
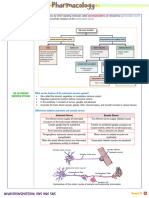
Introduction To Ans
Introduction To Ans
You might also like
- NASM CPT Study Guide - 7th EditionDocument22 pagesNASM CPT Study Guide - 7th Editionlatifa100% (3)
- Dr. Azam Anatomy NLC Notes For Dec 2021 ExamDocument134 pagesDr. Azam Anatomy NLC Notes For Dec 2021 ExamCastleKG100% (4)
- Fish Sauce ProductionDocument44 pagesFish Sauce ProductionTHANH PHẠM KIM NGUYỆT100% (1)
- Onion Root Tip MitosisDocument5 pagesOnion Root Tip MitosisNor Ashikin IsmailNo ratings yet
- Mock Tests 20 20 Class 4 Science SampleDocument13 pagesMock Tests 20 20 Class 4 Science SampleRueban manohar75% (4)
- (See Next Diagram) : Autonomic Nervous System Rashelle Lopez-Salvatierra, MD Somatic DivisionDocument7 pages(See Next Diagram) : Autonomic Nervous System Rashelle Lopez-Salvatierra, MD Somatic Divisionemely p. tango100% (4)
- Pharma - Neurotransmission Ans and SnsDocument10 pagesPharma - Neurotransmission Ans and SnsksescletoNo ratings yet
- Biology NotesDocument102 pagesBiology Notesajabgul123493No ratings yet
- Professor of Anatomy Dept. of Biomedical Sciences Heritage College of Osteopathic Medicine, Ohio University Athens, Ohio 45701 Witmerl@Ohio - EduDocument20 pagesProfessor of Anatomy Dept. of Biomedical Sciences Heritage College of Osteopathic Medicine, Ohio University Athens, Ohio 45701 Witmerl@Ohio - EduAri SudarsonoNo ratings yet
- Autonomic Nervous SystemDocument68 pagesAutonomic Nervous SystemTahir AzizNo ratings yet
- Autonomic and Systemic Pharmacology DR DahalDocument119 pagesAutonomic and Systemic Pharmacology DR Dahalअविनाश भाल्टरNo ratings yet
- The SNS and ANS Share Afferent Neurons: Autonomic Nervous SystemDocument5 pagesThe SNS and ANS Share Afferent Neurons: Autonomic Nervous SystemIshani ManivannanNo ratings yet
- 8 - Autonomic Nervous SystemDocument23 pages8 - Autonomic Nervous SystemibhaslauraNo ratings yet
- Anatomy ANSDocument8 pagesAnatomy ANSashim tiwariNo ratings yet
- Autonomic NSDocument9 pagesAutonomic NSsanyamana935No ratings yet
- Autonomic Nervous SystemDocument20 pagesAutonomic Nervous SystemArian May MarcosNo ratings yet
- Unit 2 - Nervous SystemDocument49 pagesUnit 2 - Nervous SystemAbdullah MohammedNo ratings yet
- 1st SemDocument158 pages1st SemSana chaudharyNo ratings yet
- 2023.neuroscience - Trans14.autonomic Nervous SystemDocument13 pages2023.neuroscience - Trans14.autonomic Nervous SystemstellaNo ratings yet
- Slide Deck 4 - ANSDocument21 pagesSlide Deck 4 - ANSCharlotte KalilecNo ratings yet
- Neuroanatomy: Autonomic Nervous System Dr. Antonio T. Parong JRDocument10 pagesNeuroanatomy: Autonomic Nervous System Dr. Antonio T. Parong JRZllison Mae Teodoro MangabatNo ratings yet
- Module 5 - 14. Ans NotesDocument6 pagesModule 5 - 14. Ans Notesjieannfaith.ausmolo-20No ratings yet
- St. Luke's College of Medicine - William H. Quasha Memorial: PhysiologyDocument6 pagesSt. Luke's College of Medicine - William H. Quasha Memorial: PhysiologyMavic Villanueva100% (1)
- Autonomic Nervous SystemDocument49 pagesAutonomic Nervous SystemAzmi PlusNo ratings yet
- Autonomic Nervous SystemDocument41 pagesAutonomic Nervous SystemYanto HaryantoNo ratings yet
- Basic Bladder NeurophysiologyDocument8 pagesBasic Bladder Neurophysiologylinda margaritaNo ratings yet
