
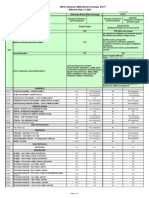
Dental MI EHB High 2024
Dental MI EHB High 2024
You might also like
- (Medicalstudyzone - Com) Medicine - Irfan Masood LatestDocument701 pages(Medicalstudyzone - Com) Medicine - Irfan Masood LatestMajid Ahmed FareaNo ratings yet
- Dental CodingDocument74 pagesDental CodingSakshi Bishnoi100% (2)
- NUR 3032 Immune System Study PlanDocument5 pagesNUR 3032 Immune System Study PlanThalia Fortune100% (1)
- Banco Kap. - CK 2Document1,099 pagesBanco Kap. - CK 2Lucas OrtizNo ratings yet
- Dental OH EHB Low 2024Document3 pagesDental OH EHB Low 2024Clifton JuraNo ratings yet
- Da Kim 01-23-2024 DD WEBDocument4 pagesDa Kim 01-23-2024 DD WEBhaWk FYZiXNo ratings yet
- Delta Dental Individual Enrollee Overview Flyer Plan III II Notre DameDocument2 pagesDelta Dental Individual Enrollee Overview Flyer Plan III II Notre DameObi-Wan KenobiNo ratings yet
- Premier 2000 NWDocument2 pagesPremier 2000 NWacolyteNo ratings yet
- Dental Plan Side-By-Side Comparison: Fast FactsDocument2 pagesDental Plan Side-By-Side Comparison: Fast FactsellenNo ratings yet
- Unitedhealthcare Dental Ppo Plan 2022 Summary of Benefits and CoverageDocument1 pageUnitedhealthcare Dental Ppo Plan 2022 Summary of Benefits and CoverageAdam CliftonNo ratings yet
- Delta Dental Plan Compare Highlight SheetDocument2 pagesDelta Dental Plan Compare Highlight SheetTiffany BarnesNo ratings yet
- 2022 Dental Plan BenefitsDocument1 page2022 Dental Plan BenefitsBrian ThurmondNo ratings yet
- Safari - Mar 11, 2019 at 11:00 PM PDFDocument1 pageSafari - Mar 11, 2019 at 11:00 PM PDFjohn jugoNo ratings yet
- Dental PrivilegioDocument11 pagesDental PrivilegioCarlos Andres ANo ratings yet
- Aetna Dental High DmoDocument5 pagesAetna Dental High DmoBeau PeskaNo ratings yet
- Dental Services Low Plan: PreventativeDocument2 pagesDental Services Low Plan: PreventativeIan PeabodyNo ratings yet
- 2021 2022 Aetna Justworks Dental Dmo Benefit SummaryDocument10 pages2021 2022 Aetna Justworks Dental Dmo Benefit SummarySunflowieNo ratings yet
- Dental by Design Broch 5.10Document16 pagesDental by Design Broch 5.10raviNo ratings yet
- 2022 1027 Ahs SD 1058-1 BroDocument8 pages2022 1027 Ahs SD 1058-1 BroFernanda VargasNo ratings yet
- 3610 - DENTAL Smart Health - Certificate-Revised 12 - 8 - 17-SalDocument28 pages3610 - DENTAL Smart Health - Certificate-Revised 12 - 8 - 17-SalOkolokin JohnsonNo ratings yet
- Snap Guardian Dental Plan Summary 2022Document4 pagesSnap Guardian Dental Plan Summary 2022Samson FungNo ratings yet
- 2021 2022 Aetna Justworks Dental Low Ppo 3 Benefit SummaryDocument10 pages2021 2022 Aetna Justworks Dental Low Ppo 3 Benefit SummarySunflowieNo ratings yet
- Cod Capitol 6 Nume Capitol (Engleza) Dental Services Nume Capitol (Romana) Servicii DentareDocument15 pagesCod Capitol 6 Nume Capitol (Engleza) Dental Services Nume Capitol (Romana) Servicii DentareMihaela VelcuNo ratings yet
- Ottonova Highlights For Dental InsuranceDocument2 pagesOttonova Highlights For Dental Insurancetomislavdrvar798No ratings yet
- Dental AwarenessDocument100 pagesDental AwarenessShourya HegdeNo ratings yet
- Rite Dentist-Studio CityDocument4 pagesRite Dentist-Studio Cityapi-731924299No ratings yet
- List of DentistsDocument21 pagesList of DentistsSaurabh Gupta100% (1)
- Trifold BrochureDocument2 pagesTrifold BrochureRendanLumbertNo ratings yet
