Download as pdf or txt
You might also like
- How To BitcoinDocument220 pagesHow To Bitcoindash100% (5)
- Revit 2020 Fundamentals For StructureDocument62 pagesRevit 2020 Fundamentals For StructureNoureddine100% (1)
- Predicting Progression of Age-Related Macular Degeneration From Fundus Images Using Deep LearningDocument27 pagesPredicting Progression of Age-Related Macular Degeneration From Fundus Images Using Deep Learningzaynab adeolaNo ratings yet
- 2023 Owsley... Curcio Measure RMDADocument9 pages2023 Owsley... Curcio Measure RMDAsq.baoNo ratings yet
- Klein Et Al. - 2011 - Risk Assessment Model For Development of Advanced Age-Related Macular DegenerationDocument8 pagesKlein Et Al. - 2011 - Risk Assessment Model For Development of Advanced Age-Related Macular DegenerationKreAch3RNo ratings yet
- A Simplified Severity Scale For Age-Related Macular Degeneration AREDS Report No 18Document14 pagesA Simplified Severity Scale For Age-Related Macular Degeneration AREDS Report No 18aholmes172No ratings yet
- Deep-Learning-Based Automatic Computer-Aided Diagnosis System For Diabetic RetinopathyDocument17 pagesDeep-Learning-Based Automatic Computer-Aided Diagnosis System For Diabetic RetinopathyAsritha ReddyNo ratings yet
- Diabetic Retinopathy Detection Using Deep Learning Implementation PaperDocument13 pagesDiabetic Retinopathy Detection Using Deep Learning Implementation Paperpuneetoxi1919No ratings yet
- Multi-Class Retinal Diseases Detection Using Deep CNN With Minimal Memory Consumption PDFDocument11 pagesMulti-Class Retinal Diseases Detection Using Deep CNN With Minimal Memory Consumption PDFavinashkumar12110No ratings yet
- Brain Sciences: A Deep Siamese Convolution Neural Network For Multi-Class Classification of Alzheimer DiseaseDocument15 pagesBrain Sciences: A Deep Siamese Convolution Neural Network For Multi-Class Classification of Alzheimer DiseaseVictorvikkNo ratings yet
- RetiNet - Feature Extractor For Learning Patterns of Diabetic Retinopathy and Age-Related Macular Degeneration From Publicly Available DatasetsDocument6 pagesRetiNet - Feature Extractor For Learning Patterns of Diabetic Retinopathy and Age-Related Macular Degeneration From Publicly Available Datasetsgunanti1307No ratings yet
- An Interpretable Multiple Instance Approach For The Detection of Referable Diabetic Retinopathy in Fundus ImagesDocument15 pagesAn Interpretable Multiple Instance Approach For The Detection of Referable Diabetic Retinopathy in Fundus ImagesokuwobiNo ratings yet
- Owsley - RMDA 2 Year History.i2164-2591-6-3-15Document10 pagesOwsley - RMDA 2 Year History.i2164-2591-6-3-15sq.baoNo ratings yet
- Diabetic Retinopathy Detection Using SVMDocument10 pagesDiabetic Retinopathy Detection Using SVMIJRASETPublicationsNo ratings yet
- Author Proof Page Proof Auto 964959 7776243 4Document4 pagesAuthor Proof Page Proof Auto 964959 7776243 4KAREN VASQUEZNo ratings yet
- Detection of Severity Level of Diabetic Retinopathy Using Bag of Features ModelDocument8 pagesDetection of Severity Level of Diabetic Retinopathy Using Bag of Features ModelaaNo ratings yet
- Diagnosis of Diabetic Retinopathy Using Multi Level Set Segmentation Algorithm With Feature Extraction Using SVM With Selective FeaturesDocument16 pagesDiagnosis of Diabetic Retinopathy Using Multi Level Set Segmentation Algorithm With Feature Extraction Using SVM With Selective FeaturesSYED AYANNo ratings yet
- Diabetic Retinopathy Detection and Stage ClassificDocument32 pagesDiabetic Retinopathy Detection and Stage ClassificOscar Julian Perdomo CharryNo ratings yet
- The Age-Related Eye Disease Study (AREDS) - Design Implications AREDS Report No. 1 (Controlled Clinical Trials, Vol. 20, Issue 6) (1999)Document28 pagesThe Age-Related Eye Disease Study (AREDS) - Design Implications AREDS Report No. 1 (Controlled Clinical Trials, Vol. 20, Issue 6) (1999)Luisa Mayta PitmanNo ratings yet
