Download as pdf or txt
You might also like
- National Health Strategy For Zimbabwe (2021 - 2025)Document104 pagesNational Health Strategy For Zimbabwe (2021 - 2025)Praise Nehumambi100% (6)
- RESNICK - Bone and Joint Imaging, 3rd Ed. CONTENIDODocument3 pagesRESNICK - Bone and Joint Imaging, 3rd Ed. CONTENIDOfabianNo ratings yet
- Breathing Terhadap Penurunan Respiratory Rate: Diajukan Sebagai Salah Satu Syarat Memperoleh Gelar Ners KeperawatanDocument31 pagesBreathing Terhadap Penurunan Respiratory Rate: Diajukan Sebagai Salah Satu Syarat Memperoleh Gelar Ners KeperawatanSri Susanti AbdulwahabNo ratings yet
- Post-Op (Terapetic Ex)Document3 pagesPost-Op (Terapetic Ex)黃子庭No ratings yet
- Week 6 DocsDocument18 pagesWeek 6 DocsSHERMINA HASANNo ratings yet
- File 3Document12 pagesFile 3Johanine VillasantiagoNo ratings yet
- Perioperative NursingDocument36 pagesPerioperative Nursinggrazelantonette.calubNo ratings yet
- Assignment of PTNDocument15 pagesAssignment of PTNSumandeep KaurNo ratings yet
- Perioperative NursingDocument18 pagesPerioperative NursingJhosita Flora LarocoNo ratings yet
- Fundamental of Nursing 3Document7 pagesFundamental of Nursing 3Atom AtomicNo ratings yet
- Nur 512 Tutorials Week 6 - 9Document42 pagesNur 512 Tutorials Week 6 - 9Katherine Vijeta karishma KumarNo ratings yet
- IntraoperativeDocument4 pagesIntraoperativeLynette Roldan RN100% (1)
- NCM 109 RLE OR TECHNIQUE F 3 Final OutputDocument74 pagesNCM 109 RLE OR TECHNIQUE F 3 Final OutputSunny100% (1)
- Perioperative NursingDocument2 pagesPerioperative NursingChin ChanNo ratings yet
- Introduction To SurgeryDocument7 pagesIntroduction To SurgeryinnocentsagemambweNo ratings yet
- Emergence and Postoperative Anesthetic Management: Prepared By: Serkalem Teshome Advised by Instructor WosneyelehDocument85 pagesEmergence and Postoperative Anesthetic Management: Prepared By: Serkalem Teshome Advised by Instructor WosneyelehagatakassaNo ratings yet
- IntraoperativeDocument10 pagesIntraoperativeIepunk ThokNo ratings yet
- Outline Perioperative NursingDocument8 pagesOutline Perioperative NursingMM VNo ratings yet
- Intraoperative Phase of SurgeryDocument8 pagesIntraoperative Phase of SurgeryCJ Thompson VanderpotNo ratings yet
- MS PeriopDocument4 pagesMS PeriopJinx GonNo ratings yet
- Adult 1 Test 1 Study GuideDocument9 pagesAdult 1 Test 1 Study GuideChristopher JamesNo ratings yet
- 7-Postoperative Care and ComplicationsDocument25 pages7-Postoperative Care and ComplicationsAiden JosephatNo ratings yet
- Postoperative Phase 2021Document56 pagesPostoperative Phase 2021Jmarie Brillantes PopiocoNo ratings yet
- Lecture 3 - Preoperative - Nursing Management - 2021-2022Document39 pagesLecture 3 - Preoperative - Nursing Management - 2021-2022عمار عاشورNo ratings yet
- Identify Common Postoperative Problems and Their ManagementDocument6 pagesIdentify Common Postoperative Problems and Their ManagementSilla, KyshiaNo ratings yet
- Aruna Ramesh Emergency...Document25 pagesAruna Ramesh Emergency...Aishu BNo ratings yet
- NURSING SCIENCE - Pre & Post Operative CareDocument61 pagesNURSING SCIENCE - Pre & Post Operative CareJiehah RudyNo ratings yet