- Autonomic Nervous SystemDocument50 pagesAutonomic Nervous SystemEbti Rizki UtamiNo ratings yet
- CHAPTER 8, Neurotransmission - The Autonomic and Somatic Motor Nervous SystemDocument15 pagesCHAPTER 8, Neurotransmission - The Autonomic and Somatic Motor Nervous SystemoreaNo ratings yet
- Control and Coordination PDFDocument24 pagesControl and Coordination PDFMUZEER PASHANo ratings yet
- ICSE Biology Notes Nervous System For 20 PDFDocument25 pagesICSE Biology Notes Nervous System For 20 PDFMmt RdcNo ratings yet
- Study Guide 5Document39 pagesStudy Guide 5Amina Rose AlghamdiNo ratings yet
- Central - Peripheral Nervous SystemDocument82 pagesCentral - Peripheral Nervous System52-nur Fadiyyah FNo ratings yet
- The Autonomic Nervous SystemDocument3 pagesThe Autonomic Nervous SystemBarneybabybopbjbtwo FdrgyNo ratings yet
- 3 QTR Notes - Biology: Functions of The Nervous System Nervous System Histology Neurons Nerve CellsDocument4 pages3 QTR Notes - Biology: Functions of The Nervous System Nervous System Histology Neurons Nerve CellsHazel Kristy CatagueNo ratings yet
- Autonomic Nervous SystemDocument48 pagesAutonomic Nervous Systembasgsr100% (1)
- By DR. Khairun Nisa Berawi Medical Faculty Universitas LampungDocument50 pagesBy DR. Khairun Nisa Berawi Medical Faculty Universitas LampungMAHARANINo ratings yet
- The Autonomic System 2019Document50 pagesThe Autonomic System 2019TheBoss 20No ratings yet
- (PHYSIO) 1.05 Autonomic Nervous System (EGBartolome)Document7 pages(PHYSIO) 1.05 Autonomic Nervous System (EGBartolome)Izza Mari DeLeon Laurio100% (2)
- Sympathetic Parasympathetic: BrainstemDocument2 pagesSympathetic Parasympathetic: Brainstemmark riveraNo ratings yet
- Unit 2 - Nervous SystemDocument39 pagesUnit 2 - Nervous SystemzulieyanaNo ratings yet
- NERVOUS AND ENDOCRINE SYSTEM Notes and ActivityDocument9 pagesNERVOUS AND ENDOCRINE SYSTEM Notes and ActivitySamantha SaavedraNo ratings yet
- Anatomy of Trigeminal Nerve2Document41 pagesAnatomy of Trigeminal Nerve2Dr. Fatema HajiNo ratings yet
- Riverside College, Inc. Department of Physical Therapy Physiology01 Module 4 Lesson 3 Autonomic Nervous SystemDocument8 pagesRiverside College, Inc. Department of Physical Therapy Physiology01 Module 4 Lesson 3 Autonomic Nervous SystemNeonil Dequina CaceresNo ratings yet
- PY40 - BIO - GROUP3The Somatic Nervous SystemDocument22 pagesPY40 - BIO - GROUP3The Somatic Nervous SystemAdéọlá OnasanyaNo ratings yet
- Autonomic Nervous System: Lecturer - I. Savinkova, PHD Department of PhysiologyDocument55 pagesAutonomic Nervous System: Lecturer - I. Savinkova, PHD Department of PhysiologyИринаNo ratings yet
- The Central Nervous System: Andi AnsharullahDocument60 pagesThe Central Nervous System: Andi AnsharullahAnonymous vUl83IptiSNo ratings yet
- Somatosensory System and PainDocument40 pagesSomatosensory System and PainAhaisibwe GordonNo ratings yet
- Ans PowerpointDocument66 pagesAns PowerpointSirawit NiceNo ratings yet
- A. MODUL PDP 9Document40 pagesA. MODUL PDP 9Suraya Eiman ZafiraNo ratings yet
- Neural Control and CoordinationDocument16 pagesNeural Control and Coordinationadityaaggarwal821No ratings yet
- Proprioceptive Sensory SystemsDocument9 pagesProprioceptive Sensory SystemsRex HuangNo ratings yet
