Download as pdf or txt
You might also like
- Ds 160 Us Visa ApplicationDocument8 pagesDs 160 Us Visa ApplicationCeasar Estrada100% (2)
- Symphonic Literature Syllabus Fall 2019Document8 pagesSymphonic Literature Syllabus Fall 2019Shawn SherwoodNo ratings yet
- Test Bank For Sociology For The 21st Century Census Update 5th Edition Tim CurryDocument10 pagesTest Bank For Sociology For The 21st Century Census Update 5th Edition Tim CurryNathan Cook100% (30)
- Tenant Application Form: nts/mshda/EDP - Contact - List - 002 - 696637 - 7 PDFDocument5 pagesTenant Application Form: nts/mshda/EDP - Contact - List - 002 - 696637 - 7 PDFCaleb HollowayNo ratings yet
- Comparative Economic Development - Pakistan and BangladeshDocument14 pagesComparative Economic Development - Pakistan and BangladeshUsman Bin Younas100% (1)
- South Carolina Department of Health and Human Services Application For South Carolina Healthy ConnectionsDocument6 pagesSouth Carolina Department of Health and Human Services Application For South Carolina Healthy ConnectionsJames KirkpatrickNo ratings yet
- DS 160 - QuestionnaireDocument9 pagesDS 160 - QuestionnaireChristian MoralesNo ratings yet
- AFBSummary 820867071Document11 pagesAFBSummary 820867071williamsdareshaNo ratings yet
- Liheap ApplicationDocument10 pagesLiheap ApplicationSon BurnyoazNo ratings yet
- Us Visa Application FormDocument6 pagesUs Visa Application Forminfo786primeNo ratings yet
- Open US VISA FORM EMPTY ALLDocument7 pagesOpen US VISA FORM EMPTY ALLo1No ratings yet
- Form US VISA HAL Updated10122022Document7 pagesForm US VISA HAL Updated10122022Hendro NuryahyaNo ratings yet
- Us Tourist Visa FormDocument8 pagesUs Tourist Visa FormMark MontañezNo ratings yet
- Tradução E Rascunho Do Formulário Ds 160 em Português - Passo A PassoDocument5 pagesTradução E Rascunho Do Formulário Ds 160 em Português - Passo A PassoBruno B. SilvaNo ratings yet
- Responsible Party: Montefiore Medical Group Patient Registration FormDocument2 pagesResponsible Party: Montefiore Medical Group Patient Registration FormJpt YapNo ratings yet
- Personal Information Form 06Document2 pagesPersonal Information Form 06Rizki AgustiantoNo ratings yet
- Adult HistoryDocument8 pagesAdult Historyapi-267215948No ratings yet
- Tourist Visa App FormDocument4 pagesTourist Visa App Formmcoled12No ratings yet
- AFBSummary 4437390Document12 pagesAFBSummary 4437390Jennifer Lee-AnnNo ratings yet
- Form 2Document4 pagesForm 2Tyrone StewartNo ratings yet
- 1.formal ApplicationDocument8 pages1.formal ApplicationNaturalBite ChefNo ratings yet
- Draft of Online Us Nonimmigrant Visa FormDocument4 pagesDraft of Online Us Nonimmigrant Visa Formjobert de jesusNo ratings yet
- Health Care Application 2547388Document9 pagesHealth Care Application 2547388benwalterofarrellNo ratings yet
- ACCESS Florida: Benefits InformationDocument10 pagesACCESS Florida: Benefits InformationAngel Daniel PuppoNo ratings yet
- 2 - Admission Form - 07.04.21Document3 pages2 - Admission Form - 07.04.21Hassan ShahzadNo ratings yet
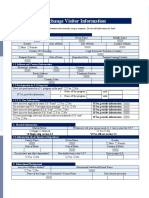
- Exchange Visitor InformationDocument3 pagesExchange Visitor InformationPrathamesh ParabNo ratings yet
- DS 160 FormDocument8 pagesDS 160 FormJam del RosarioNo ratings yet
- Us Visa Updated Draft FormDocument8 pagesUs Visa Updated Draft FormLorenzo OngNo ratings yet
- SubmissionDocument4 pagesSubmissionfarishta.nasratNo ratings yet
- PERSONAL DATA FORM - Personal DetailsDocument3 pagesPERSONAL DATA FORM - Personal DetailsMORSHEDNo ratings yet
- Employment ApplicationDocument3 pagesEmployment ApplicationkualakububharuNo ratings yet
- U.S. Visa Application Form Questionnaire: SECURITY QUESTION: Please Select One and Place AnswerDocument8 pagesU.S. Visa Application Form Questionnaire: SECURITY QUESTION: Please Select One and Place AnswerArielle NicoleNo ratings yet
- ACCESS Florida: Benefits InformationDocument8 pagesACCESS Florida: Benefits InformationCrystal HernandezNo ratings yet
- DS 160Document5 pagesDS 160Bert SantosNo ratings yet
