
UCAF 2.0: To Be Completed and ID Verified by The Reception/nurse: Print/Fill in Clear Letters or Emboss Card
UCAF 2.0: To Be Completed and ID Verified by The Reception/nurse: Print/Fill in Clear Letters or Emboss Card
You might also like
- UCAF 2.0: To Be Completed and ID Verified by The Reception/nurse: Print/Fill in Clear Letters or Emboss CardDocument2 pagesUCAF 2.0: To Be Completed and ID Verified by The Reception/nurse: Print/Fill in Clear Letters or Emboss Cardsohaibkhaled5858No ratings yet
- Contributor Eligibility: Welcome HOS261Document3 pagesContributor Eligibility: Welcome HOS261Structural EngineerNo ratings yet
- Printable Version - Approval Reference No - 8021555511Document2 pagesPrintable Version - Approval Reference No - 8021555511SalmanNo ratings yet
- Attachment MailDocument2 pagesAttachment MailQussai BitarNo ratings yet
- ANNYAADocument1 pageANNYAABay watchNo ratings yet
- ClaimForm GIC 145516000Document1 pageClaimForm GIC 145516000aymn iskandrNo ratings yet
- MSF008147722TMA CertificateDocument1 pageMSF008147722TMA CertificateHj Husain Hj RosleyNo ratings yet
- QLM Reimbursement Claim FormDocument1 pageQLM Reimbursement Claim FormMuhammad SaeedNo ratings yet
- Enquiry Details:: Bureau Name Response DetailsDocument4 pagesEnquiry Details:: Bureau Name Response DetailsRavinder singhNo ratings yet
- Invoice Gh00094427Document1 pageInvoice Gh00094427Ahmed GomaaNo ratings yet
- National Claim Form Primary Medical Care: Section A: Member Details (To Be Filled by The Insured Member)Document1 pageNational Claim Form Primary Medical Care: Section A: Member Details (To Be Filled by The Insured Member)Sundararajan PIVNo ratings yet
- Generate LOADocument1 pageGenerate LOAdead9122No ratings yet
- 2 FHPL 26042021 ProviderDocument3 pages2 FHPL 26042021 ProviderHOD (MVGR Civil)No ratings yet
- Billu Nayak PDFDocument3 pagesBillu Nayak PDFShaik Chand BashaNo ratings yet
- Service Is Referred To, Lemon Medical Pharmacy 76478727Document4 pagesService Is Referred To, Lemon Medical Pharmacy 76478727Mohamed NagyNo ratings yet
- Lemon Medical PharmacyDocument4 pagesLemon Medical PharmacyMohamed NagyNo ratings yet
- MP000011412KIAR11 Certificate PDFDocument2 pagesMP000011412KIAR11 Certificate PDFJayne Stalton RahmanNo ratings yet
- Printable Version - Approval Reference No - 60247630Document2 pagesPrintable Version - Approval Reference No - 60247630sohaibkhaled5858No ratings yet
- KoTTI APPLICATION FORM FOR ADMISSIONDocument2 pagesKoTTI APPLICATION FORM FOR ADMISSIONnicholaskoech56No ratings yet
- CheckMultipleDetails 2024 01 18 12 06 44Document8 pagesCheckMultipleDetails 2024 01 18 12 06 44hillumbertoNo ratings yet
- MSF010358722TMA CertificateDocument1 pageMSF010358722TMA CertificateHassan Hj AhmadNo ratings yet
- Sonam Preauth Approval LetterDocument3 pagesSonam Preauth Approval LetterVishu SinghNo ratings yet
- Elig 152568391Document1 pageElig 152568391alredhamuhamadNo ratings yet
- Explanation of BenefitsDocument1 pageExplanation of BenefitsKoky LabibNo ratings yet
- Backupnew PreAuthLetters ALIssuance 2023 PSU-OIC DEC 05-12-2023-17-35-27 6434664Document2 pagesBackupnew PreAuthLetters ALIssuance 2023 PSU-OIC DEC 05-12-2023-17-35-27 6434664abhieshek.roy1No ratings yet
