
Gastric Disease
Gastric Disease
You might also like
- Ceces Study Guides 1&2Document56 pagesCeces Study Guides 1&2Kimberly Louise LopezNo ratings yet
- 2021 Return To Play Protocols - USL ChampionshipDocument62 pages2021 Return To Play Protocols - USL ChampionshipUSLNo ratings yet
- PancreatitisDocument6 pagesPancreatitisMary AmaliaNo ratings yet
- Encefalopatie Notițe EngDocument4 pagesEncefalopatie Notițe EngAnda884No ratings yet
- АDocument78 pagesАjaha190702No ratings yet
- Gastro Esophageal Reflux Disease (GERD)Document7 pagesGastro Esophageal Reflux Disease (GERD)MahaNo ratings yet
- Osmosis Esophageal Disease PDF Amm DR NotesDocument13 pagesOsmosis Esophageal Disease PDF Amm DR NotestajammalNo ratings yet
- hs320 W11 DigestiveSystemDisordersDocument41 pageshs320 W11 DigestiveSystemDisordersjoseyalm2323No ratings yet
- Nausea 0 VomitingDocument10 pagesNausea 0 VomitingJasmeen KaurNo ratings yet
- Balance DisordersDocument6 pagesBalance DisordersAli 10No ratings yet
- Dyspepsia Abdul Rahman NewDocument50 pagesDyspepsia Abdul Rahman NewRahmawati Nur AriyantiNo ratings yet
- Kelainan-Kelainan Ginjal Yang Sering Pada AnakDocument76 pagesKelainan-Kelainan Ginjal Yang Sering Pada Anakindragirsang21No ratings yet
- Im Irritable Bowel Syndrome Intestinal Obstruction Acute Appendicitis Lecture TransDocument6 pagesIm Irritable Bowel Syndrome Intestinal Obstruction Acute Appendicitis Lecture TransMelissa LabadorNo ratings yet
- Nitourinary Tract InfectionsDocument4 pagesNitourinary Tract InfectionsWoo Rin ParkNo ratings yet
- Renal and Urinary DisordersDocument11 pagesRenal and Urinary DisordersChristian Espanilla100% (4)
- Dyspepsia LectureDocument2 pagesDyspepsia LectureDaneva Reyes0% (1)
- Drugstudy BangkalDocument16 pagesDrugstudy BangkalClaire MachicaNo ratings yet
- Oral and Esophageal DisordersDocument33 pagesOral and Esophageal DisordersSandeepNo ratings yet
- Adrenal HyperfunctionDocument5 pagesAdrenal HyperfunctionHalla BennaaNo ratings yet
- H.A.M. Akil Fardah Akil: "GI Disorders" Lecture in GERIATRI System, FKUHDocument14 pagesH.A.M. Akil Fardah Akil: "GI Disorders" Lecture in GERIATRI System, FKUHCutDianafitriaNo ratings yet
- 02 ConstipationDocument11 pages02 ConstipationYunus AmmarieNo ratings yet
- Dysphagia, Dyspepsia, VomitingDocument24 pagesDysphagia, Dyspepsia, VomitingNasser SalahNo ratings yet
- IM Lecture (GIT) ?Document105 pagesIM Lecture (GIT) ?om635arNo ratings yet
- MS Lec Gi and Icp Reviewer - Limon, Adine Jeminah DDocument8 pagesMS Lec Gi and Icp Reviewer - Limon, Adine Jeminah DShawn TejanoNo ratings yet
- NRG 304 Lec 9Document3 pagesNRG 304 Lec 9Patricia Therese BernadezNo ratings yet
- INA 2 Medical Surgical Nursing Gastrointestinal SystemDocument36 pagesINA 2 Medical Surgical Nursing Gastrointestinal SystemMeryville JacildoNo ratings yet
- Nausea Vomiting ReportDocument67 pagesNausea Vomiting Reportstephanie gayetaNo ratings yet
- Anorexia: Basic InformationDocument34 pagesAnorexia: Basic InformationcarlosNo ratings yet
- Upper Gastrointestinal Congenital MalformationsDocument8 pagesUpper Gastrointestinal Congenital Malformationsaasingh7800No ratings yet
- Gastroesophageal Reflux Disease (GERD) : Glayza P. TiuDocument22 pagesGastroesophageal Reflux Disease (GERD) : Glayza P. TiuTiffany TiuNo ratings yet