- Perioperative Concepts and Nursing Management: NCM 112-LecturerDocument98 pagesPerioperative Concepts and Nursing Management: NCM 112-LecturerJaylord Verazon100% (1)
- Therapy After Injury To The HandDocument10 pagesTherapy After Injury To The HandPujia Cahya Amalia100% (1)
- Introduction To Perioperative NursingDocument19 pagesIntroduction To Perioperative NursingaidaelgamilNo ratings yet
- Distal Radius FractureDocument10 pagesDistal Radius Fracturemajiavik11No ratings yet
- Linee Guida KNGF Distorsione CavigliaDocument24 pagesLinee Guida KNGF Distorsione CavigliaRoberto TommasiniNo ratings yet
- Cts ArticlesDocument4 pagesCts ArticlesdrarunraoNo ratings yet
- Care of Surgical PatientsDocument79 pagesCare of Surgical PatientsyewollolijfikreNo ratings yet
- OET Sample Reading Test NewDocument22 pagesOET Sample Reading Test NewAHMED TANJIMUL ISLAM100% (3)
- NCPDocument10 pagesNCPbabycheska08No ratings yet
- Perioperative Nursing PhaseDocument80 pagesPerioperative Nursing PhaseMary Ann Sambo OgoyNo ratings yet
- MS Reviewer PrelimDocument23 pagesMS Reviewer PrelimCindy GeronimoNo ratings yet
- Practice Teaching On Pre and Post Op Nursing Care of Neurosurgery PatientsDocument15 pagesPractice Teaching On Pre and Post Op Nursing Care of Neurosurgery PatientsPriya SinghNo ratings yet
- General ConsiderationsDocument14 pagesGeneral ConsiderationsAudree BustamanteNo ratings yet
- Sas 2 Cabahug, Victoria Mae IDocument4 pagesSas 2 Cabahug, Victoria Mae Ibekbekk cabahugNo ratings yet
- Case-Scenario ElvinDocument3 pagesCase-Scenario ElvinKOBE TOMAGANNo ratings yet
- Post Op HandoutDocument3 pagesPost Op Handoutapi-28337695850% (2)
- Perioperative Care Definition and Three PhasesDocument1 pagePerioperative Care Definition and Three Phasesestical.23nick2No ratings yet
- Case Study On Head InjuryDocument15 pagesCase Study On Head InjuryPriya SinghNo ratings yet
- Preoperative PhaseDocument3 pagesPreoperative PhaseHans Dayag MallillinNo ratings yet
- Basic Patient NeedsDocument15 pagesBasic Patient NeedsMarggie SalaoNo ratings yet
- Damage Control Orthopaedics DR Bambang SpOT (Salinan Berkonflik Enggar Yusrina 2015-10-14)Document37 pagesDamage Control Orthopaedics DR Bambang SpOT (Salinan Berkonflik Enggar Yusrina 2015-10-14)SemestaNo ratings yet
- DR - Bambang-Damage Control OrthopaedicsDocument37 pagesDR - Bambang-Damage Control OrthopaedicsbadliinaaNo ratings yet
- NCPDocument17 pagesNCPShayne Jessemae AlmarioNo ratings yet
- Post-Op Teaching ProjectDocument18 pagesPost-Op Teaching Projectapi-283536133No ratings yet
- NCPDocument8 pagesNCPJose Benit DelacruzNo ratings yet
- Or Tho 4Document29 pagesOr Tho 4Maricar TaparNo ratings yet
- SURGERY For Nurses PDFDocument98 pagesSURGERY For Nurses PDFirene8000100% (1)
- Perioperative Nursing CareDocument17 pagesPerioperative Nursing CareMisikir Eyob100% (1)
- Week 2 Medical Surgical NursingDocument45 pagesWeek 2 Medical Surgical NursingKristel Anne100% (1)
- Perawatan Perioperatif 1Document72 pagesPerawatan Perioperatif 1Jesika VitamaniaNo ratings yet
- Perioperative Nursing: Prepared By: Annabeth K. Salonga RN, MANDocument67 pagesPerioperative Nursing: Prepared By: Annabeth K. Salonga RN, MANAnnabeth Kwong Salonga100% (2)