- Takaful Musafir / Musafir Takaful Jadual / ScheduleDocument3 pagesTakaful Musafir / Musafir Takaful Jadual / ScheduleGee MuhamadNo ratings yet
- RejectedDocument2 pagesRejectedMohamed NagyNo ratings yet
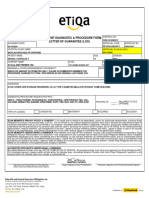
- Outpatient Diagnostic & Procedure Form Letter of Guarantee (Log)Document1 pageOutpatient Diagnostic & Procedure Form Letter of Guarantee (Log)selinaberina18No ratings yet
- Certificate of Insurance - Endorsed Copy Sarv Suraksha Plus (Group)Document4 pagesCertificate of Insurance - Endorsed Copy Sarv Suraksha Plus (Group)Ravi FrankNo ratings yet
- Pre-Import Permit: CommodityDocument3 pagesPre-Import Permit: Commoditychristina tetemkeNo ratings yet
- D2207D0017624Document2 pagesD2207D0017624Ana Rose NavarroNo ratings yet
- Eft # 211203740Document36 pagesEft # 211203740missansheNo ratings yet
- Ericson Insurance Tpa Pvt. Limited.: Cashless Authorization Letter (Part-D)Document3 pagesEricson Insurance Tpa Pvt. Limited.: Cashless Authorization Letter (Part-D)baladon 007No ratings yet
- private car insurance policyDocument3 pagesprivate car insurance policySharma General Insurance AdvisorNo ratings yet
- TVS LoanDocument20 pagesTVS LoanJOY CHERRYNo ratings yet
- PCSB OSP Application Form - Geostreamer - 1Document1 pagePCSB OSP Application Form - Geostreamer - 1jacek 11No ratings yet
- Insured & Vehicle Details: Product Code: 3001 UIN: IRDAN115P0017V01200102Document2 pagesInsured & Vehicle Details: Product Code: 3001 UIN: IRDAN115P0017V01200102Raman ParasharNo ratings yet
- SickLeaveCertificate With and Without Diagnosis 20231221 141430Document2 pagesSickLeaveCertificate With and Without Diagnosis 20231221 141430sr8670070No ratings yet
- PurnimaDocument1 pagePurnimaBeatriz Sophia BugayongNo ratings yet
- D2211D0017147Document2 pagesD2211D0017147marc bitangNo ratings yet
- CHRISTOPHERDocument2 pagesCHRISTOPHERChristopher MuriithiNo ratings yet
- 4010ip-03083292001 QTDocument4 pages4010ip-03083292001 QTMayank SharmaNo ratings yet
- Generate LOADocument1 pageGenerate LOAangel.domingo0309No ratings yet
- Cashless Authorization LetterDocument3 pagesCashless Authorization LetterJanakiraman BNo ratings yet
- Cana240224cr182853983 1Document9 pagesCana240224cr182853983 1VIJAY SHANKARNo ratings yet
- Statement of AccountsDocument9 pagesStatement of AccountsVinay NandedkarNo ratings yet
- BCBS - C23156e15895140Document31 pagesBCBS - C23156e15895140Business LoanNo ratings yet
- Statement of Account As On: 08 Jan 2022: 9563182959 Cust ID: 9013726141 Account / Folio NumberDocument2 pagesStatement of Account As On: 08 Jan 2022: 9563182959 Cust ID: 9013726141 Account / Folio NumberSubha DasNo ratings yet
- StatementOfAccount TCFTW0260000010725367 11 04 2024 11 55 49Document6 pagesStatementOfAccount TCFTW0260000010725367 11 04 2024 11 55 49smaheshwari816No ratings yet
- GUILLERMO T. PILI JR.-SI-PCV-500579648 - RN-500218633 - Schedule PDFDocument7 pagesGUILLERMO T. PILI JR.-SI-PCV-500579648 - RN-500218633 - Schedule PDFPearl JoyNo ratings yet
- Cancel Residence Inside UAE : Personal InformationDocument1 pageCancel Residence Inside UAE : Personal Informationlamaprajina213No ratings yet
- Statement of AccountsDocument3 pagesStatement of Accountsravinderkumar93060No ratings yet