- Muntah Pada Anak PDFDocument21 pagesMuntah Pada Anak PDFAndika SiswantaNo ratings yet
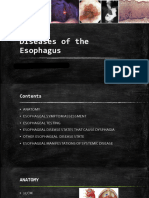
- Diseases of EsophagusDocument133 pagesDiseases of EsophagusSawanyaPrammanakulNo ratings yet
- Elderly, Disability CareDocument32 pagesElderly, Disability CareVita YoanitaNo ratings yet
- 1-Differential Diagnosis of Vomiting 2021 PsáderR SAM3Document28 pages1-Differential Diagnosis of Vomiting 2021 PsáderR SAM3Simay KızılkayaNo ratings yet
- 02 VomitingDocument36 pages02 VomitingHasan BaiquniNo ratings yet
- Acute Pancreatitis: Aguirre, Lucas Galligani, Guido Gorostiaga, Marcos Kreutzer, GustavoDocument20 pagesAcute Pancreatitis: Aguirre, Lucas Galligani, Guido Gorostiaga, Marcos Kreutzer, GustavoGüids GalliganiNo ratings yet
- 06.2 Inborn Error of Metabolism - Iii B - Trans PDFDocument10 pages06.2 Inborn Error of Metabolism - Iii B - Trans PDFAshim AbhiNo ratings yet
- Upper GI Guided NotesDocument9 pagesUpper GI Guided NotesVanessaNo ratings yet
- Intestinal ObstructionDocument46 pagesIntestinal ObstructionvenkatNo ratings yet
- Lianne Beck, MD Assistant Professor Emory Family MedicineDocument52 pagesLianne Beck, MD Assistant Professor Emory Family MedicineTauqeer IqbalNo ratings yet
- Nursing Care of Clients With Altered Metabolic GastrointestinalDocument75 pagesNursing Care of Clients With Altered Metabolic GastrointestinalGrace Jane DionaldoNo ratings yet
- Dysphagia: Ian Paul Titus DM FRCSDocument59 pagesDysphagia: Ian Paul Titus DM FRCSGiovanni HenryNo ratings yet
- 62 DiarrheaChronic MGHG MIMG MFM 20161229Document10 pages62 DiarrheaChronic MGHG MIMG MFM 20161229Wei HangNo ratings yet
- Anti EpilepticsDocument9 pagesAnti Epilepticsnur qistina humaira zulkarshamsiNo ratings yet
- GitDocument302 pagesGitjgcriste100% (7)
- Lecture 1part 2Document50 pagesLecture 1part 2mashe1No ratings yet
- PD 3.2 Alterations in GI Function Part 1Document6 pagesPD 3.2 Alterations in GI Function Part 1Kim DeeNo ratings yet
- Presenting Problems in Gastrointestinal Disease:: DysphagiaDocument9 pagesPresenting Problems in Gastrointestinal Disease:: DysphagiaMohamed AlsaabNo ratings yet
- Acute Pancreatitis: Aguirre, Lucas Galligani, Guido Gorostiaga, Marcos Kreutzer, GustavoDocument20 pagesAcute Pancreatitis: Aguirre, Lucas Galligani, Guido Gorostiaga, Marcos Kreutzer, GustavoGüids GalliganiNo ratings yet
- Chapter 5, CARE OF OLDERDocument7 pagesChapter 5, CARE OF OLDERGracian Vel AsocsomNo ratings yet
- Pain and Mobility Medication CardsDocument8 pagesPain and Mobility Medication CardsJamie O.No ratings yet
- Assignment Cancer Prevention LectureDocument12 pagesAssignment Cancer Prevention LectureAlexNo ratings yet
- Pancreatitis - Rhuby AbenojaDocument17 pagesPancreatitis - Rhuby AbenojaRhuby Pascual AbenojaNo ratings yet
- Evaluation of Patients With PolyuriaDocument25 pagesEvaluation of Patients With Polyurianaura ghinaNo ratings yet
- Inflammatory Bowel DiseaseDocument8 pagesInflammatory Bowel Diseasevmc6gyvh9gNo ratings yet
- Imprinting DisordersDocument4 pagesImprinting Disordersanwar jabariNo ratings yet
- Liver DiseasesDocument27 pagesLiver DiseasesharideepNo ratings yet
- Gastrointestinal TransesDocument22 pagesGastrointestinal TransesKrystal MericulloNo ratings yet
- Kuliah 2Document97 pagesKuliah 2Septia AnggaswariNo ratings yet