- A Deep Feature-Based Real-Time System For Alzheimer Disease Stage DetectionDocument19 pagesA Deep Feature-Based Real-Time System For Alzheimer Disease Stage Detectionmozhganeutoop1998No ratings yet
- Using A Deep Learning Algorithm and Integrated Gradients Explanation To Assist Grading For Diabetic RetinopathyDocument13 pagesUsing A Deep Learning Algorithm and Integrated Gradients Explanation To Assist Grading For Diabetic RetinopathyMitcheel Lanas SozaNo ratings yet
- Healthcare 11 00863 CompressedDocument17 pagesHealthcare 11 00863 Compresseddarshanmythreya14No ratings yet
- Deep Learning Is Effective For Classifying Normal Versus Age-Related MacularDocument6 pagesDeep Learning Is Effective For Classifying Normal Versus Age-Related MacularNicolòNo ratings yet
- Uncertainty Aware and Explainable Diagnosis of Retinal DiseaseDocument10 pagesUncertainty Aware and Explainable Diagnosis of Retinal DiseaseokuwobiNo ratings yet
- LE Kumar Project Paper 3Document7 pagesLE Kumar Project Paper 3LIVAN KUMARNo ratings yet
- Using Transfer Learning For DiabeticDocument11 pagesUsing Transfer Learning For DiabeticNitinNo ratings yet
- Ocular Diseases Diagnosis in Fundus Images Using A Deep Learning: Approaches, Tools and Performance EvaluationDocument8 pagesOcular Diseases Diagnosis in Fundus Images Using A Deep Learning: Approaches, Tools and Performance EvaluationVarshhaNo ratings yet
- A Hybrid Convolutional Neural Network Model For Automatic Diabetic Retinopathy Classification From Fundus ImagesDocument10 pagesA Hybrid Convolutional Neural Network Model For Automatic Diabetic Retinopathy Classification From Fundus Imagesdalaisai1234No ratings yet
- Automated Classification of Age-Related Macular Degeneration From Optical Coherence Tomography Images Using Deep Learning ApproachDocument11 pagesAutomated Classification of Age-Related Macular Degeneration From Optical Coherence Tomography Images Using Deep Learning ApproachIAES IJAINo ratings yet
- s41598 023 32518 3Document13 pagess41598 023 32518 3Hello PtaiNo ratings yet
- A Survey of Feature Extraction in Dermoscopy Image Analysis of Skin CancerDocument14 pagesA Survey of Feature Extraction in Dermoscopy Image Analysis of Skin CancerSUMIT GANGWARNo ratings yet
- Deep Learning Approach For Early Detection of Alzheimer's DiseaseDocument17 pagesDeep Learning Approach For Early Detection of Alzheimer's DiseaseKIRAN ECENo ratings yet
- Assessment of Severity Level For Diabetic Macular PDFDocument8 pagesAssessment of Severity Level For Diabetic Macular PDFhaymanotNo ratings yet
- Early Diabetic Retinopathy Detection Using Deep LearningDocument7 pagesEarly Diabetic Retinopathy Detection Using Deep LearningIJRASETPublicationsNo ratings yet
- Helaly2021 Article DeepLearningApproachForEarlyDeDocument17 pagesHelaly2021 Article DeepLearningApproachForEarlyDemozhganeutoop1998No ratings yet
- Research Article: Ensemble Framework of Deep Cnns For Diabetic Retinopathy DetectionDocument11 pagesResearch Article: Ensemble Framework of Deep Cnns For Diabetic Retinopathy Detectionasma khanNo ratings yet
- Automatic Prediction of Diabetic Retinopathy and Glaucoma Through Retinal Image Analysis and Data Mining Techniques PDFDocument4 pagesAutomatic Prediction of Diabetic Retinopathy and Glaucoma Through Retinal Image Analysis and Data Mining Techniques PDFMohammad RofiiNo ratings yet
- Delineation of Blood Vessels in Pediatric Retinal Images Using Decision Trees-Based Ensemble ClassificationDocument17 pagesDelineation of Blood Vessels in Pediatric Retinal Images Using Decision Trees-Based Ensemble ClassificationJothibasu MarappanNo ratings yet
- Classification of The Clinical Images ForDocument10 pagesClassification of The Clinical Images ForHaleema ahsanNo ratings yet