- 1221 Profit Drive Dallas, TX 752473919 (972) 323-9393 Fax (214) 658-9051 NPI 1801181003Document3 pages1221 Profit Drive Dallas, TX 752473919 (972) 323-9393 Fax (214) 658-9051 NPI 1801181003kimNo ratings yet
- Backupnew PreAuthLetters ALIssuance 2022 SBIGI APR 28-04-2022-16-59-01 5456830Document2 pagesBackupnew PreAuthLetters ALIssuance 2022 SBIGI APR 28-04-2022-16-59-01 5456830MahanNo ratings yet
- Disbursement Voucher: DPWH-Sorsogon 1st DEODocument27 pagesDisbursement Voucher: DPWH-Sorsogon 1st DEOTIMMY BOYNo ratings yet
- The New India Assurance Co. Ltd. (Government of India Undertaking)Document2 pagesThe New India Assurance Co. Ltd. (Government of India Undertaking)rajib paulNo ratings yet
- SDFZDocument3 pagesSDFZShaik Chand BashaNo ratings yet
- Third Party Insurance - Shikhar - 1644994914.369046Document1 pageThird Party Insurance - Shikhar - 1644994914.369046soniyaranamagar6No ratings yet
- Understanding Named, Automatic and Additional Insureds in the CGL PolicyFrom EverandUnderstanding Named, Automatic and Additional Insureds in the CGL PolicyNo ratings yet
- A Guide to District Court Civil Forms in the State of HawaiiFrom EverandA Guide to District Court Civil Forms in the State of HawaiiNo ratings yet
- Hospital Management Da2Document4 pagesHospital Management Da2Anvita tadepalliNo ratings yet
- Renewal Mediclaim PolicyDocument8 pagesRenewal Mediclaim PolicychurmuriNo ratings yet
- Interprofessional Collaboration: Three Best Practice Models of Interprofessional EducationDocument5 pagesInterprofessional Collaboration: Three Best Practice Models of Interprofessional Educationna5649No ratings yet
- E-Health Management SystemDocument85 pagesE-Health Management Systemwalid youssefNo ratings yet
- Adult Patient Registration FormDocument7 pagesAdult Patient Registration FormTakpire DrMadhukarNo ratings yet
- Rights Regarding Classification and SeparationDocument28 pagesRights Regarding Classification and SeparationkvreddyNo ratings yet
- Sri Hariharan J 730617251050 (Thesis Synopsis - Super Speciality Hospital)Document5 pagesSri Hariharan J 730617251050 (Thesis Synopsis - Super Speciality Hospital)HàríShNo ratings yet
- 14 Patient Perceptions About CustomerDocument9 pages14 Patient Perceptions About CustomerAl AsyaryNo ratings yet
- Health Emergency Kits Training 2019 PDFDocument33 pagesHealth Emergency Kits Training 2019 PDFrema_rhere95No ratings yet
- Theory of Goal AttainmentDocument28 pagesTheory of Goal AttainmentparkaleenaNo ratings yet
- Communication ManualDocument6 pagesCommunication ManualGeofel Cutar AbejeroNo ratings yet
- Serenity: Violence, Inequality, and Recovery On The Edge of Mexico CityDocument18 pagesSerenity: Violence, Inequality, and Recovery On The Edge of Mexico CityE Panchi NuñezNo ratings yet
- Poster Template 20191206Document1 pagePoster Template 20191206api-402053549No ratings yet
- VHA NCPS Fall Prevention and ManagementDocument7 pagesVHA NCPS Fall Prevention and ManagementEvaNo ratings yet
- 84-Article Text-538-1-10-20201115Document54 pages84-Article Text-538-1-10-20201115Rubilin NitishaNo ratings yet
- Root Cause Analysis FrameworkDocument59 pagesRoot Cause Analysis Frameworkshridhar pandianNo ratings yet