- 2021 - Life, Dental, Vision PacketDocument12 pages2021 - Life, Dental, Vision PacketEberNo ratings yet
- 2011 Delta Dental General MarketingDocument1 page2011 Delta Dental General MarketingKristieNo ratings yet
- Epidemiology, Aetiology and Prevention of Oral CancerDocument9 pagesEpidemiology, Aetiology and Prevention of Oral Cancerpemirafkgunair 2020No ratings yet
- What Happens During A Routine Dental Checkup?: Say Hello To Your ReceptionistDocument1 pageWhat Happens During A Routine Dental Checkup?: Say Hello To Your ReceptionistAishani MeggiNo ratings yet
- Ottonova Coverage For Dental InsuranceDocument3 pagesOttonova Coverage For Dental Insurancetomislavdrvar798No ratings yet
- Generic Open Enrollment KitDocument22 pagesGeneric Open Enrollment KitSteve BarrowsNo ratings yet
- BDA Advice Tooth WhiteningDocument3 pagesBDA Advice Tooth WhiteningMariam Waseem0% (1)
- Cubierta Dental D-611 P.ideal C.P. 2Document4 pagesCubierta Dental D-611 P.ideal C.P. 2JessicaNo ratings yet
- BlueDental Copayment QF Plan BrochureDocument4 pagesBlueDental Copayment QF Plan BrochureJoshua JohnsonNo ratings yet
- DentalDocument3 pagesDentalCarl WiltNo ratings yet
- Delta Dental of California - Dental Ppo 12Document2 pagesDelta Dental of California - Dental Ppo 12api-252555369No ratings yet
- One Arch Braces & Pain Free Dentist London - Dental-SpaDocument2 pagesOne Arch Braces & Pain Free Dentist London - Dental-SpadentalspaukNo ratings yet
- Aetna Y0001 H5521 380 PR25 SB24 M 2024 SF20240425Document23 pagesAetna Y0001 H5521 380 PR25 SB24 M 2024 SF20240425kevin.mccreaNo ratings yet
- Keep Smiling: Delta Dental PPO™Document2 pagesKeep Smiling: Delta Dental PPO™olimaziNo ratings yet
- 888674a Ooc Cigna Dental 1500 CaDocument13 pages888674a Ooc Cigna Dental 1500 CaImmanuel TaquonNo ratings yet
- MEDICARDDocument19 pagesMEDICARDSrcdc CooperativeNo ratings yet
- Guardian - Dental PPO Plan Summary 2022Document4 pagesGuardian - Dental PPO Plan Summary 2022Jessi ChallagullaNo ratings yet
- Avant Dental Welness ProgramDocument4 pagesAvant Dental Welness Programskarthik011No ratings yet
- Rite Dentist-North HollywoodDocument3 pagesRite Dentist-North Hollywoodapi-731909862No ratings yet
- 2003 Delta SumDocument1 page2003 Delta SumbpracticalNo ratings yet
- Tooth WhiteningDocument3 pagesTooth WhiteningrizwanNo ratings yet
- Slater Inc Dental EnglishDocument4 pagesSlater Inc Dental Englishapi-531507901No ratings yet
- LSG DentalDocument1 pageLSG Dentalres6250No ratings yet
- Hospital ProposalDocument8 pagesHospital ProposalMurali MohanNo ratings yet
- Carefree: Show Your Card. Save Your MoneyDocument7 pagesCarefree: Show Your Card. Save Your MoneyMichelle Angelina CortezNo ratings yet
- LoyaltyCard 2016 July11 PDFDocument14 pagesLoyaltyCard 2016 July11 PDFchico_belandresNo ratings yet
- Epidemiology, Aetiology and Prevention of Periodontal Disease (Recovered)Document8 pagesEpidemiology, Aetiology and Prevention of Periodontal Disease (Recovered)pemirafkgunair 2020No ratings yet
- Outpatient One Pager Version 1.0 Apr 20Document1 pageOutpatient One Pager Version 1.0 Apr 20naval730107No ratings yet
- Our Mission: Yp Yp Yp Yp Yp Yp Yp YpDocument3 pagesOur Mission: Yp Yp Yp Yp Yp Yp Yp YpalshadNo ratings yet
- Dental Plans and Rates: Bay AreaDocument6 pagesDental Plans and Rates: Bay AreaJDanaNo ratings yet