- Access ControllerDocument4 pagesAccess Controllersumaiyatabassum2006No ratings yet
- Reverse Transfer ApplicationDocument4 pagesReverse Transfer ApplicationAbhishek SharmaNo ratings yet
- Us Visa Questionnaire: Personal InformationDocument5 pagesUs Visa Questionnaire: Personal InformationmyieNo ratings yet
- Access Florida Application Details 810968014Document11 pagesAccess Florida Application Details 810968014Samantha DuffNo ratings yet
- Unam 2Document1 pageUnam 2qualityrepeatNo ratings yet
- Visa Form B1-B2 (Updated)Document4 pagesVisa Form B1-B2 (Updated)bahram1pkNo ratings yet
- DS 260 Fillable FormDocument11 pagesDS 260 Fillable FormRandy EncomiendaNo ratings yet
- Asylum Support Application Form ASF1Document36 pagesAsylum Support Application Form ASF1Eğitime Destek GrubuNo ratings yet
- Ca Potential Client Intake FormDocument5 pagesCa Potential Client Intake Formbash shangNo ratings yet
- Information Pertaining To The Applicant: Family HistoryDocument8 pagesInformation Pertaining To The Applicant: Family Historyy.jabariNo ratings yet
- Additional InformationDocument7 pagesAdditional InformationDivina GarciaNo ratings yet
- U.S Visa Questioner: Personal, Address, Phone, and Passport/Travel Document InformationDocument4 pagesU.S Visa Questioner: Personal, Address, Phone, and Passport/Travel Document InformationAnonymous ku7POqvKNo ratings yet
- US Visa Questionnaire For Non Immigrant App 003Document5 pagesUS Visa Questionnaire For Non Immigrant App 003Pam Ponio-MacapugayNo ratings yet
- China Visa QuestionnaireDocument5 pagesChina Visa Questionnairepmd20190707No ratings yet
- Asylum Support Application Form ASF1Document36 pagesAsylum Support Application Form ASF1cococatelulNo ratings yet
- Fy AppDocument7 pagesFy AppTadiwa ChikatiNo ratings yet
- LIHEAPLIHWAP Application FY23 FinalUpdated Applicant Rights 912202285Document9 pagesLIHEAPLIHWAP Application FY23 FinalUpdated Applicant Rights 912202285yuly.montoyaNo ratings yet
- Formato DS-160 RevisionDocument6 pagesFormato DS-160 Revisionvic3edw100% (2)
- Vocational Rehabilitation Referral FormDocument1 pageVocational Rehabilitation Referral Formdavjazz16No ratings yet
- Usa Application Form - New - 31052019Document5 pagesUsa Application Form - New - 31052019Shivam MishraNo ratings yet
- Access Florida Application Details 320460282Document8 pagesAccess Florida Application Details 320460282Javier MazparroteNo ratings yet
- Ngala br2 HhregistrationDocument4 pagesNgala br2 HhregistrationAbdullahi MustaphaNo ratings yet
- Office of Unemployment Insurance OperationsDocument4 pagesOffice of Unemployment Insurance OperationsTaylor LynnNo ratings yet
- Degree Application Form - Page 1: Srija Anand, Computer Science & Engineering M.S.,, Fall 2023Document7 pagesDegree Application Form - Page 1: Srija Anand, Computer Science & Engineering M.S.,, Fall 2023Srija AnandNo ratings yet
- Mandela Washington Fellowship Application - Mercy-Aisha IliyaDocument5 pagesMandela Washington Fellowship Application - Mercy-Aisha IliyaAmos MainaNo ratings yet
- PDF SAMPLE - DO NOT SUBMIT - Knight-Hennessy Scholars Application 2023Document40 pagesPDF SAMPLE - DO NOT SUBMIT - Knight-Hennessy Scholars Application 2023begna bileNo ratings yet
- Consular Electronic Application Center - Print ApplicationDocument6 pagesConsular Electronic Application Center - Print Applicationdesikudi9000No ratings yet
- CCCApplicationFinal GrossmontCollegeDocument3 pagesCCCApplicationFinal GrossmontCollegeShirley BrizuelaNo ratings yet
- US Immigration Exam Study Guide in English and Albanian: Study Guides for the US Immigration TestFrom EverandUS Immigration Exam Study Guide in English and Albanian: Study Guides for the US Immigration TestNo ratings yet
- contentdamcenteneSunshinepdfsMMA Reg4 PDFDocument501 pagescontentdamcenteneSunshinepdfsMMA Reg4 PDFShawn SherwoodNo ratings yet
- April 9, 2023 - ChoirDocument1 pageApril 9, 2023 - ChoirShawn SherwoodNo ratings yet
- AtkinsonDocument10 pagesAtkinsonShawn SherwoodNo ratings yet