- BioPsychology Chapter 34Document10 pagesBioPsychology Chapter 34Johnreih BanggaNo ratings yet
- Science Reviewer 3rd Quarter For Grade 10 BiologyDocument20 pagesScience Reviewer 3rd Quarter For Grade 10 BiologyTirao, Lizette Luz O.No ratings yet
- To Autonomic Pharmacology: Anatomy of The Autonomic Nervous System: Sympathetic and Parasympathetic DivisionsDocument154 pagesTo Autonomic Pharmacology: Anatomy of The Autonomic Nervous System: Sympathetic and Parasympathetic DivisionsLycan AsaleNo ratings yet
- 300-16 The Autonomic Nervous System 2020Document24 pages300-16 The Autonomic Nervous System 202076nr4m8ndxNo ratings yet
- Nutshell NeuroDocument15 pagesNutshell NeuroAdeel abbas rajaNo ratings yet
- Pharma 2Document12 pagesPharma 2MARIEMIL FOLLOSONo ratings yet
- Histology of The Peripheral Nervous SystemDocument37 pagesHistology of The Peripheral Nervous SystemREMAN ALINGASANo ratings yet
- The Nervous SystemDocument80 pagesThe Nervous SystemAngelicaBarbosaNo ratings yet
- O Inferior Hypogastric Plexus/pelvis PlexusDocument11 pagesO Inferior Hypogastric Plexus/pelvis PlexusMaxinefgc BaculoNo ratings yet
- Physio Reviwer (AutoRecovered)Document16 pagesPhysio Reviwer (AutoRecovered)Maria Angelica PescadorNo ratings yet
- Autonomic Nervous System For MBBSDocument20 pagesAutonomic Nervous System For MBBSjacobsNo ratings yet
- Nervous System ExaminationDocument84 pagesNervous System ExaminationFelix FwsNo ratings yet
- Introduction of Neuroanatomy: Muhammad Iqbal BasriDocument14 pagesIntroduction of Neuroanatomy: Muhammad Iqbal BasriUgaNo ratings yet
- Mind at Rest: How Neuron Structure Evolves in the Sleep Cycle.From EverandMind at Rest: How Neuron Structure Evolves in the Sleep Cycle.No ratings yet
- 5851 978-1-5386-4658-8/18/$31.00 ©2019 Ieee Icassp 2019Document5 pages5851 978-1-5386-4658-8/18/$31.00 ©2019 Ieee Icassp 2019Swarnadip SahaNo ratings yet
- KriptorkismusDocument14 pagesKriptorkismusMutiara Prima DianaNo ratings yet
- Document 5Document5 pagesDocument 5kauthar hassanNo ratings yet
- The Heart Activity 3 PDFDocument4 pagesThe Heart Activity 3 PDFbiancaNo ratings yet
- JRF Question Bank-1 PDFDocument479 pagesJRF Question Bank-1 PDFBilal HassanNo ratings yet
- 10 Simple Home Remedies For Flawless Smooth Glowing SkinDocument2 pages10 Simple Home Remedies For Flawless Smooth Glowing SkinFirdous BhatNo ratings yet
- Alambra Et Al - Review & Comments Edited 01-22 EditDocument8 pagesAlambra Et Al - Review & Comments Edited 01-22 EditKenneth_Alambr_1485No ratings yet
- Contrast Media: Vashist B. Mhalsekar III Year Medical Imaging Technology Goa Medical CollegeDocument33 pagesContrast Media: Vashist B. Mhalsekar III Year Medical Imaging Technology Goa Medical CollegeOmkar GaonkarNo ratings yet
- Human NutritionDocument11 pagesHuman NutritionAbby Faure100% (2)
- Parts of The BodyDocument7 pagesParts of The BodyAnita de BorbonNo ratings yet
- Pengaruh Berbagai Jenis Skarifikasi Terhadap Perkecambahan Benih Saga (Adenanthera Pavonina L) Di Persemaian Permanen Bpdas Palu-PosoDocument6 pagesPengaruh Berbagai Jenis Skarifikasi Terhadap Perkecambahan Benih Saga (Adenanthera Pavonina L) Di Persemaian Permanen Bpdas Palu-PosoKhxlifx CarakaNo ratings yet