- Welcome To Lifetime Smiles Dental Hygiene ClinicDocument7 pagesWelcome To Lifetime Smiles Dental Hygiene CliniclifetimesmileNo ratings yet
- Dental Wellness Plan: Our Exclusive In-House Savings PlanDocument1 pageDental Wellness Plan: Our Exclusive In-House Savings PlanJamez MattauzNo ratings yet
- Welcome To Lifetime Smiles Dental Hygiene ClinicDocument7 pagesWelcome To Lifetime Smiles Dental Hygiene CliniclifetimesmileNo ratings yet
- Your Path to Healthier Dentistry: A Holistic Approach to Keeping Your Teeth for a LifetimeFrom EverandYour Path to Healthier Dentistry: A Holistic Approach to Keeping Your Teeth for a LifetimeRating: 5 out of 5 stars5/5 (1)
- DENTURES: The Ultimate Guide to Dentures & Denture Care for a Beautifully Restored SmileFrom EverandDENTURES: The Ultimate Guide to Dentures & Denture Care for a Beautifully Restored SmileNo ratings yet
- Dental - Docushare-App-12 - 10 - 2023 6 - 29 - 09 PMDocument6 pagesDental - Docushare-App-12 - 10 - 2023 6 - 29 - 09 PMClifton JuraNo ratings yet
- HACCP WATER FinalDocument68 pagesHACCP WATER FinalClifton JuraNo ratings yet
- 2001 Dewettincketal HACCPDocument9 pages2001 Dewettincketal HACCPClifton JuraNo ratings yet
- IBWA MODEL CODE 2016 Rev 02 2016Document30 pagesIBWA MODEL CODE 2016 Rev 02 2016Katherine KimNo ratings yet
- HACCP FOR WATER OPERATIONS AN OPERATORS EXPERIENCE - GrahamMcKeonDocument6 pagesHACCP FOR WATER OPERATIONS AN OPERATORS EXPERIENCE - GrahamMcKeonClifton JuraNo ratings yet
- SilosDocument3 pagesSilosapi-548205221100% (1)
- Vazno IstrazivanjeDocument2 pagesVazno IstrazivanjeDomagoj BažantNo ratings yet
- Blood Bank UnitDocument9 pagesBlood Bank UnitMary CabalceNo ratings yet
- Drug StudyDocument8 pagesDrug StudyTheresa Reyes De JesusNo ratings yet
- Daftar Harga Produk Generik 2022 New (DITEMPEL)Document1 pageDaftar Harga Produk Generik 2022 New (DITEMPEL)Ade IrawanNo ratings yet
- 8776 00Document30 pages8776 00Elma MufidhaNo ratings yet
- Biodata Dr. P. Sirohi - 2021.06.16Document10 pagesBiodata Dr. P. Sirohi - 2021.06.16kvpy iisc bangloreNo ratings yet
- PRC LeahDocument8 pagesPRC LeahInes Hamoy JunioNo ratings yet
- Landrus Unit IIDocument4 pagesLandrus Unit IIRobert ContiNo ratings yet
- Patient Rights Patient ResponsibilitiesDocument1 pagePatient Rights Patient ResponsibilitiesHassan KhanNo ratings yet
- Phillipine Herbal MedicineDocument23 pagesPhillipine Herbal MedicineCENTHREE MAGALLANESNo ratings yet
- MVS Pulmonary AuscultationDocument8 pagesMVS Pulmonary Auscultationvashini9151No ratings yet
- Foreign Body in Eye Icd 10 - Google SearchDocument1 pageForeign Body in Eye Icd 10 - Google SearchAnandita ParamastutiNo ratings yet
- Suzhou Vocaional University Courses NAVTTC OnlineDocument10 pagesSuzhou Vocaional University Courses NAVTTC Onlineshafiq rehmanNo ratings yet
- Republic Act No. 9173: The Philippine Nursing Act O F 2 0 0 2 Presented By: Judith Leano RNDocument167 pagesRepublic Act No. 9173: The Philippine Nursing Act O F 2 0 0 2 Presented By: Judith Leano RNJohnasse Sebastian NavalNo ratings yet
- Ref. Safety Guide On "Safe Working at Height and Fragile Roof" No. NPCIL/04700/CE (IS&F) /2006/M/139, Dated July 19, 2006Document2 pagesRef. Safety Guide On "Safe Working at Height and Fragile Roof" No. NPCIL/04700/CE (IS&F) /2006/M/139, Dated July 19, 2006Bhagat DeepakNo ratings yet