- Sponsorship FormDocument2 pagesSponsorship FormShawn SherwoodNo ratings yet
- Sponsorship FormDocument2 pagesSponsorship FormShawn SherwoodNo ratings yet
- Brown Tonality and Form in Debussey PDFDocument18 pagesBrown Tonality and Form in Debussey PDFShawn SherwoodNo ratings yet
- Aesthetic Vs Praxial Music EducationDocument5 pagesAesthetic Vs Praxial Music EducationShawn Sherwood100% (1)
- Missa No. IX (Cum Jubilo) Translation PDFDocument1 pageMissa No. IX (Cum Jubilo) Translation PDFShawn SherwoodNo ratings yet
- Music SyllabusDocument6 pagesMusic SyllabusShawn SherwoodNo ratings yet
- RomanticismDocument2 pagesRomanticismbeckyinmnNo ratings yet
- Explaining The TrinityDocument3 pagesExplaining The TrinityAriellaNo ratings yet
- Advanced Vehicle Technologies, Autonomous Vehicles and CyclingDocument15 pagesAdvanced Vehicle Technologies, Autonomous Vehicles and CyclingGiampaolo PastorinoNo ratings yet
- CivilPro Cases 37 and 38 Full Texts - AyingDocument15 pagesCivilPro Cases 37 and 38 Full Texts - Ayingvienuell ayingNo ratings yet
- Last 6 Months RBI in News Part 2 NiharDocument6 pagesLast 6 Months RBI in News Part 2 NiharbuhhbubuhgNo ratings yet
- Banaszynski v. United States Government - Document No. 4Document2 pagesBanaszynski v. United States Government - Document No. 4Justia.comNo ratings yet
- A Reply To Prof Mark Tatz - Brian GallowayDocument5 pagesA Reply To Prof Mark Tatz - Brian GallowayAjit GargeshwariNo ratings yet
- CAR BLGF Covid Response UpdateDocument8 pagesCAR BLGF Covid Response UpdatenormanNo ratings yet
- Bitcoin Us $350,000 Palm Beach Research GroupDocument56 pagesBitcoin Us $350,000 Palm Beach Research GroupJose Castillo71% (7)
- Speech On The East India BillDocument21 pagesSpeech On The East India BillAnonymous 5bULbK100% (1)
- Site Visit Report - 6 TH SEM - DssDocument9 pagesSite Visit Report - 6 TH SEM - DssJuhi PatelNo ratings yet
- Doctrine of Revelation (Transcrição Das Aulas 1 À 10)Document91 pagesDoctrine of Revelation (Transcrição Das Aulas 1 À 10)Leandro ÁlissonNo ratings yet
- Heavy Duty and Static Dissipative Footwear With Mid-Sole DeviceDocument14 pagesHeavy Duty and Static Dissipative Footwear With Mid-Sole DeviceJenniferValleNo ratings yet
- I. Demographic Profile/Information Name: Theodore Robert Bundy (Ted Bundy) Age: 42Document5 pagesI. Demographic Profile/Information Name: Theodore Robert Bundy (Ted Bundy) Age: 42Maanne MandalNo ratings yet
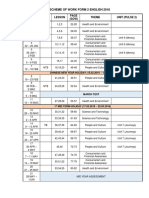
- Scheme of Work Form 2 English 2018: Week Types Lesson (SOW) Theme Unit (Pulse 2)Document2 pagesScheme of Work Form 2 English 2018: Week Types Lesson (SOW) Theme Unit (Pulse 2)Subramaniam Periannan100% (2)
- CIR Vs RhombusDocument2 pagesCIR Vs RhombusKateBarrionEspinosaNo ratings yet
- IA 6 Module 5-Edited-CorpuzDocument15 pagesIA 6 Module 5-Edited-CorpuzAngeline AlesnaNo ratings yet
- SV - ComplaintDocument72 pagesSV - ComplaintĐỗ Trà MyNo ratings yet
- Mindanao Development Authority v. CADocument14 pagesMindanao Development Authority v. CAKadzNitura0% (1)
- Freeman v. Grain Processing Corp., No. 13-0723 (Iowa June 13, 2014)Document63 pagesFreeman v. Grain Processing Corp., No. 13-0723 (Iowa June 13, 2014)RHTNo ratings yet
- Markov Chain PoetryDocument24 pagesMarkov Chain PoetryBea MillwardNo ratings yet
- 100 Earth Shattering Remote Sensing ApplicationsDocument145 pages100 Earth Shattering Remote Sensing ApplicationsENRIQUENo ratings yet
- Opening RemarksDocument2 pagesOpening Remarksjennelyn malayno100% (1)
- Holy Rosary - Sorrowful MysteriesDocument43 pagesHoly Rosary - Sorrowful MysteriesRhea AvilaNo ratings yet
- Definition:: Handover NotesDocument3 pagesDefinition:: Handover NotesRalkan KantonNo ratings yet
- Ethics SyllabusDocument5 pagesEthics SyllabusprincessNo ratings yet
- Information Before Stay BFDocument7 pagesInformation Before Stay BFBrat SiostraNo ratings yet
- Benjamin Franklin: Huge Pain in My... ExcerptDocument27 pagesBenjamin Franklin: Huge Pain in My... ExcerptDisney PublishingNo ratings yet