- Tracer Study: Online Library of Quality, Service Improvement and Redesign ToolsDocument4 pagesTracer Study: Online Library of Quality, Service Improvement and Redesign ToolsSolomonNo ratings yet
- Steve M. Esteban RN, LPT, MSN, ManDocument39 pagesSteve M. Esteban RN, LPT, MSN, ManSteve Esteban100% (1)
- Dovercourt Surgery: 3 Skye Edge Avenue Sheffield S2 5FXDocument4 pagesDovercourt Surgery: 3 Skye Edge Avenue Sheffield S2 5FXsafasayedNo ratings yet
- Cna Med Tech ResumeDocument7 pagesCna Med Tech Resumeafiwhyber100% (2)
- Defining Staffing:: Workforce ManagementDocument33 pagesDefining Staffing:: Workforce ManagementMari FeNo ratings yet
- Hyposkillia: Guest EditorialDocument3 pagesHyposkillia: Guest EditorialRenan BragaNo ratings yet
- 756 AfghanistanHealthInsuranceFeasibilitFINAL PDFDocument118 pages756 AfghanistanHealthInsuranceFeasibilitFINAL PDFbejarhasanNo ratings yet
- Strategi Operasi RUmah SakitDocument4 pagesStrategi Operasi RUmah SakituddindjmNo ratings yet
- Binder 7Document20 pagesBinder 7Anonymous 2yVesLNo ratings yet
- United Healthcare CA Select Plus Silver 30 2000 30 Aksa W 405Document8 pagesUnited Healthcare CA Select Plus Silver 30 2000 30 Aksa W 405zxcvNo ratings yet
- Compassion and Choices Mag Fall 2014Document23 pagesCompassion and Choices Mag Fall 2014Matthew LloydNo ratings yet
- Clinical Guide GIP VersionDocument22 pagesClinical Guide GIP Versionsireesha gandrotuNo ratings yet
- Patient Classification System and Assignment of PatientsDocument25 pagesPatient Classification System and Assignment of PatientsStephy Sojan100% (3)
- Death From Orange PithDocument1 pageDeath From Orange PithMwagaVumbiNo ratings yet






















































































Download as pdf or txt
You might also like
- UCAF 2.0: To Be Completed and ID Verified by The Reception/nurse: Print/Fill in Clear Letters or Emboss CardDocument2 pagesUCAF 2.0: To Be Completed and ID Verified by The Reception/nurse: Print/Fill in Clear Letters or Emboss Cardsohaibkhaled5858No ratings yet
- Contributor Eligibility: Welcome HOS261Document3 pagesContributor Eligibility: Welcome HOS261Structural EngineerNo ratings yet
- Printable Version - Approval Reference No - 8021555511Document2 pagesPrintable Version - Approval Reference No - 8021555511SalmanNo ratings yet
- Attachment MailDocument2 pagesAttachment MailQussai BitarNo ratings yet
- ANNYAADocument1 pageANNYAABay watchNo ratings yet
- ClaimForm GIC 145516000Document1 pageClaimForm GIC 145516000aymn iskandrNo ratings yet
- MSF008147722TMA CertificateDocument1 pageMSF008147722TMA CertificateHj Husain Hj RosleyNo ratings yet
- QLM Reimbursement Claim FormDocument1 pageQLM Reimbursement Claim FormMuhammad SaeedNo ratings yet
- Enquiry Details:: Bureau Name Response DetailsDocument4 pagesEnquiry Details:: Bureau Name Response DetailsRavinder singhNo ratings yet
- Invoice Gh00094427Document1 pageInvoice Gh00094427Ahmed GomaaNo ratings yet
- National Claim Form Primary Medical Care: Section A: Member Details (To Be Filled by The Insured Member)Document1 pageNational Claim Form Primary Medical Care: Section A: Member Details (To Be Filled by The Insured Member)Sundararajan PIVNo ratings yet