- Physical Examination of The PatientDocument9 pagesPhysical Examination of The PatientzbrojkoNo ratings yet
- Medication Errors - Where Do They Happen - The Pharmaceutical JournalDocument7 pagesMedication Errors - Where Do They Happen - The Pharmaceutical JournalAre Pee EtcNo ratings yet
- Systemic Light Chain Amyloidosis: NCCN Clinical Practice Guidelines in Oncology (NCCN Guidelines)Document26 pagesSystemic Light Chain Amyloidosis: NCCN Clinical Practice Guidelines in Oncology (NCCN Guidelines)Adina StemateNo ratings yet
- Occupational English Test: Writing Sub-Test: Nursing Time Allowed: Reading Time: 5 Minutes Writing Time: 40 MinutesDocument2 pagesOccupational English Test: Writing Sub-Test: Nursing Time Allowed: Reading Time: 5 Minutes Writing Time: 40 MinutesAnit XingNo ratings yet
- Barlet Juliette Optimized 3d Flair Sequences ToDocument10 pagesBarlet Juliette Optimized 3d Flair Sequences ToFontas LadoprakopoulosNo ratings yet
- Submental Intubation in Patients With Complex Maxillofacial InjuriesDocument4 pagesSubmental Intubation in Patients With Complex Maxillofacial InjuriesMudassar SattarNo ratings yet
- Camus 2016Document7 pagesCamus 2016Dra CarrascoNo ratings yet
- Vascular DisordersDocument13 pagesVascular DisordersMichelle Dona MirallesNo ratings yet
- Journal of Hematology & Oncology: A Journal Open To AllDocument2 pagesJournal of Hematology & Oncology: A Journal Open To AllKay BristolNo ratings yet
- Obstetric EmbolismDocument81 pagesObstetric Embolismmiss_izzniNo ratings yet
- Form C AuthorizationRequestForm PDFDocument4 pagesForm C AuthorizationRequestForm PDFKalaimani SNo ratings yet




























































































Download as pdf or txt
You might also like
- (Medicalstudyzone - Com) Medicine - Irfan Masood LatestDocument701 pages(Medicalstudyzone - Com) Medicine - Irfan Masood LatestMajid Ahmed FareaNo ratings yet
- Dental CodingDocument74 pagesDental CodingSakshi Bishnoi100% (2)
- NUR 3032 Immune System Study PlanDocument5 pagesNUR 3032 Immune System Study PlanThalia Fortune100% (1)
- Banco Kap. - CK 2Document1,099 pagesBanco Kap. - CK 2Lucas OrtizNo ratings yet
- Dental OH EHB Low 2024Document3 pagesDental OH EHB Low 2024Clifton JuraNo ratings yet
- Da Kim 01-23-2024 DD WEBDocument4 pagesDa Kim 01-23-2024 DD WEBhaWk FYZiXNo ratings yet
- Delta Dental Individual Enrollee Overview Flyer Plan III II Notre DameDocument2 pagesDelta Dental Individual Enrollee Overview Flyer Plan III II Notre DameObi-Wan KenobiNo ratings yet
- Premier 2000 NWDocument2 pagesPremier 2000 NWacolyteNo ratings yet
- Dental Plan Side-By-Side Comparison: Fast FactsDocument2 pagesDental Plan Side-By-Side Comparison: Fast FactsellenNo ratings yet
- Unitedhealthcare Dental Ppo Plan 2022 Summary of Benefits and CoverageDocument1 pageUnitedhealthcare Dental Ppo Plan 2022 Summary of Benefits and CoverageAdam CliftonNo ratings yet
- Delta Dental Plan Compare Highlight SheetDocument2 pagesDelta Dental Plan Compare Highlight SheetTiffany BarnesNo ratings yet
- 2022 Dental Plan BenefitsDocument1 page2022 Dental Plan BenefitsBrian ThurmondNo ratings yet
- Safari - Mar 11, 2019 at 11:00 PM PDFDocument1 pageSafari - Mar 11, 2019 at 11:00 PM PDFjohn jugoNo ratings yet
- Dental PrivilegioDocument11 pagesDental PrivilegioCarlos Andres ANo ratings yet