- BioDocument18 pagesBioKinza ZubairNo ratings yet
- Case Presentation: Cagayan Valley Medical CenterDocument57 pagesCase Presentation: Cagayan Valley Medical CenterGian Pagaddu100% (1)
- The Perfect Insulin Resistance Diet Cookbook:The Complete Nutrition Guide To Losing Weight, Reversing Insulin Resistant And And Preventing Pre-Diabetes With Delectable And Nourishing RecipesFrom EverandThe Perfect Insulin Resistance Diet Cookbook:The Complete Nutrition Guide To Losing Weight, Reversing Insulin Resistant And And Preventing Pre-Diabetes With Delectable And Nourishing RecipesNo ratings yet
- Amniotic Pulmonary Embolism Medical Malpractice Case StudyDocument4 pagesAmniotic Pulmonary Embolism Medical Malpractice Case StudyMiguel CastricionesNo ratings yet
- Insulin Sliding Scale Protocol For Type II Diabetic PatientsDocument3 pagesInsulin Sliding Scale Protocol For Type II Diabetic PatientsDaulat JosuaNo ratings yet
- Psychiatric Nursing - Psycho PharmacologyDocument50 pagesPsychiatric Nursing - Psycho PharmacologyKaren MichelleNo ratings yet
- Conserving Blood During Cardiac Surgery at Huntington University Hospital (A)Document6 pagesConserving Blood During Cardiac Surgery at Huntington University Hospital (A)Touba KhalidNo ratings yet
- Treatment ModalitiesDocument5 pagesTreatment ModalitiesMichelleIragAlmarioNo ratings yet
- Pharmacy Guidelines 2Document2 pagesPharmacy Guidelines 2Inas IbrahimNo ratings yet
- Of Antimicrobial Resistance: The Who Aware (Access, Watch, Reserve) Antibiotic Book and PreventionDocument7 pagesOf Antimicrobial Resistance: The Who Aware (Access, Watch, Reserve) Antibiotic Book and PreventionBBD BBDNo ratings yet
- Nasty Creatures.: 1. According To The Author Ticks Can Transmit To Humans Such Illnesses AsDocument4 pagesNasty Creatures.: 1. According To The Author Ticks Can Transmit To Humans Such Illnesses AsКсенияNo ratings yet
- Mac OS X 10.3.7 Quartz PDFContext - Word - 000494Document3 pagesMac OS X 10.3.7 Quartz PDFContext - Word - 000494srini durveshNo ratings yet
- Life Is Good in JC 2015Document64 pagesLife Is Good in JC 2015News_TribuneNo ratings yet
- Routine Newborn Pediatrics: Goals of Neonate CareDocument29 pagesRoutine Newborn Pediatrics: Goals of Neonate CareAshlin HinojosaNo ratings yet
- Draft: The Principles of Infection Prevention and ControlDocument36 pagesDraft: The Principles of Infection Prevention and Controlandrel davidNo ratings yet
- Set 3 PNLE IDocument52 pagesSet 3 PNLE IDarnell Adrian EstobioNo ratings yet
- PRIO Lemus Acute Pain and Risk For Def. Fluid VolumeDocument3 pagesPRIO Lemus Acute Pain and Risk For Def. Fluid VolumeChe ValenzuelaNo ratings yet
- Radial Vascular Complication - Rini Tri MarwantiDocument29 pagesRadial Vascular Complication - Rini Tri MarwantiLail نعمانNo ratings yet
- Aravind Eye Hospital, Madurai, IndiaDocument8 pagesAravind Eye Hospital, Madurai, IndiaArka Mitra100% (2)
- YL Camping Consent and Health FormDocument4 pagesYL Camping Consent and Health Formmcronin1970No ratings yet
- Daftar PustakaDocument5 pagesDaftar Pustakaandika scribd1No ratings yet
- Coming Soon Full-Body Transplants But Is Your Soul IncludedDocument3 pagesComing Soon Full-Body Transplants But Is Your Soul IncludedscribedoctorNo ratings yet