- Generate LOADocument1 pageGenerate LOAdead9122No ratings yet
- 2 FHPL 26042021 ProviderDocument3 pages2 FHPL 26042021 ProviderHOD (MVGR Civil)No ratings yet
- Billu Nayak PDFDocument3 pagesBillu Nayak PDFShaik Chand BashaNo ratings yet
- Service Is Referred To, Lemon Medical Pharmacy 76478727Document4 pagesService Is Referred To, Lemon Medical Pharmacy 76478727Mohamed NagyNo ratings yet
- Lemon Medical PharmacyDocument4 pagesLemon Medical PharmacyMohamed NagyNo ratings yet
- MP000011412KIAR11 Certificate PDFDocument2 pagesMP000011412KIAR11 Certificate PDFJayne Stalton RahmanNo ratings yet
- Printable Version - Approval Reference No - 60247630Document2 pagesPrintable Version - Approval Reference No - 60247630sohaibkhaled5858No ratings yet
- KoTTI APPLICATION FORM FOR ADMISSIONDocument2 pagesKoTTI APPLICATION FORM FOR ADMISSIONnicholaskoech56No ratings yet
- CheckMultipleDetails 2024 01 18 12 06 44Document8 pagesCheckMultipleDetails 2024 01 18 12 06 44hillumbertoNo ratings yet
- MSF010358722TMA CertificateDocument1 pageMSF010358722TMA CertificateHassan Hj AhmadNo ratings yet
- Sonam Preauth Approval LetterDocument3 pagesSonam Preauth Approval LetterVishu SinghNo ratings yet
- Elig 152568391Document1 pageElig 152568391alredhamuhamadNo ratings yet
- Explanation of BenefitsDocument1 pageExplanation of BenefitsKoky LabibNo ratings yet
- Backupnew PreAuthLetters ALIssuance 2023 PSU-OIC DEC 05-12-2023-17-35-27 6434664Document2 pagesBackupnew PreAuthLetters ALIssuance 2023 PSU-OIC DEC 05-12-2023-17-35-27 6434664abhieshek.roy1No ratings yet
- Takaful Musafir / Musafir Takaful Jadual / ScheduleDocument3 pagesTakaful Musafir / Musafir Takaful Jadual / ScheduleGee MuhamadNo ratings yet
- RejectedDocument2 pagesRejectedMohamed NagyNo ratings yet
- Outpatient Diagnostic & Procedure Form Letter of Guarantee (Log)Document1 pageOutpatient Diagnostic & Procedure Form Letter of Guarantee (Log)selinaberina18No ratings yet
- Certificate of Insurance - Endorsed Copy Sarv Suraksha Plus (Group)Document4 pagesCertificate of Insurance - Endorsed Copy Sarv Suraksha Plus (Group)Ravi FrankNo ratings yet
- Pre-Import Permit: CommodityDocument3 pagesPre-Import Permit: Commoditychristina tetemkeNo ratings yet
- D2207D0017624Document2 pagesD2207D0017624Ana Rose NavarroNo ratings yet
- Eft # 211203740Document36 pagesEft # 211203740missansheNo ratings yet
- Ericson Insurance Tpa Pvt. Limited.: Cashless Authorization Letter (Part-D)Document3 pagesEricson Insurance Tpa Pvt. Limited.: Cashless Authorization Letter (Part-D)baladon 007No ratings yet
- private car insurance policyDocument3 pagesprivate car insurance policySharma General Insurance AdvisorNo ratings yet
- TVS LoanDocument20 pagesTVS LoanJOY CHERRYNo ratings yet
- PCSB OSP Application Form - Geostreamer - 1Document1 pagePCSB OSP Application Form - Geostreamer - 1jacek 11No ratings yet
- Insured & Vehicle Details: Product Code: 3001 UIN: IRDAN115P0017V01200102Document2 pagesInsured & Vehicle Details: Product Code: 3001 UIN: IRDAN115P0017V01200102Raman ParasharNo ratings yet
- SickLeaveCertificate With and Without Diagnosis 20231221 141430Document2 pagesSickLeaveCertificate With and Without Diagnosis 20231221 141430sr8670070No ratings yet