- Aetna Dental High DmoDocument5 pagesAetna Dental High DmoBeau PeskaNo ratings yet
- Dental Services Low Plan: PreventativeDocument2 pagesDental Services Low Plan: PreventativeIan PeabodyNo ratings yet
- 2021 2022 Aetna Justworks Dental Dmo Benefit SummaryDocument10 pages2021 2022 Aetna Justworks Dental Dmo Benefit SummarySunflowieNo ratings yet
- Dental by Design Broch 5.10Document16 pagesDental by Design Broch 5.10raviNo ratings yet
- 2022 1027 Ahs SD 1058-1 BroDocument8 pages2022 1027 Ahs SD 1058-1 BroFernanda VargasNo ratings yet
- 3610 - DENTAL Smart Health - Certificate-Revised 12 - 8 - 17-SalDocument28 pages3610 - DENTAL Smart Health - Certificate-Revised 12 - 8 - 17-SalOkolokin JohnsonNo ratings yet
- Snap Guardian Dental Plan Summary 2022Document4 pagesSnap Guardian Dental Plan Summary 2022Samson FungNo ratings yet
- 2021 2022 Aetna Justworks Dental Low Ppo 3 Benefit SummaryDocument10 pages2021 2022 Aetna Justworks Dental Low Ppo 3 Benefit SummarySunflowieNo ratings yet
- Cod Capitol 6 Nume Capitol (Engleza) Dental Services Nume Capitol (Romana) Servicii DentareDocument15 pagesCod Capitol 6 Nume Capitol (Engleza) Dental Services Nume Capitol (Romana) Servicii DentareMihaela VelcuNo ratings yet
- Ottonova Highlights For Dental InsuranceDocument2 pagesOttonova Highlights For Dental Insurancetomislavdrvar798No ratings yet
- Dental AwarenessDocument100 pagesDental AwarenessShourya HegdeNo ratings yet
- Rite Dentist-Studio CityDocument4 pagesRite Dentist-Studio Cityapi-731924299No ratings yet
- List of DentistsDocument21 pagesList of DentistsSaurabh Gupta100% (1)
- Trifold BrochureDocument2 pagesTrifold BrochureRendanLumbertNo ratings yet
- 2021 - Life, Dental, Vision PacketDocument12 pages2021 - Life, Dental, Vision PacketEberNo ratings yet
- 2011 Delta Dental General MarketingDocument1 page2011 Delta Dental General MarketingKristieNo ratings yet
- Epidemiology, Aetiology and Prevention of Oral CancerDocument9 pagesEpidemiology, Aetiology and Prevention of Oral Cancerpemirafkgunair 2020No ratings yet
- What Happens During A Routine Dental Checkup?: Say Hello To Your ReceptionistDocument1 pageWhat Happens During A Routine Dental Checkup?: Say Hello To Your ReceptionistAishani MeggiNo ratings yet
- Ottonova Coverage For Dental InsuranceDocument3 pagesOttonova Coverage For Dental Insurancetomislavdrvar798No ratings yet
- Generic Open Enrollment KitDocument22 pagesGeneric Open Enrollment KitSteve BarrowsNo ratings yet
- BDA Advice Tooth WhiteningDocument3 pagesBDA Advice Tooth WhiteningMariam Waseem0% (1)
- Cubierta Dental D-611 P.ideal C.P. 2Document4 pagesCubierta Dental D-611 P.ideal C.P. 2JessicaNo ratings yet
- BlueDental Copayment QF Plan BrochureDocument4 pagesBlueDental Copayment QF Plan BrochureJoshua JohnsonNo ratings yet
- DentalDocument3 pagesDentalCarl WiltNo ratings yet
- Delta Dental of California - Dental Ppo 12Document2 pagesDelta Dental of California - Dental Ppo 12api-252555369No ratings yet
- One Arch Braces & Pain Free Dentist London - Dental-SpaDocument2 pagesOne Arch Braces & Pain Free Dentist London - Dental-SpadentalspaukNo ratings yet
- Aetna Y0001 H5521 380 PR25 SB24 M 2024 SF20240425Document23 pagesAetna Y0001 H5521 380 PR25 SB24 M 2024 SF20240425kevin.mccreaNo ratings yet