- Criticool-Management of Temperature During and After Cardiac Surgery PDFDocument4 pagesCriticool-Management of Temperature During and After Cardiac Surgery PDFMrunali PatilNo ratings yet
- Tang Et Al. - 2020 - Abnormal Coagulation Parameters Are Associated With Poor Prognosis in Patients With Novel Coronavirus PneumoniaDocument4 pagesTang Et Al. - 2020 - Abnormal Coagulation Parameters Are Associated With Poor Prognosis in Patients With Novel Coronavirus PneumoniaAlexandre Campos Moraes AmatoNo ratings yet
- An Insight Into The Quality Assurance of Ayurvedic, Siddha and Unani DrugsDocument10 pagesAn Insight Into The Quality Assurance of Ayurvedic, Siddha and Unani DrugsHomoeopathic PulseNo ratings yet
- Drug Study AMIODARONE & PROPOFOLDocument3 pagesDrug Study AMIODARONE & PROPOFOLNIKKI CARYL ZAFRANo ratings yet
- BronchiolitisDocument45 pagesBronchiolitisYuusuf MubarikNo ratings yet
- Oral Assessment 1 Infants and Children in Ward AreasDocument2 pagesOral Assessment 1 Infants and Children in Ward AreasRiniRiandiniNo ratings yet
- Occupational English Test: Writing Sub-Test: Nursing Time Allowed: Reading Time: 5 Minutes Writing Time: 40 MinutesDocument2 pagesOccupational English Test: Writing Sub-Test: Nursing Time Allowed: Reading Time: 5 Minutes Writing Time: 40 MinutesAnit XingNo ratings yet
- The Physical Therapy Licensure Examination Syllabus (Philippines) )Document14 pagesThe Physical Therapy Licensure Examination Syllabus (Philippines) )Xy FloresNo ratings yet
- Principles of Basic Clinical Pharmacokinetic ParametersDocument7 pagesPrinciples of Basic Clinical Pharmacokinetic ParametersThe Ghost By HarethNo ratings yet
























































































Download as pdf or txt
You might also like
- Ceces Study Guides 1&2Document56 pagesCeces Study Guides 1&2Kimberly Louise LopezNo ratings yet
- 2021 Return To Play Protocols - USL ChampionshipDocument62 pages2021 Return To Play Protocols - USL ChampionshipUSLNo ratings yet
- PancreatitisDocument6 pagesPancreatitisMary AmaliaNo ratings yet
- Encefalopatie Notițe EngDocument4 pagesEncefalopatie Notițe EngAnda884No ratings yet
- АDocument78 pagesАjaha190702No ratings yet
- Gastro Esophageal Reflux Disease (GERD)Document7 pagesGastro Esophageal Reflux Disease (GERD)MahaNo ratings yet
- Osmosis Esophageal Disease PDF Amm DR NotesDocument13 pagesOsmosis Esophageal Disease PDF Amm DR NotestajammalNo ratings yet
- hs320 W11 DigestiveSystemDisordersDocument41 pageshs320 W11 DigestiveSystemDisordersjoseyalm2323No ratings yet
- Nausea 0 VomitingDocument10 pagesNausea 0 VomitingJasmeen KaurNo ratings yet
- Balance DisordersDocument6 pagesBalance DisordersAli 10No ratings yet
- Dyspepsia Abdul Rahman NewDocument50 pagesDyspepsia Abdul Rahman NewRahmawati Nur AriyantiNo ratings yet
- Kelainan-Kelainan Ginjal Yang Sering Pada AnakDocument76 pagesKelainan-Kelainan Ginjal Yang Sering Pada Anakindragirsang21No ratings yet
- Im Irritable Bowel Syndrome Intestinal Obstruction Acute Appendicitis Lecture TransDocument6 pagesIm Irritable Bowel Syndrome Intestinal Obstruction Acute Appendicitis Lecture TransMelissa LabadorNo ratings yet
- Nitourinary Tract InfectionsDocument4 pagesNitourinary Tract InfectionsWoo Rin ParkNo ratings yet