- PurnimaDocument1 pagePurnimaBeatriz Sophia BugayongNo ratings yet
- D2211D0017147Document2 pagesD2211D0017147marc bitangNo ratings yet
- CHRISTOPHERDocument2 pagesCHRISTOPHERChristopher MuriithiNo ratings yet
- 4010ip-03083292001 QTDocument4 pages4010ip-03083292001 QTMayank SharmaNo ratings yet
- Generate LOADocument1 pageGenerate LOAangel.domingo0309No ratings yet
- Cashless Authorization LetterDocument3 pagesCashless Authorization LetterJanakiraman BNo ratings yet
- Cana240224cr182853983 1Document9 pagesCana240224cr182853983 1VIJAY SHANKARNo ratings yet
- Statement of AccountsDocument9 pagesStatement of AccountsVinay NandedkarNo ratings yet
- BCBS - C23156e15895140Document31 pagesBCBS - C23156e15895140Business LoanNo ratings yet
- Statement of Account As On: 08 Jan 2022: 9563182959 Cust ID: 9013726141 Account / Folio NumberDocument2 pagesStatement of Account As On: 08 Jan 2022: 9563182959 Cust ID: 9013726141 Account / Folio NumberSubha DasNo ratings yet
- StatementOfAccount TCFTW0260000010725367 11 04 2024 11 55 49Document6 pagesStatementOfAccount TCFTW0260000010725367 11 04 2024 11 55 49smaheshwari816No ratings yet
- GUILLERMO T. PILI JR.-SI-PCV-500579648 - RN-500218633 - Schedule PDFDocument7 pagesGUILLERMO T. PILI JR.-SI-PCV-500579648 - RN-500218633 - Schedule PDFPearl JoyNo ratings yet
- Cancel Residence Inside UAE : Personal InformationDocument1 pageCancel Residence Inside UAE : Personal Informationlamaprajina213No ratings yet
- Statement of AccountsDocument3 pagesStatement of Accountsravinderkumar93060No ratings yet
- 1221 Profit Drive Dallas, TX 752473919 (972) 323-9393 Fax (214) 658-9051 NPI 1801181003Document3 pages1221 Profit Drive Dallas, TX 752473919 (972) 323-9393 Fax (214) 658-9051 NPI 1801181003kimNo ratings yet
- Backupnew PreAuthLetters ALIssuance 2022 SBIGI APR 28-04-2022-16-59-01 5456830Document2 pagesBackupnew PreAuthLetters ALIssuance 2022 SBIGI APR 28-04-2022-16-59-01 5456830MahanNo ratings yet
- Disbursement Voucher: DPWH-Sorsogon 1st DEODocument27 pagesDisbursement Voucher: DPWH-Sorsogon 1st DEOTIMMY BOYNo ratings yet
- The New India Assurance Co. Ltd. (Government of India Undertaking)Document2 pagesThe New India Assurance Co. Ltd. (Government of India Undertaking)rajib paulNo ratings yet
- SDFZDocument3 pagesSDFZShaik Chand BashaNo ratings yet
- Third Party Insurance - Shikhar - 1644994914.369046Document1 pageThird Party Insurance - Shikhar - 1644994914.369046soniyaranamagar6No ratings yet
- Understanding Named, Automatic and Additional Insureds in the CGL PolicyFrom EverandUnderstanding Named, Automatic and Additional Insureds in the CGL PolicyNo ratings yet
- A Guide to District Court Civil Forms in the State of HawaiiFrom EverandA Guide to District Court Civil Forms in the State of HawaiiNo ratings yet
- Hospital Management Da2Document4 pagesHospital Management Da2Anvita tadepalliNo ratings yet
- Renewal Mediclaim PolicyDocument8 pagesRenewal Mediclaim PolicychurmuriNo ratings yet
- Interprofessional Collaboration: Three Best Practice Models of Interprofessional EducationDocument5 pagesInterprofessional Collaboration: Three Best Practice Models of Interprofessional Educationna5649No ratings yet