- Keep Smiling: Delta Dental PPO™Document2 pagesKeep Smiling: Delta Dental PPO™olimaziNo ratings yet
- 888674a Ooc Cigna Dental 1500 CaDocument13 pages888674a Ooc Cigna Dental 1500 CaImmanuel TaquonNo ratings yet
- MEDICARDDocument19 pagesMEDICARDSrcdc CooperativeNo ratings yet
- Guardian - Dental PPO Plan Summary 2022Document4 pagesGuardian - Dental PPO Plan Summary 2022Jessi ChallagullaNo ratings yet
- Avant Dental Welness ProgramDocument4 pagesAvant Dental Welness Programskarthik011No ratings yet
- Rite Dentist-North HollywoodDocument3 pagesRite Dentist-North Hollywoodapi-731909862No ratings yet
- 2003 Delta SumDocument1 page2003 Delta SumbpracticalNo ratings yet
- Tooth WhiteningDocument3 pagesTooth WhiteningrizwanNo ratings yet
- Slater Inc Dental EnglishDocument4 pagesSlater Inc Dental Englishapi-531507901No ratings yet
- LSG DentalDocument1 pageLSG Dentalres6250No ratings yet
- Hospital ProposalDocument8 pagesHospital ProposalMurali MohanNo ratings yet
- Carefree: Show Your Card. Save Your MoneyDocument7 pagesCarefree: Show Your Card. Save Your MoneyMichelle Angelina CortezNo ratings yet
- LoyaltyCard 2016 July11 PDFDocument14 pagesLoyaltyCard 2016 July11 PDFchico_belandresNo ratings yet
- Epidemiology, Aetiology and Prevention of Periodontal Disease (Recovered)Document8 pagesEpidemiology, Aetiology and Prevention of Periodontal Disease (Recovered)pemirafkgunair 2020No ratings yet
- Outpatient One Pager Version 1.0 Apr 20Document1 pageOutpatient One Pager Version 1.0 Apr 20naval730107No ratings yet
- Our Mission: Yp Yp Yp Yp Yp Yp Yp YpDocument3 pagesOur Mission: Yp Yp Yp Yp Yp Yp Yp YpalshadNo ratings yet
- Dental Plans and Rates: Bay AreaDocument6 pagesDental Plans and Rates: Bay AreaJDanaNo ratings yet
- Welcome To Lifetime Smiles Dental Hygiene ClinicDocument7 pagesWelcome To Lifetime Smiles Dental Hygiene CliniclifetimesmileNo ratings yet
- Dental Wellness Plan: Our Exclusive In-House Savings PlanDocument1 pageDental Wellness Plan: Our Exclusive In-House Savings PlanJamez MattauzNo ratings yet
- Welcome To Lifetime Smiles Dental Hygiene ClinicDocument7 pagesWelcome To Lifetime Smiles Dental Hygiene CliniclifetimesmileNo ratings yet
- Your Path to Healthier Dentistry: A Holistic Approach to Keeping Your Teeth for a LifetimeFrom EverandYour Path to Healthier Dentistry: A Holistic Approach to Keeping Your Teeth for a LifetimeRating: 5 out of 5 stars5/5 (1)
- DENTURES: The Ultimate Guide to Dentures & Denture Care for a Beautifully Restored SmileFrom EverandDENTURES: The Ultimate Guide to Dentures & Denture Care for a Beautifully Restored SmileNo ratings yet
- Dental - Docushare-App-12 - 10 - 2023 6 - 29 - 09 PMDocument6 pagesDental - Docushare-App-12 - 10 - 2023 6 - 29 - 09 PMClifton JuraNo ratings yet
- HACCP WATER FinalDocument68 pagesHACCP WATER FinalClifton JuraNo ratings yet
- 2001 Dewettincketal HACCPDocument9 pages2001 Dewettincketal HACCPClifton JuraNo ratings yet
- IBWA MODEL CODE 2016 Rev 02 2016Document30 pagesIBWA MODEL CODE 2016 Rev 02 2016Katherine KimNo ratings yet
- HACCP FOR WATER OPERATIONS AN OPERATORS EXPERIENCE - GrahamMcKeonDocument6 pagesHACCP FOR WATER OPERATIONS AN OPERATORS EXPERIENCE - GrahamMcKeonClifton JuraNo ratings yet
- SilosDocument3 pagesSilosapi-548205221100% (1)
- Vazno IstrazivanjeDocument2 pagesVazno IstrazivanjeDomagoj BažantNo ratings yet