- Renal and Urinary DisordersDocument11 pagesRenal and Urinary DisordersChristian Espanilla100% (4)
- Dyspepsia LectureDocument2 pagesDyspepsia LectureDaneva Reyes0% (1)
- Drugstudy BangkalDocument16 pagesDrugstudy BangkalClaire MachicaNo ratings yet
- Oral and Esophageal DisordersDocument33 pagesOral and Esophageal DisordersSandeepNo ratings yet
- Adrenal HyperfunctionDocument5 pagesAdrenal HyperfunctionHalla BennaaNo ratings yet
- H.A.M. Akil Fardah Akil: "GI Disorders" Lecture in GERIATRI System, FKUHDocument14 pagesH.A.M. Akil Fardah Akil: "GI Disorders" Lecture in GERIATRI System, FKUHCutDianafitriaNo ratings yet
- 02 ConstipationDocument11 pages02 ConstipationYunus AmmarieNo ratings yet
- Dysphagia, Dyspepsia, VomitingDocument24 pagesDysphagia, Dyspepsia, VomitingNasser SalahNo ratings yet
- IM Lecture (GIT) ?Document105 pagesIM Lecture (GIT) ?om635arNo ratings yet
- MS Lec Gi and Icp Reviewer - Limon, Adine Jeminah DDocument8 pagesMS Lec Gi and Icp Reviewer - Limon, Adine Jeminah DShawn TejanoNo ratings yet
- NRG 304 Lec 9Document3 pagesNRG 304 Lec 9Patricia Therese BernadezNo ratings yet
- INA 2 Medical Surgical Nursing Gastrointestinal SystemDocument36 pagesINA 2 Medical Surgical Nursing Gastrointestinal SystemMeryville JacildoNo ratings yet
- Nausea Vomiting ReportDocument67 pagesNausea Vomiting Reportstephanie gayetaNo ratings yet
- Anorexia: Basic InformationDocument34 pagesAnorexia: Basic InformationcarlosNo ratings yet
- Upper Gastrointestinal Congenital MalformationsDocument8 pagesUpper Gastrointestinal Congenital Malformationsaasingh7800No ratings yet
- Gastroesophageal Reflux Disease (GERD) : Glayza P. TiuDocument22 pagesGastroesophageal Reflux Disease (GERD) : Glayza P. TiuTiffany TiuNo ratings yet
- Muntah Pada Anak PDFDocument21 pagesMuntah Pada Anak PDFAndika SiswantaNo ratings yet
- Diseases of EsophagusDocument133 pagesDiseases of EsophagusSawanyaPrammanakulNo ratings yet
- Elderly, Disability CareDocument32 pagesElderly, Disability CareVita YoanitaNo ratings yet
- 1-Differential Diagnosis of Vomiting 2021 PsáderR SAM3Document28 pages1-Differential Diagnosis of Vomiting 2021 PsáderR SAM3Simay KızılkayaNo ratings yet
- 02 VomitingDocument36 pages02 VomitingHasan BaiquniNo ratings yet
- Acute Pancreatitis: Aguirre, Lucas Galligani, Guido Gorostiaga, Marcos Kreutzer, GustavoDocument20 pagesAcute Pancreatitis: Aguirre, Lucas Galligani, Guido Gorostiaga, Marcos Kreutzer, GustavoGüids GalliganiNo ratings yet
- 06.2 Inborn Error of Metabolism - Iii B - Trans PDFDocument10 pages06.2 Inborn Error of Metabolism - Iii B - Trans PDFAshim AbhiNo ratings yet
- Upper GI Guided NotesDocument9 pagesUpper GI Guided NotesVanessaNo ratings yet
- Intestinal ObstructionDocument46 pagesIntestinal ObstructionvenkatNo ratings yet
- Lianne Beck, MD Assistant Professor Emory Family MedicineDocument52 pagesLianne Beck, MD Assistant Professor Emory Family MedicineTauqeer IqbalNo ratings yet
- Nursing Care of Clients With Altered Metabolic GastrointestinalDocument75 pagesNursing Care of Clients With Altered Metabolic GastrointestinalGrace Jane DionaldoNo ratings yet
- Dysphagia: Ian Paul Titus DM FRCSDocument59 pagesDysphagia: Ian Paul Titus DM FRCSGiovanni HenryNo ratings yet
- 62 DiarrheaChronic MGHG MIMG MFM 20161229Document10 pages62 DiarrheaChronic MGHG MIMG MFM 20161229Wei HangNo ratings yet
