Download as pdf or txt
You might also like
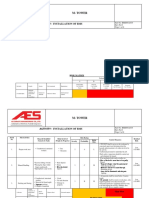
- Risk Assessment For Installation of BMS M Tower PDFDocument15 pagesRisk Assessment For Installation of BMS M Tower PDFAndrew HivNo ratings yet
- Steri ZL IzationDocument19 pagesSteri ZL Izationأبو محمدNo ratings yet
- Swing TradingDocument12 pagesSwing TradingAalon Sheikh71% (24)
- Armamentarium and Sterilization 2Document40 pagesArmamentarium and Sterilization 2EISHA ABRARNo ratings yet
- Sterilization and DisinfectionDocument48 pagesSterilization and DisinfectionBharanija100% (2)
- My SeminarDocument52 pagesMy SeminarvinnycoolbuddyNo ratings yet
- Sterallization and Disinfection-1Document50 pagesSterallization and Disinfection-1Sadam Hussain MagsiNo ratings yet
- Mrs. Tole S.B. Asst. Prof. K.T.Patil College of Pharmacy, OsmanabadDocument56 pagesMrs. Tole S.B. Asst. Prof. K.T.Patil College of Pharmacy, OsmanabadShobha ToleNo ratings yet
- ZahidDocument38 pagesZahidZahid Yaseen MirNo ratings yet
- Sterilization in OrthodonticsDocument32 pagesSterilization in OrthodonticsLeo JuniorNo ratings yet
- 2 Sterilization &disinfectionDocument73 pages2 Sterilization &disinfectionali tiwanaNo ratings yet
- SteDis - HospWMDocument68 pagesSteDis - HospWMArvinth Guna SegaranNo ratings yet
- Sterilization and Asepsis Oral SurgeryDocument15 pagesSterilization and Asepsis Oral SurgeryFourthMolar.comNo ratings yet
- 09 Sterilization PDFDocument34 pages09 Sterilization PDFDian NurdianaNo ratings yet
- Disinfection and Sterilization Lecture NotesDocument36 pagesDisinfection and Sterilization Lecture Notesminenhle ngcongoNo ratings yet
- Sterlization Procedures and DisinfectionDocument36 pagesSterlization Procedures and DisinfectionHarshinie AudimulamNo ratings yet
- Sterilisation and DisinfectionDocument121 pagesSterilisation and DisinfectionSreelekshmi JNo ratings yet
- Sterilization in OperativeDocument31 pagesSterilization in OperativehaithemNo ratings yet
- SterilizationDocument50 pagesSterilizationSafoora TariqNo ratings yet
- Sterilisation MBDocument9 pagesSterilisation MBWaliNo ratings yet
- 5.IP Sterilization Part 5Document24 pages5.IP Sterilization Part 5fatoman469No ratings yet
- Chapter 4 - Systems in HospitalsDocument40 pagesChapter 4 - Systems in Hospitalsmarye agegnNo ratings yet
- Sterilization and DisinfectionDocument137 pagesSterilization and Disinfectionitsme543210No ratings yet
- Lecture # 6 Physical Methods: Mentor Aleena Khan, Lecturer College of Nursing, IslamabadDocument31 pagesLecture # 6 Physical Methods: Mentor Aleena Khan, Lecturer College of Nursing, IslamabadAbdur RehmanNo ratings yet
- Sterlization by DR WajidDocument38 pagesSterlization by DR Wajidsagarsajnani15No ratings yet
- Sterilization: LecturerDocument16 pagesSterilization: Lecturerمظفر يوسف رشمNo ratings yet
- Sterlization and Disinfecti For ParamedicalDocument122 pagesSterlization and Disinfecti For ParamedicalanshikakathairiaNo ratings yet
- 2 SterilizationDocument32 pages2 SterilizationUmme RubabNo ratings yet
- Sepsis and AsepsisDocument53 pagesSepsis and AsepsisSANANo ratings yet
- Sterilizationprocess 190907172803Document70 pagesSterilizationprocess 190907172803TanurajNo ratings yet
- Sterilization DRNDocument61 pagesSterilization DRNdr.sujathaNo ratings yet
