treatment of Dark Circles With The New 15 MGML Hyaluronic Acid Filler With LidocaineDocument2 pagesTreatment of Dark Circles With The New 15 MGML Hyaluronic Acid Filler With Lidocainevanessa_werbickyNo ratings yet
- Bioengineering The Microanatomy of Human SkinDocument18 pagesBioengineering The Microanatomy of Human Skinvanessa_werbickyNo ratings yet
- Wound Healing and Fibrosis A Contrasting Role For Periostin in Skin and The Oral MucosaDocument13 pagesWound Healing and Fibrosis A Contrasting Role For Periostin in Skin and The Oral Mucosavanessa_werbickyNo ratings yet
- Skin Filling and Firming Activity of A HyaluronicDocument10 pagesSkin Filling and Firming Activity of A Hyaluronicvanessa_werbickyNo ratings yet
- Fowler SlidesManiaDocument19 pagesFowler SlidesManiavanessa_werbickyNo ratings yet
- Biological Mediators For Periodontal RegenerationDocument19 pagesBiological Mediators For Periodontal Regenerationvanessa_werbickyNo ratings yet
- Biological Activity of Bone Morphogenetic ProteinsDocument4 pagesBiological Activity of Bone Morphogenetic Proteinsvanessa_werbickyNo ratings yet
- Blackboard SlidesManiaDocument23 pagesBlackboard SlidesManiavanessa_werbickyNo ratings yet
- 2009 Article 52Document7 pages2009 Article 52vanessa_werbickyNo ratings yet
- Unveiling Novel Genes Upregulated by Both Rhbmp2 and Rhbmp7 During Early Osteoblastic Transdifferentiation of C2C12 CellsDocument15 pagesUnveiling Novel Genes Upregulated by Both Rhbmp2 and Rhbmp7 During Early Osteoblastic Transdifferentiation of C2C12 Cellsvanessa_werbickyNo ratings yet
- Mesenchymal Stem Cells With Rhbmp-2 Inhibits The Growth of Canine Osteosarcoma CellsDocument9 pagesMesenchymal Stem Cells With Rhbmp-2 Inhibits The Growth of Canine Osteosarcoma Cellsvanessa_werbickyNo ratings yet
- Adhesion and Osteogenic Differentiation of Human Mesenchymal Stem Cells On Titanium NanoporesDocument13 pagesAdhesion and Osteogenic Differentiation of Human Mesenchymal Stem Cells On Titanium Nanoporesvanessa_werbickyNo ratings yet
- Istvan A. Urban, DMD, MD, PHD Alberto Monje, Dds Jaime L. Lozada, DMD Hom-Lay Wang, DDS, MSD, PHDDocument10 pagesIstvan A. Urban, DMD, MD, PHD Alberto Monje, Dds Jaime L. Lozada, DMD Hom-Lay Wang, DDS, MSD, PHDvanessa_werbickyNo ratings yet
- V-Belt DriveDocument9 pagesV-Belt DriveCHANDRASEKARANNo ratings yet
- Chapter 1Document43 pagesChapter 1Nour Aira NaoNo ratings yet
- Lexical Semantic Problems in TranslationDocument13 pagesLexical Semantic Problems in Translationvargas199511100% (2)
- Ral Colour ChartDocument7 pagesRal Colour ChartBoda CsabaNo ratings yet
- Diaphragm and Lung Ultrasound To Predict Weaning Outcome: Systematic Review and Meta-AnalysisDocument11 pagesDiaphragm and Lung Ultrasound To Predict Weaning Outcome: Systematic Review and Meta-AnalysisPablo IgnacioNo ratings yet
- SeptemberDocument119 pagesSeptemberThami KNo ratings yet
- JAMB English Language Past Questions and Answers 2010 - 2018Document84 pagesJAMB English Language Past Questions and Answers 2010 - 2018Joel Adams100% (6)
- Abon Sapi GloriaDocument1 pageAbon Sapi GloriaPratidina WulandariNo ratings yet
- ScrewCompressors XRV204 SpecSheet DigitalDocument1 pageScrewCompressors XRV204 SpecSheet DigitalBarros Arias EnriqueNo ratings yet
- 8 SWOT Analysis Tools For Small Businesses: 1. SmartsheetDocument3 pages8 SWOT Analysis Tools For Small Businesses: 1. SmartsheetSantu BiswaaNo ratings yet
- climateChangeStat2015 PDFDocument294 pagesclimateChangeStat2015 PDFPallaviNo ratings yet
- Excel Formulas ManualDocument8 pagesExcel Formulas ManualVidya NeemuNo ratings yet
- Arts 1ST Q Grade 9 ReviewerDocument6 pagesArts 1ST Q Grade 9 Reviewereri zen100% (1)
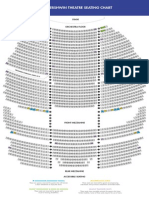
- The Gershwin Theatre Seating Chart: StageDocument1 pageThe Gershwin Theatre Seating Chart: StageCharles DavidsonNo ratings yet
- 4 PsDocument5 pages4 PsRaj Vardhan GaurNo ratings yet
- NY CREATES IBM Board PacketDocument2 pagesNY CREATES IBM Board PacketSean MickeyNo ratings yet
- 459 - So FG13Document5 pages459 - So FG13ronni gunadi sNo ratings yet
- Shared Information ModelDocument16 pagesShared Information Modelrohitchawandke100% (1)
- ArcUri - Organe de Masini OMDocument18 pagesArcUri - Organe de Masini OMCîrstea BökiNo ratings yet
- Individual Taxpayers Tax Filing ExercisesDocument3 pagesIndividual Taxpayers Tax Filing ExercisesKIM RAGANo ratings yet
- Invenia ABUS 2.0 Release Notes - UM - 4700-0044-00 - 4Document24 pagesInvenia ABUS 2.0 Release Notes - UM - 4700-0044-00 - 4Jawad SandhuNo ratings yet
- Sistemi Embedded AA 2012/2013: SOPC Design FlowDocument9 pagesSistemi Embedded AA 2012/2013: SOPC Design Flowmeseret sisayNo ratings yet
- Poliomyelitis: By: Reema I. DabbasDocument35 pagesPoliomyelitis: By: Reema I. DabbasReema DabbasNo ratings yet
- Inventory TheoryDocument18 pagesInventory TheoryIsaac LeeNo ratings yet
- Multiattribute Utility FunctionsDocument25 pagesMultiattribute Utility FunctionssilentNo ratings yet
- Jab Chem Nat 5 Question Banks All ExamsDocument55 pagesJab Chem Nat 5 Question Banks All ExamsHariNo ratings yet
- Phrasal Verb LESSON FINAL 1701874327225Document67 pagesPhrasal Verb LESSON FINAL 1701874327225bgt dfgNo ratings yet