- Anti EpilepticsDocument9 pagesAnti Epilepticsnur qistina humaira zulkarshamsiNo ratings yet
- GitDocument302 pagesGitjgcriste100% (7)
- Lecture 1part 2Document50 pagesLecture 1part 2mashe1No ratings yet
- PD 3.2 Alterations in GI Function Part 1Document6 pagesPD 3.2 Alterations in GI Function Part 1Kim DeeNo ratings yet
- Presenting Problems in Gastrointestinal Disease:: DysphagiaDocument9 pagesPresenting Problems in Gastrointestinal Disease:: DysphagiaMohamed AlsaabNo ratings yet
- Acute Pancreatitis: Aguirre, Lucas Galligani, Guido Gorostiaga, Marcos Kreutzer, GustavoDocument20 pagesAcute Pancreatitis: Aguirre, Lucas Galligani, Guido Gorostiaga, Marcos Kreutzer, GustavoGüids GalliganiNo ratings yet
- Chapter 5, CARE OF OLDERDocument7 pagesChapter 5, CARE OF OLDERGracian Vel AsocsomNo ratings yet
- Pain and Mobility Medication CardsDocument8 pagesPain and Mobility Medication CardsJamie O.No ratings yet
- Assignment Cancer Prevention LectureDocument12 pagesAssignment Cancer Prevention LectureAlexNo ratings yet
- Pancreatitis - Rhuby AbenojaDocument17 pagesPancreatitis - Rhuby AbenojaRhuby Pascual AbenojaNo ratings yet
- Evaluation of Patients With PolyuriaDocument25 pagesEvaluation of Patients With Polyurianaura ghinaNo ratings yet
- Inflammatory Bowel DiseaseDocument8 pagesInflammatory Bowel Diseasevmc6gyvh9gNo ratings yet
- Imprinting DisordersDocument4 pagesImprinting Disordersanwar jabariNo ratings yet
- Liver DiseasesDocument27 pagesLiver DiseasesharideepNo ratings yet
- Gastrointestinal TransesDocument22 pagesGastrointestinal TransesKrystal MericulloNo ratings yet
- Kuliah 2Document97 pagesKuliah 2Septia AnggaswariNo ratings yet
- BioDocument18 pagesBioKinza ZubairNo ratings yet
- Case Presentation: Cagayan Valley Medical CenterDocument57 pagesCase Presentation: Cagayan Valley Medical CenterGian Pagaddu100% (1)
- The Perfect Insulin Resistance Diet Cookbook:The Complete Nutrition Guide To Losing Weight, Reversing Insulin Resistant And And Preventing Pre-Diabetes With Delectable And Nourishing RecipesFrom EverandThe Perfect Insulin Resistance Diet Cookbook:The Complete Nutrition Guide To Losing Weight, Reversing Insulin Resistant And And Preventing Pre-Diabetes With Delectable And Nourishing RecipesNo ratings yet
- Amniotic Pulmonary Embolism Medical Malpractice Case StudyDocument4 pagesAmniotic Pulmonary Embolism Medical Malpractice Case StudyMiguel CastricionesNo ratings yet
- Insulin Sliding Scale Protocol For Type II Diabetic PatientsDocument3 pagesInsulin Sliding Scale Protocol For Type II Diabetic PatientsDaulat JosuaNo ratings yet
- Psychiatric Nursing - Psycho PharmacologyDocument50 pagesPsychiatric Nursing - Psycho PharmacologyKaren MichelleNo ratings yet
- Conserving Blood During Cardiac Surgery at Huntington University Hospital (A)Document6 pagesConserving Blood During Cardiac Surgery at Huntington University Hospital (A)Touba KhalidNo ratings yet
- Treatment ModalitiesDocument5 pagesTreatment ModalitiesMichelleIragAlmarioNo ratings yet
- Pharmacy Guidelines 2Document2 pagesPharmacy Guidelines 2Inas IbrahimNo ratings yet
- Of Antimicrobial Resistance: The Who Aware (Access, Watch, Reserve) Antibiotic Book and PreventionDocument7 pagesOf Antimicrobial Resistance: The Who Aware (Access, Watch, Reserve) Antibiotic Book and PreventionBBD BBDNo ratings yet