- Sterilization and DisinfectionDocument8 pagesSterilization and Disinfectionزين العابدين محمد عويش مشريNo ratings yet
- Surgical Preparation: Lobna El FikyDocument51 pagesSurgical Preparation: Lobna El FikyMayursinh SolankiNo ratings yet
- Disinfection and SterilizationDocument48 pagesDisinfection and SterilizationShriefElghazalyNo ratings yet
- Lecture 1 Asepsis and AntisepsisDocument47 pagesLecture 1 Asepsis and AntisepsisAmir KhanNo ratings yet
- Sterilization مضغوطDocument34 pagesSterilization مضغوطtaiif4678No ratings yet
- Sterilization & DisinfectionDocument27 pagesSterilization & DisinfectionmisdduaaNo ratings yet
- Sterilization and DisinfectionDocument78 pagesSterilization and DisinfectionMuhammad Shoaib50% (2)
- Sterilization - Principles - Physical and Chemical Methods Sterilization - Principles - Physical and Chemical MethodsDocument64 pagesSterilization - Principles - Physical and Chemical Methods Sterilization - Principles - Physical and Chemical MethodsSELVI ANo ratings yet
- Industrial MicrobiologyDocument121 pagesIndustrial Microbiologyarbazsabir88No ratings yet
- 09 SterilizationDocument34 pages09 Sterilizationitung2350% (2)
- SterilizationDocument4 pagesSterilizationMaheshwar MukkaNo ratings yet
- Infection Control in Restorative DentistryDocument32 pagesInfection Control in Restorative Dentistryjamaica faith ramonNo ratings yet
- Sterilization and DisinfectionDocument27 pagesSterilization and DisinfectionAtikah0% (1)
- Jammu Dental PresentationDocument51 pagesJammu Dental PresentationJaswant Singh DhonsiNo ratings yet
- Course-M.Sc. Botany Part - II Paper - XVI Topic - Methods of Sterilization (Biotechnology & Bioinformatics)Document11 pagesCourse-M.Sc. Botany Part - II Paper - XVI Topic - Methods of Sterilization (Biotechnology & Bioinformatics)Sidrah ParkarNo ratings yet
- Microbiology Ii - Lecture Ii-1Document14 pagesMicrobiology Ii - Lecture Ii-1Cosmos OcranNo ratings yet
- Bacte All MergedDocument78 pagesBacte All MergedShin DongzalNo ratings yet
- SterilizationDocument27 pagesSterilizationSmriti Grover100% (1)
- Lec 3 Part 2Document4 pagesLec 3 Part 2Ahmed JamalNo ratings yet
- Cleaning, Disinfection & Sterilisation For IPCCDocument99 pagesCleaning, Disinfection & Sterilisation For IPCCJyotiNo ratings yet
- Sterilization 2014Document18 pagesSterilization 2014Keith OmwoyoNo ratings yet
- SterilizationDocument41 pagesSterilizationharini meenakshiNo ratings yet
- Presentation On AsepsisDocument40 pagesPresentation On Asepsiskiran pandeyNo ratings yet
- Instrument ProcessingDocument22 pagesInstrument ProcessingJheannel Khriztine LadeNo ratings yet
- Teknik Sterilisasi Alat Dan Bahan (English Ver)Document18 pagesTeknik Sterilisasi Alat Dan Bahan (English Ver)Ani NurHidayantiNo ratings yet
- Microbial ControlDocument43 pagesMicrobial ControlAyman ElsirNo ratings yet
- Sterilisation Newppt1Document58 pagesSterilisation Newppt1priscillabaidoo.paNo ratings yet
- Disinfection & Sterilization: DR: Dina RamadanDocument26 pagesDisinfection & Sterilization: DR: Dina RamadanSudheer RevanthNo ratings yet
- Disinfection Sterilization 2Document15 pagesDisinfection Sterilization 2Ãbdi TefNo ratings yet
- Sterlization and DisinfectionDocument20 pagesSterlization and Disinfectionshagun singh100% (1)