- PAM Abd BLOSUMDocument3 pagesPAM Abd BLOSUMhohoiyinNo ratings yet
- ITP ReviewerDocument8 pagesITP ReviewerBailey EtormaNo ratings yet
- Exam ANS Pharmacology Report Inter2023 1 PRVDocument8 pagesExam ANS Pharmacology Report Inter2023 1 PRVtestingNo ratings yet
- Sorenson Atlas of Human Histology Chapter 14Document42 pagesSorenson Atlas of Human Histology Chapter 14NUEVO SUSANNA N.No ratings yet
- Neuroimaging Clinics - Imaging of Head TraumaDocument184 pagesNeuroimaging Clinics - Imaging of Head TraumaSimion Iulian100% (1)
- PharmacologyDocument84 pagesPharmacologyhenrydycoco100% (1)
- Anatomi Kepala Dan Leher: Oleh: Abdullah Putra Perdana Ppds Ilmu Bedah FK Ulm 2017Document32 pagesAnatomi Kepala Dan Leher: Oleh: Abdullah Putra Perdana Ppds Ilmu Bedah FK Ulm 2017drhendyjuniorNo ratings yet
- InstrumentsDocument35 pagesInstrumentsvgmanjunathNo ratings yet
- Plant Biology - IB Biology SL Grade 11Document6 pagesPlant Biology - IB Biology SL Grade 11atharNo ratings yet
- Guyton Physiology Trang 784 796Document13 pagesGuyton Physiology Trang 784 796Bùi Nguyễn Yến VyNo ratings yet
- Schools Division of Negros Oriental: Republic of The Philippines Region VII, Central VisayasDocument2 pagesSchools Division of Negros Oriental: Republic of The Philippines Region VII, Central VisayasSharna Flynn SolonNo ratings yet
- Oral Anatomy DefinitionDocument17 pagesOral Anatomy DefinitionJoe AjibadeNo ratings yet
- Abdominal Aortic AneurysmDocument3 pagesAbdominal Aortic AneurysmyabaeveNo ratings yet
- Digestive System NotesDocument11 pagesDigestive System NotesijustneedtheanswersNo ratings yet
























































































Download as pdf or txt
You might also like
- NASM CPT Study Guide - 7th EditionDocument22 pagesNASM CPT Study Guide - 7th Editionlatifa100% (3)
- Dr. Azam Anatomy NLC Notes For Dec 2021 ExamDocument134 pagesDr. Azam Anatomy NLC Notes For Dec 2021 ExamCastleKG100% (4)
- Fish Sauce ProductionDocument44 pagesFish Sauce ProductionTHANH PHẠM KIM NGUYỆT100% (1)
- Onion Root Tip MitosisDocument5 pagesOnion Root Tip MitosisNor Ashikin IsmailNo ratings yet
- Mock Tests 20 20 Class 4 Science SampleDocument13 pagesMock Tests 20 20 Class 4 Science SampleRueban manohar75% (4)
- (See Next Diagram) : Autonomic Nervous System Rashelle Lopez-Salvatierra, MD Somatic DivisionDocument7 pages(See Next Diagram) : Autonomic Nervous System Rashelle Lopez-Salvatierra, MD Somatic Divisionemely p. tango100% (4)
- Pharma - Neurotransmission Ans and SnsDocument10 pagesPharma - Neurotransmission Ans and SnsksescletoNo ratings yet
- Biology NotesDocument102 pagesBiology Notesajabgul123493No ratings yet
- Professor of Anatomy Dept. of Biomedical Sciences Heritage College of Osteopathic Medicine, Ohio University Athens, Ohio 45701 Witmerl@Ohio - EduDocument20 pagesProfessor of Anatomy Dept. of Biomedical Sciences Heritage College of Osteopathic Medicine, Ohio University Athens, Ohio 45701 Witmerl@Ohio - EduAri SudarsonoNo ratings yet
- Autonomic Nervous SystemDocument68 pagesAutonomic Nervous SystemTahir AzizNo ratings yet
- Autonomic and Systemic Pharmacology DR DahalDocument119 pagesAutonomic and Systemic Pharmacology DR Dahalअविनाश भाल्टरNo ratings yet