- E-Health Management SystemDocument85 pagesE-Health Management Systemwalid youssefNo ratings yet
- Adult Patient Registration FormDocument7 pagesAdult Patient Registration FormTakpire DrMadhukarNo ratings yet
- Rights Regarding Classification and SeparationDocument28 pagesRights Regarding Classification and SeparationkvreddyNo ratings yet
- Sri Hariharan J 730617251050 (Thesis Synopsis - Super Speciality Hospital)Document5 pagesSri Hariharan J 730617251050 (Thesis Synopsis - Super Speciality Hospital)HàríShNo ratings yet
- 14 Patient Perceptions About CustomerDocument9 pages14 Patient Perceptions About CustomerAl AsyaryNo ratings yet
- Health Emergency Kits Training 2019 PDFDocument33 pagesHealth Emergency Kits Training 2019 PDFrema_rhere95No ratings yet
- Theory of Goal AttainmentDocument28 pagesTheory of Goal AttainmentparkaleenaNo ratings yet
- Communication ManualDocument6 pagesCommunication ManualGeofel Cutar AbejeroNo ratings yet
- Serenity: Violence, Inequality, and Recovery On The Edge of Mexico CityDocument18 pagesSerenity: Violence, Inequality, and Recovery On The Edge of Mexico CityE Panchi NuñezNo ratings yet
- Poster Template 20191206Document1 pagePoster Template 20191206api-402053549No ratings yet
- VHA NCPS Fall Prevention and ManagementDocument7 pagesVHA NCPS Fall Prevention and ManagementEvaNo ratings yet
- 84-Article Text-538-1-10-20201115Document54 pages84-Article Text-538-1-10-20201115Rubilin NitishaNo ratings yet
- Root Cause Analysis FrameworkDocument59 pagesRoot Cause Analysis Frameworkshridhar pandianNo ratings yet
- Tracer Study: Online Library of Quality, Service Improvement and Redesign ToolsDocument4 pagesTracer Study: Online Library of Quality, Service Improvement and Redesign ToolsSolomonNo ratings yet
- Steve M. Esteban RN, LPT, MSN, ManDocument39 pagesSteve M. Esteban RN, LPT, MSN, ManSteve Esteban100% (1)
- Dovercourt Surgery: 3 Skye Edge Avenue Sheffield S2 5FXDocument4 pagesDovercourt Surgery: 3 Skye Edge Avenue Sheffield S2 5FXsafasayedNo ratings yet
- Cna Med Tech ResumeDocument7 pagesCna Med Tech Resumeafiwhyber100% (2)
- Defining Staffing:: Workforce ManagementDocument33 pagesDefining Staffing:: Workforce ManagementMari FeNo ratings yet
- Hyposkillia: Guest EditorialDocument3 pagesHyposkillia: Guest EditorialRenan BragaNo ratings yet
- 756 AfghanistanHealthInsuranceFeasibilitFINAL PDFDocument118 pages756 AfghanistanHealthInsuranceFeasibilitFINAL PDFbejarhasanNo ratings yet
- Strategi Operasi RUmah SakitDocument4 pagesStrategi Operasi RUmah SakituddindjmNo ratings yet
- Binder 7Document20 pagesBinder 7Anonymous 2yVesLNo ratings yet
- United Healthcare CA Select Plus Silver 30 2000 30 Aksa W 405Document8 pagesUnited Healthcare CA Select Plus Silver 30 2000 30 Aksa W 405zxcvNo ratings yet
- Compassion and Choices Mag Fall 2014Document23 pagesCompassion and Choices Mag Fall 2014Matthew LloydNo ratings yet
- Clinical Guide GIP VersionDocument22 pagesClinical Guide GIP Versionsireesha gandrotuNo ratings yet
- Patient Classification System and Assignment of PatientsDocument25 pagesPatient Classification System and Assignment of PatientsStephy Sojan100% (3)
- Death From Orange PithDocument1 pageDeath From Orange PithMwagaVumbiNo ratings yet