- Blood Bank UnitDocument9 pagesBlood Bank UnitMary CabalceNo ratings yet
- Drug StudyDocument8 pagesDrug StudyTheresa Reyes De JesusNo ratings yet
- Daftar Harga Produk Generik 2022 New (DITEMPEL)Document1 pageDaftar Harga Produk Generik 2022 New (DITEMPEL)Ade IrawanNo ratings yet
- 8776 00Document30 pages8776 00Elma MufidhaNo ratings yet
- Biodata Dr. P. Sirohi - 2021.06.16Document10 pagesBiodata Dr. P. Sirohi - 2021.06.16kvpy iisc bangloreNo ratings yet
- PRC LeahDocument8 pagesPRC LeahInes Hamoy JunioNo ratings yet
- Landrus Unit IIDocument4 pagesLandrus Unit IIRobert ContiNo ratings yet
- Patient Rights Patient ResponsibilitiesDocument1 pagePatient Rights Patient ResponsibilitiesHassan KhanNo ratings yet
- Phillipine Herbal MedicineDocument23 pagesPhillipine Herbal MedicineCENTHREE MAGALLANESNo ratings yet
- MVS Pulmonary AuscultationDocument8 pagesMVS Pulmonary Auscultationvashini9151No ratings yet
- Foreign Body in Eye Icd 10 - Google SearchDocument1 pageForeign Body in Eye Icd 10 - Google SearchAnandita ParamastutiNo ratings yet
- Suzhou Vocaional University Courses NAVTTC OnlineDocument10 pagesSuzhou Vocaional University Courses NAVTTC Onlineshafiq rehmanNo ratings yet
- Republic Act No. 9173: The Philippine Nursing Act O F 2 0 0 2 Presented By: Judith Leano RNDocument167 pagesRepublic Act No. 9173: The Philippine Nursing Act O F 2 0 0 2 Presented By: Judith Leano RNJohnasse Sebastian NavalNo ratings yet
- Ref. Safety Guide On "Safe Working at Height and Fragile Roof" No. NPCIL/04700/CE (IS&F) /2006/M/139, Dated July 19, 2006Document2 pagesRef. Safety Guide On "Safe Working at Height and Fragile Roof" No. NPCIL/04700/CE (IS&F) /2006/M/139, Dated July 19, 2006Bhagat DeepakNo ratings yet
- Physical Examination of The PatientDocument9 pagesPhysical Examination of The PatientzbrojkoNo ratings yet
- Medication Errors - Where Do They Happen - The Pharmaceutical JournalDocument7 pagesMedication Errors - Where Do They Happen - The Pharmaceutical JournalAre Pee EtcNo ratings yet
- Systemic Light Chain Amyloidosis: NCCN Clinical Practice Guidelines in Oncology (NCCN Guidelines)Document26 pagesSystemic Light Chain Amyloidosis: NCCN Clinical Practice Guidelines in Oncology (NCCN Guidelines)Adina StemateNo ratings yet
- Occupational English Test: Writing Sub-Test: Nursing Time Allowed: Reading Time: 5 Minutes Writing Time: 40 MinutesDocument2 pagesOccupational English Test: Writing Sub-Test: Nursing Time Allowed: Reading Time: 5 Minutes Writing Time: 40 MinutesAnit XingNo ratings yet
- Barlet Juliette Optimized 3d Flair Sequences ToDocument10 pagesBarlet Juliette Optimized 3d Flair Sequences ToFontas LadoprakopoulosNo ratings yet
- Submental Intubation in Patients With Complex Maxillofacial InjuriesDocument4 pagesSubmental Intubation in Patients With Complex Maxillofacial InjuriesMudassar SattarNo ratings yet
- Camus 2016Document7 pagesCamus 2016Dra CarrascoNo ratings yet
- Vascular DisordersDocument13 pagesVascular DisordersMichelle Dona MirallesNo ratings yet
- Journal of Hematology & Oncology: A Journal Open To AllDocument2 pagesJournal of Hematology & Oncology: A Journal Open To AllKay BristolNo ratings yet
- Obstetric EmbolismDocument81 pagesObstetric Embolismmiss_izzniNo ratings yet
- Form C AuthorizationRequestForm PDFDocument4 pagesForm C AuthorizationRequestForm PDFKalaimani SNo ratings yet