- Nasty Creatures.: 1. According To The Author Ticks Can Transmit To Humans Such Illnesses AsDocument4 pagesNasty Creatures.: 1. According To The Author Ticks Can Transmit To Humans Such Illnesses AsКсенияNo ratings yet
- Mac OS X 10.3.7 Quartz PDFContext - Word - 000494Document3 pagesMac OS X 10.3.7 Quartz PDFContext - Word - 000494srini durveshNo ratings yet
- Life Is Good in JC 2015Document64 pagesLife Is Good in JC 2015News_TribuneNo ratings yet
- Routine Newborn Pediatrics: Goals of Neonate CareDocument29 pagesRoutine Newborn Pediatrics: Goals of Neonate CareAshlin HinojosaNo ratings yet
- Draft: The Principles of Infection Prevention and ControlDocument36 pagesDraft: The Principles of Infection Prevention and Controlandrel davidNo ratings yet
- Set 3 PNLE IDocument52 pagesSet 3 PNLE IDarnell Adrian EstobioNo ratings yet
- PRIO Lemus Acute Pain and Risk For Def. Fluid VolumeDocument3 pagesPRIO Lemus Acute Pain and Risk For Def. Fluid VolumeChe ValenzuelaNo ratings yet
- Radial Vascular Complication - Rini Tri MarwantiDocument29 pagesRadial Vascular Complication - Rini Tri MarwantiLail نعمانNo ratings yet
- Aravind Eye Hospital, Madurai, IndiaDocument8 pagesAravind Eye Hospital, Madurai, IndiaArka Mitra100% (2)
- YL Camping Consent and Health FormDocument4 pagesYL Camping Consent and Health Formmcronin1970No ratings yet
- Daftar PustakaDocument5 pagesDaftar Pustakaandika scribd1No ratings yet
- Coming Soon Full-Body Transplants But Is Your Soul IncludedDocument3 pagesComing Soon Full-Body Transplants But Is Your Soul IncludedscribedoctorNo ratings yet
- Criticool-Management of Temperature During and After Cardiac Surgery PDFDocument4 pagesCriticool-Management of Temperature During and After Cardiac Surgery PDFMrunali PatilNo ratings yet
- Tang Et Al. - 2020 - Abnormal Coagulation Parameters Are Associated With Poor Prognosis in Patients With Novel Coronavirus PneumoniaDocument4 pagesTang Et Al. - 2020 - Abnormal Coagulation Parameters Are Associated With Poor Prognosis in Patients With Novel Coronavirus PneumoniaAlexandre Campos Moraes AmatoNo ratings yet
- An Insight Into The Quality Assurance of Ayurvedic, Siddha and Unani DrugsDocument10 pagesAn Insight Into The Quality Assurance of Ayurvedic, Siddha and Unani DrugsHomoeopathic PulseNo ratings yet
- Drug Study AMIODARONE & PROPOFOLDocument3 pagesDrug Study AMIODARONE & PROPOFOLNIKKI CARYL ZAFRANo ratings yet
- BronchiolitisDocument45 pagesBronchiolitisYuusuf MubarikNo ratings yet
- Oral Assessment 1 Infants and Children in Ward AreasDocument2 pagesOral Assessment 1 Infants and Children in Ward AreasRiniRiandiniNo ratings yet
- Occupational English Test: Writing Sub-Test: Nursing Time Allowed: Reading Time: 5 Minutes Writing Time: 40 MinutesDocument2 pagesOccupational English Test: Writing Sub-Test: Nursing Time Allowed: Reading Time: 5 Minutes Writing Time: 40 MinutesAnit XingNo ratings yet
- The Physical Therapy Licensure Examination Syllabus (Philippines) )Document14 pagesThe Physical Therapy Licensure Examination Syllabus (Philippines) )Xy FloresNo ratings yet
- Principles of Basic Clinical Pharmacokinetic ParametersDocument7 pagesPrinciples of Basic Clinical Pharmacokinetic ParametersThe Ghost By HarethNo ratings yet