- The SNS and ANS Share Afferent Neurons: Autonomic Nervous SystemDocument5 pagesThe SNS and ANS Share Afferent Neurons: Autonomic Nervous SystemIshani ManivannanNo ratings yet
- 8 - Autonomic Nervous SystemDocument23 pages8 - Autonomic Nervous SystemibhaslauraNo ratings yet
- Anatomy ANSDocument8 pagesAnatomy ANSashim tiwariNo ratings yet
- Autonomic NSDocument9 pagesAutonomic NSsanyamana935No ratings yet
- Autonomic Nervous SystemDocument20 pagesAutonomic Nervous SystemArian May MarcosNo ratings yet
- Unit 2 - Nervous SystemDocument49 pagesUnit 2 - Nervous SystemAbdullah MohammedNo ratings yet
- 1st SemDocument158 pages1st SemSana chaudharyNo ratings yet
- 2023.neuroscience - Trans14.autonomic Nervous SystemDocument13 pages2023.neuroscience - Trans14.autonomic Nervous SystemstellaNo ratings yet
- Slide Deck 4 - ANSDocument21 pagesSlide Deck 4 - ANSCharlotte KalilecNo ratings yet
- Neuroanatomy: Autonomic Nervous System Dr. Antonio T. Parong JRDocument10 pagesNeuroanatomy: Autonomic Nervous System Dr. Antonio T. Parong JRZllison Mae Teodoro MangabatNo ratings yet
- Module 5 - 14. Ans NotesDocument6 pagesModule 5 - 14. Ans Notesjieannfaith.ausmolo-20No ratings yet
- St. Luke's College of Medicine - William H. Quasha Memorial: PhysiologyDocument6 pagesSt. Luke's College of Medicine - William H. Quasha Memorial: PhysiologyMavic Villanueva100% (1)
- Autonomic Nervous SystemDocument49 pagesAutonomic Nervous SystemAzmi PlusNo ratings yet
- Autonomic Nervous SystemDocument41 pagesAutonomic Nervous SystemYanto HaryantoNo ratings yet
- Basic Bladder NeurophysiologyDocument8 pagesBasic Bladder Neurophysiologylinda margaritaNo ratings yet
- Autonomic Nervous SystemDocument50 pagesAutonomic Nervous SystemEbti Rizki UtamiNo ratings yet
- CHAPTER 8, Neurotransmission - The Autonomic and Somatic Motor Nervous SystemDocument15 pagesCHAPTER 8, Neurotransmission - The Autonomic and Somatic Motor Nervous SystemoreaNo ratings yet
- Control and Coordination PDFDocument24 pagesControl and Coordination PDFMUZEER PASHANo ratings yet
- ICSE Biology Notes Nervous System For 20 PDFDocument25 pagesICSE Biology Notes Nervous System For 20 PDFMmt RdcNo ratings yet
- Study Guide 5Document39 pagesStudy Guide 5Amina Rose AlghamdiNo ratings yet
- Central - Peripheral Nervous SystemDocument82 pagesCentral - Peripheral Nervous System52-nur Fadiyyah FNo ratings yet
- The Autonomic Nervous SystemDocument3 pagesThe Autonomic Nervous SystemBarneybabybopbjbtwo FdrgyNo ratings yet
- 3 QTR Notes - Biology: Functions of The Nervous System Nervous System Histology Neurons Nerve CellsDocument4 pages3 QTR Notes - Biology: Functions of The Nervous System Nervous System Histology Neurons Nerve CellsHazel Kristy CatagueNo ratings yet
- Autonomic Nervous SystemDocument48 pagesAutonomic Nervous Systembasgsr100% (1)
- By DR. Khairun Nisa Berawi Medical Faculty Universitas LampungDocument50 pagesBy DR. Khairun Nisa Berawi Medical Faculty Universitas LampungMAHARANINo ratings yet
- The Autonomic System 2019Document50 pagesThe Autonomic System 2019TheBoss 20No ratings yet
- (PHYSIO) 1.05 Autonomic Nervous System (EGBartolome)Document7 pages(PHYSIO) 1.05 Autonomic Nervous System (EGBartolome)Izza Mari DeLeon Laurio100% (2)