- 5 - 6255737462828565350 (10 Files Merged)Document307 pages5 - 6255737462828565350 (10 Files Merged)Aman PalNo ratings yet
- Experiment 6 Kirchhoff and PowerDocument13 pagesExperiment 6 Kirchhoff and PowerVenus IlaganNo ratings yet
- Design of CylinderDocument14 pagesDesign of CylinderRushikesh BhatkarNo ratings yet
- ScriptDocument1 pageScriptstar trendzNo ratings yet
- Nazi Germany Resource SampleDocument7 pagesNazi Germany Resource SampleIrram RanaNo ratings yet
- Handbook - Calculations 2Document1 pageHandbook - Calculations 2Smith SivaNo ratings yet
- Occupational Health and Safety Management PlanDocument216 pagesOccupational Health and Safety Management PlanMaung MyintNo ratings yet
- Lab - Fossil EvidenceDocument3 pagesLab - Fossil Evidenceapi-223694170No ratings yet
- Examen de NES Inglés B - APROBADODocument12 pagesExamen de NES Inglés B - APROBADOJuanMa DiazNo ratings yet
- 1987-2007 AL-Econ-Micro-Past Paper (Sorted in Topics)Document311 pages1987-2007 AL-Econ-Micro-Past Paper (Sorted in Topics)Sky Xing100% (2)
- Elementary Differential Equations and Boundary Value Problems, 11th EditionDocument1 pageElementary Differential Equations and Boundary Value Problems, 11th EditionPatriot NJROTC0% (1)
- Merger of HDFC and Centurion Bank of PunjabDocument2 pagesMerger of HDFC and Centurion Bank of Punjabanant ashwaryaNo ratings yet
- Rizal SyllabusDocument10 pagesRizal SyllabusLeslie S. AndresNo ratings yet
- CC55Document21 pagesCC55azhar saddiqNo ratings yet
- What Is Bacteria - What Are BacteriaDocument15 pagesWhat Is Bacteria - What Are BacteriaFernando OssNo ratings yet
- Environmental Awareness QuotesDocument21 pagesEnvironmental Awareness QuotesJaveed AktharNo ratings yet
- Symmetry: He Quality of Being Made Up of Exactly Similar Parts Facing Each Other or Around An AxisDocument3 pagesSymmetry: He Quality of Being Made Up of Exactly Similar Parts Facing Each Other or Around An AxisJubelle Mae Batalla RentuzaNo ratings yet
- 2n Quarter SCIENCE 8 - Quiz 2Document2 pages2n Quarter SCIENCE 8 - Quiz 2Jerwin Canteras100% (1)
- Monitoring Tool For Functional School ClinicDocument5 pagesMonitoring Tool For Functional School ClinicYatts De La Cuesta100% (1)
- Cam Band Assembly: Lacing Webbing Bands Through Scuba Cam BucklesDocument10 pagesCam Band Assembly: Lacing Webbing Bands Through Scuba Cam BuckleshdhdhdNo ratings yet
- Online Signature Verification Using Dynamic Time WarpingDocument5 pagesOnline Signature Verification Using Dynamic Time Warpingapi-3837813No ratings yet
- Clamp-On Ground Resistance Testing: Fall 2008 NETA WORLDDocument4 pagesClamp-On Ground Resistance Testing: Fall 2008 NETA WORLDAnonymous utxGVB5VyNo ratings yet
- Hs DiagramDocument32 pagesHs DiagramsubratorajNo ratings yet
- Shantanu KumarDocument4 pagesShantanu KumarPiyush AgarwalNo ratings yet
- Refrigeration P&ID)Document3 pagesRefrigeration P&ID)ratheesh0% (1)
- Thin Layer Chromatography (TLC) PDFDocument11 pagesThin Layer Chromatography (TLC) PDFValeriaCusumanoNo ratings yet
- A Pizza: English Teacher: Nole Geraldo RiveraDocument2 pagesA Pizza: English Teacher: Nole Geraldo RiveraJazmin Brigid Perales CarranzaNo ratings yet
- DVB RodmDocument2 pagesDVB RodmAnanda BhattacharyyaNo ratings yet