- Early Mobility Care GuidelineDocument7 pagesEarly Mobility Care GuidelineAny AndrianiNo ratings yet
- TÉCNICAS DEL AUXILIAR DE ENFERMERÍA EN EL ÁREA DE QUIRÓFANOFrom EverandTÉCNICAS DEL AUXILIAR DE ENFERMERÍA EN EL ÁREA DE QUIRÓFANONo ratings yet
- Primary Management of PolytraumaFrom EverandPrimary Management of PolytraumaSuk-Kyung HongNo ratings yet
- 04 Electrical Stimulation To Increase Functional ActivityDocument4 pages04 Electrical Stimulation To Increase Functional Activity楊畯凱No ratings yet
- Posterior, Lateral, and Anterior Hip Pain Due To Musculoskeletal OriginDocument4 pagesPosterior, Lateral, and Anterior Hip Pain Due To Musculoskeletal Origin楊畯凱No ratings yet
- 03 Principle of Electrical StimulationDocument5 pages03 Principle of Electrical Stimulation楊畯凱No ratings yet
- 09 Cervical Spine 1Document14 pages09 Cervical Spine 1楊畯凱No ratings yet
- 14 Emergency Sport AssessmentDocument7 pages14 Emergency Sport Assessment楊畯凱No ratings yet
- Shoulder Special TestDocument2 pagesShoulder Special Test楊畯凱No ratings yet
- 10 Thoracolumbar Spine 3Document4 pages10 Thoracolumbar Spine 3楊畯凱No ratings yet
- CHAPTER 23 Fatty Acid CatabolismDocument9 pagesCHAPTER 23 Fatty Acid Catabolism楊畯凱No ratings yet
- 02 Retraining Basic and Instrumental Activities of Daily LicingDocument5 pages02 Retraining Basic and Instrumental Activities of Daily Licing楊畯凱No ratings yet
- Shoe and Foot OrthosisDocument9 pagesShoe and Foot Orthosis楊畯凱No ratings yet
- 01 Musculoskeletal AssessmentDocument10 pages01 Musculoskeletal Assessment楊畯凱100% (1)
- Spinal OrthosisDocument6 pagesSpinal Orthosis楊畯凱No ratings yet
- KneeDocument10 pagesKnee楊畯凱No ratings yet
- Ankle Foot OrthosisDocument4 pagesAnkle Foot Orthosis楊畯凱No ratings yet
- CHAPTER 25 Nitrogen Acquisition and Amino Acid Metabolism I (Amino Acid Synthesis)Document12 pagesCHAPTER 25 Nitrogen Acquisition and Amino Acid Metabolism I (Amino Acid Synthesis)楊畯凱No ratings yet
- Knee and Hip OrthosisDocument4 pagesKnee and Hip Orthosis楊畯凱No ratings yet
- CHAPTER 24 Lipid BiosynthesisDocument16 pagesCHAPTER 24 Lipid Biosynthesis楊畯凱No ratings yet
- CHAPTER 22 Gluconeogenesis, Glycogen Metabolism, and The Pentose Phosphate PathwayDocument12 pagesCHAPTER 22 Gluconeogenesis, Glycogen Metabolism, and The Pentose Phosphate Pathway楊畯凱No ratings yet
- CHAPTER 21 PhotosynthesisDocument12 pagesCHAPTER 21 Photosynthesis楊畯凱No ratings yet
- CHAPTER 7 Carbohydrates and The Glyconjugates of Cell SurfaceDocument14 pagesCHAPTER 7 Carbohydrates and The Glyconjugates of Cell Surface楊畯凱No ratings yet
- CHAPTER 19 Tricarboxylic Acid CycleDocument11 pagesCHAPTER 19 Tricarboxylic Acid Cycle楊畯凱No ratings yet
- CHAPTER 17 The Metabolism An OverviewDocument10 pagesCHAPTER 17 The Metabolism An Overview楊畯凱No ratings yet
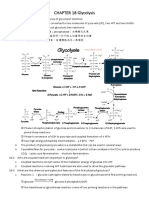
- CHAPTER 18 GlycolysisDocument10 pagesCHAPTER 18 Glycolysis楊畯凱No ratings yet
- Korelasi Faktor Demografi, Nutrisi Dan Antropometri Terhadap Kejadian Hipertensi Pada Petugas Keamanan Di Universitas Tarumanagara JakartaDocument16 pagesKorelasi Faktor Demografi, Nutrisi Dan Antropometri Terhadap Kejadian Hipertensi Pada Petugas Keamanan Di Universitas Tarumanagara JakartaMery Nurun rNo ratings yet