- Sympathetic Parasympathetic: BrainstemDocument2 pagesSympathetic Parasympathetic: Brainstemmark riveraNo ratings yet
- Unit 2 - Nervous SystemDocument39 pagesUnit 2 - Nervous SystemzulieyanaNo ratings yet
- NERVOUS AND ENDOCRINE SYSTEM Notes and ActivityDocument9 pagesNERVOUS AND ENDOCRINE SYSTEM Notes and ActivitySamantha SaavedraNo ratings yet
- Anatomy of Trigeminal Nerve2Document41 pagesAnatomy of Trigeminal Nerve2Dr. Fatema HajiNo ratings yet
- Riverside College, Inc. Department of Physical Therapy Physiology01 Module 4 Lesson 3 Autonomic Nervous SystemDocument8 pagesRiverside College, Inc. Department of Physical Therapy Physiology01 Module 4 Lesson 3 Autonomic Nervous SystemNeonil Dequina CaceresNo ratings yet
- PY40 - BIO - GROUP3The Somatic Nervous SystemDocument22 pagesPY40 - BIO - GROUP3The Somatic Nervous SystemAdéọlá OnasanyaNo ratings yet
- Autonomic Nervous System: Lecturer - I. Savinkova, PHD Department of PhysiologyDocument55 pagesAutonomic Nervous System: Lecturer - I. Savinkova, PHD Department of PhysiologyИринаNo ratings yet
- The Central Nervous System: Andi AnsharullahDocument60 pagesThe Central Nervous System: Andi AnsharullahAnonymous vUl83IptiSNo ratings yet
- Somatosensory System and PainDocument40 pagesSomatosensory System and PainAhaisibwe GordonNo ratings yet
- Ans PowerpointDocument66 pagesAns PowerpointSirawit NiceNo ratings yet
- A. MODUL PDP 9Document40 pagesA. MODUL PDP 9Suraya Eiman ZafiraNo ratings yet
- Neural Control and CoordinationDocument16 pagesNeural Control and Coordinationadityaaggarwal821No ratings yet
- Proprioceptive Sensory SystemsDocument9 pagesProprioceptive Sensory SystemsRex HuangNo ratings yet
- BioPsychology Chapter 34Document10 pagesBioPsychology Chapter 34Johnreih BanggaNo ratings yet
- Science Reviewer 3rd Quarter For Grade 10 BiologyDocument20 pagesScience Reviewer 3rd Quarter For Grade 10 BiologyTirao, Lizette Luz O.No ratings yet
- To Autonomic Pharmacology: Anatomy of The Autonomic Nervous System: Sympathetic and Parasympathetic DivisionsDocument154 pagesTo Autonomic Pharmacology: Anatomy of The Autonomic Nervous System: Sympathetic and Parasympathetic DivisionsLycan AsaleNo ratings yet
- 300-16 The Autonomic Nervous System 2020Document24 pages300-16 The Autonomic Nervous System 202076nr4m8ndxNo ratings yet
- Nutshell NeuroDocument15 pagesNutshell NeuroAdeel abbas rajaNo ratings yet
- Pharma 2Document12 pagesPharma 2MARIEMIL FOLLOSONo ratings yet
- Histology of The Peripheral Nervous SystemDocument37 pagesHistology of The Peripheral Nervous SystemREMAN ALINGASANo ratings yet
- The Nervous SystemDocument80 pagesThe Nervous SystemAngelicaBarbosaNo ratings yet
- O Inferior Hypogastric Plexus/pelvis PlexusDocument11 pagesO Inferior Hypogastric Plexus/pelvis PlexusMaxinefgc BaculoNo ratings yet
- Physio Reviwer (AutoRecovered)Document16 pagesPhysio Reviwer (AutoRecovered)Maria Angelica PescadorNo ratings yet
- Autonomic Nervous System For MBBSDocument20 pagesAutonomic Nervous System For MBBSjacobsNo ratings yet
- Nervous System ExaminationDocument84 pagesNervous System ExaminationFelix FwsNo ratings yet
- Introduction of Neuroanatomy: Muhammad Iqbal BasriDocument14 pagesIntroduction of Neuroanatomy: Muhammad Iqbal BasriUgaNo ratings yet
- Mind at Rest: How Neuron Structure Evolves in the Sleep Cycle.From EverandMind at Rest: How Neuron Structure Evolves in the Sleep Cycle.No ratings yet
- 5851 978-1-5386-4658-8/18/$31.00 ©2019 Ieee Icassp 2019Document5 pages5851 978-1-5386-4658-8/18/$31.00 ©2019 Ieee Icassp 2019Swarnadip SahaNo ratings yet
- KriptorkismusDocument14 pagesKriptorkismusMutiara Prima DianaNo ratings yet
- Document 5Document5 pagesDocument 5kauthar hassanNo ratings yet
- The Heart Activity 3 PDFDocument4 pagesThe Heart Activity 3 PDFbiancaNo ratings yet
- JRF Question Bank-1 PDFDocument479 pagesJRF Question Bank-1 PDFBilal HassanNo ratings yet
- 10 Simple Home Remedies For Flawless Smooth Glowing SkinDocument2 pages10 Simple Home Remedies For Flawless Smooth Glowing SkinFirdous BhatNo ratings yet
- Alambra Et Al - Review & Comments Edited 01-22 EditDocument8 pagesAlambra Et Al - Review & Comments Edited 01-22 EditKenneth_Alambr_1485No ratings yet
- Contrast Media: Vashist B. Mhalsekar III Year Medical Imaging Technology Goa Medical CollegeDocument33 pagesContrast Media: Vashist B. Mhalsekar III Year Medical Imaging Technology Goa Medical CollegeOmkar GaonkarNo ratings yet
- Human NutritionDocument11 pagesHuman NutritionAbby Faure100% (2)
- Parts of The BodyDocument7 pagesParts of The BodyAnita de BorbonNo ratings yet
- Pengaruh Berbagai Jenis Skarifikasi Terhadap Perkecambahan Benih Saga (Adenanthera Pavonina L) Di Persemaian Permanen Bpdas Palu-PosoDocument6 pagesPengaruh Berbagai Jenis Skarifikasi Terhadap Perkecambahan Benih Saga (Adenanthera Pavonina L) Di Persemaian Permanen Bpdas Palu-PosoKhxlifx CarakaNo ratings yet
- PAM Abd BLOSUMDocument3 pagesPAM Abd BLOSUMhohoiyinNo ratings yet
- ITP ReviewerDocument8 pagesITP ReviewerBailey EtormaNo ratings yet
- Exam ANS Pharmacology Report Inter2023 1 PRVDocument8 pagesExam ANS Pharmacology Report Inter2023 1 PRVtestingNo ratings yet
- Sorenson Atlas of Human Histology Chapter 14Document42 pagesSorenson Atlas of Human Histology Chapter 14NUEVO SUSANNA N.No ratings yet
- Neuroimaging Clinics - Imaging of Head TraumaDocument184 pagesNeuroimaging Clinics - Imaging of Head TraumaSimion Iulian100% (1)
- PharmacologyDocument84 pagesPharmacologyhenrydycoco100% (1)
- Anatomi Kepala Dan Leher: Oleh: Abdullah Putra Perdana Ppds Ilmu Bedah FK Ulm 2017Document32 pagesAnatomi Kepala Dan Leher: Oleh: Abdullah Putra Perdana Ppds Ilmu Bedah FK Ulm 2017drhendyjuniorNo ratings yet
- InstrumentsDocument35 pagesInstrumentsvgmanjunathNo ratings yet
- Plant Biology - IB Biology SL Grade 11Document6 pagesPlant Biology - IB Biology SL Grade 11atharNo ratings yet
- Guyton Physiology Trang 784 796Document13 pagesGuyton Physiology Trang 784 796Bùi Nguyễn Yến VyNo ratings yet
- Schools Division of Negros Oriental: Republic of The Philippines Region VII, Central VisayasDocument2 pagesSchools Division of Negros Oriental: Republic of The Philippines Region VII, Central VisayasSharna Flynn SolonNo ratings yet
- Oral Anatomy DefinitionDocument17 pagesOral Anatomy DefinitionJoe AjibadeNo ratings yet
- Abdominal Aortic AneurysmDocument3 pagesAbdominal Aortic AneurysmyabaeveNo ratings yet
- Digestive System NotesDocument11 pagesDigestive System NotesijustneedtheanswersNo ratings yet