- Toolbox Talks: Hand Tool SafetyDocument1 pageToolbox Talks: Hand Tool Safetyserdar yücelNo ratings yet
- Application Status Granted Visa Conditions: Evisitor (Subclass 651)Document2 pagesApplication Status Granted Visa Conditions: Evisitor (Subclass 651)emmett PattenNo ratings yet
- OBGYN Notes - USMLE Step 2CKDocument107 pagesOBGYN Notes - USMLE Step 2CKDuncan89No ratings yet
- Bacterial Pneumonia - StatPearls - NCBI BookshelfDocument1 pageBacterial Pneumonia - StatPearls - NCBI BookshelfNang KhamNo ratings yet
- First Aid - NotesDocument10 pagesFirst Aid - NotesRoisin McdonnellNo ratings yet
- Heart Failure Guidelines For India Update 2017Document6 pagesHeart Failure Guidelines For India Update 2017Aditya SutarNo ratings yet
- Dr. Ashraf Sayeed: Department of OphthalmologyDocument49 pagesDr. Ashraf Sayeed: Department of Ophthalmologysaiful haque100% (1)
- Discourses On The Sober Life - How To Live 100 YearsDocument12 pagesDiscourses On The Sober Life - How To Live 100 YearsJacques HammanNo ratings yet
- AHW3e - Level 2 - Unit Test 8aDocument3 pagesAHW3e - Level 2 - Unit Test 8aDorian FarinangoNo ratings yet
- Icd 10 CM Pcs Coding Theory and Practice 2016 Edition 1st Edition Lovaasen Test BankDocument11 pagesIcd 10 CM Pcs Coding Theory and Practice 2016 Edition 1st Edition Lovaasen Test Bankgisellephongejs100% (42)
- Emp09 PDFDocument5 pagesEmp09 PDFKarthik SNo ratings yet
- 19-109 Putri Amalia CSS Radiologi PDFDocument20 pages19-109 Putri Amalia CSS Radiologi PDFPutri AmaliaNo ratings yet
- 3.2 Risk Rate Measures Cohort Studies PDFDocument3 pages3.2 Risk Rate Measures Cohort Studies PDFSherida GibbsNo ratings yet
- Therapeutic Ultrasound in Soft Tissue Lesions: ReviewDocument6 pagesTherapeutic Ultrasound in Soft Tissue Lesions: ReviewNgoma FaithNo ratings yet
- Aslo Si RFC MG Si ME 2017Document52 pagesAslo Si RFC MG Si ME 2017Mădă IorgaNo ratings yet
- CH12 DiagnosingDocument33 pagesCH12 DiagnosingAbod AshourNo ratings yet
- Test Bank For Medical Genetics 4th Edition Lynn B JordeDocument8 pagesTest Bank For Medical Genetics 4th Edition Lynn B Jorderoytuyenbau100% (1)
- College of Nursing: Cebu Normal UniversityDocument3 pagesCollege of Nursing: Cebu Normal UniversityLouie Danielle SegarraNo ratings yet
- Communicable Disease McqsDocument2 pagesCommunicable Disease McqsMuhammad AdilNo ratings yet
- Difference Between Community Health Nurse and A Public Health NurseDocument1 pageDifference Between Community Health Nurse and A Public Health NurseKim Angelo ReyesNo ratings yet
- Understanding Bile Acid DiarrheaDocument5 pagesUnderstanding Bile Acid DiarrheaAgastya Indian Martial ArtsNo ratings yet
- Wellness and Mental Health in 2020 Online LearningDocument4 pagesWellness and Mental Health in 2020 Online LearningClarissa BerganteNo ratings yet
- Sexton 2011Document19 pagesSexton 2011koushikNo ratings yet
- Ehad 883Document3 pagesEhad 883nhunhuochachNo ratings yet
- Mikrokolon & TerjemahanDocument35 pagesMikrokolon & Terjemahanizza mumtazatiNo ratings yet
- CS (Medical Attendance Rules) 1944: - Extent of ApplicationDocument50 pagesCS (Medical Attendance Rules) 1944: - Extent of ApplicationRohitKalraNo ratings yet