- Genomics: Original ArticleDocument8 pagesGenomics: Original ArticleGOBINATH KNo ratings yet
- Grader Variability and The Importance of Reference Standards For Evaluating Machine Learning Models For Diabetic RetinopathyDocument23 pagesGrader Variability and The Importance of Reference Standards For Evaluating Machine Learning Models For Diabetic RetinopathyAstri HandayaniNo ratings yet
- Computer Methods and Prgrams in BiomedicineDocument11 pagesComputer Methods and Prgrams in BiomedicineHimashree KalitaNo ratings yet
- Harnessing The Power of Longitudinal Medical Imaging For Eye Disease Prognosis Using Transformer-Based Sequence ModelingDocument26 pagesHarnessing The Power of Longitudinal Medical Imaging For Eye Disease Prognosis Using Transformer-Based Sequence Modelinghoutatsu16No ratings yet
- Applsci 12 03358Document18 pagesApplsci 12 03358nha8378No ratings yet
- Computer Assisted Detection, Prognosis and Management of Diabetic RetinopathyDocument4 pagesComputer Assisted Detection, Prognosis and Management of Diabetic Retinopathyjurnal sajaNo ratings yet
- PIIS000293942200407XDocument13 pagesPIIS000293942200407XAnca Florina GaceaNo ratings yet
- Classification of Diabetic Maculopathy Based On Optical Coherence Tomography Images Using A Vision Transformer Model Bmjophth-2023-001423Document8 pagesClassification of Diabetic Maculopathy Based On Optical Coherence Tomography Images Using A Vision Transformer Model Bmjophth-2023-001423MarioNo ratings yet
- An Intelligent Alzheimer's Disease Diagnosis Method Using Unsupervised Feature LearningDocument16 pagesAn Intelligent Alzheimer's Disease Diagnosis Method Using Unsupervised Feature LearningKamran AhmedNo ratings yet
- SK-P2017 Article AMachineLearningEnsembleClassiDocument12 pagesSK-P2017 Article AMachineLearningEnsembleClassisaadiaNo ratings yet
- A Deep Transfer Learning Approach For Identification of Diabetic Retinopathy Using Data AugmentationDocument10 pagesA Deep Transfer Learning Approach For Identification of Diabetic Retinopathy Using Data AugmentationIAES IJAINo ratings yet
- Automated Classification of Diabetic Retinopathy Through Reliable Feature SelectionDocument19 pagesAutomated Classification of Diabetic Retinopathy Through Reliable Feature SelectionSangeethaNo ratings yet
- 2017 EstevaDocument12 pages2017 EstevawytlandpvtltdNo ratings yet
- Published Paper - Deep Learning With A Novel Concoction Loss Function For IdenticationDocument19 pagesPublished Paper - Deep Learning With A Novel Concoction Loss Function For Identicationkarohal22No ratings yet
- Ocular LSTMDocument25 pagesOcular LSTMthereviewer185No ratings yet
- Research ArticleDocument15 pagesResearch ArticleShanviNo ratings yet
- A Novel Gaussian Discriminant Analysis-Based Computer Aided Diagnosis System For Screening Different Stages of Alzheimers DiseaseDocument6 pagesA Novel Gaussian Discriminant Analysis-Based Computer Aided Diagnosis System For Screening Different Stages of Alzheimers Disease1NT20CS076 KAMSALA THARUNNo ratings yet
- Automatic Severity Classification of Diabetic Retinopathy Based On Densenet and Convolutional Block Attention ModuleDocument10 pagesAutomatic Severity Classification of Diabetic Retinopathy Based On Densenet and Convolutional Block Attention ModuleNitinNo ratings yet
- DR ReportDocument21 pagesDR ReportSahil NegiNo ratings yet
- Diabetic Retinopathy Detection Using MatlabDocument7 pagesDiabetic Retinopathy Detection Using MatlabMani Narayana K TNo ratings yet
- Mask RCNN in MelenomaDocument12 pagesMask RCNN in MelenomaVainavi SamantNo ratings yet
- Machine Learning For Comprehensive Forecasting of Alzheimer's Disease ProgressionDocument14 pagesMachine Learning For Comprehensive Forecasting of Alzheimer's Disease Progressionth8yvv4gpmNo ratings yet
- Age-Related Macular Degeneration: Current Treatment ConceptsFrom EverandAge-Related Macular Degeneration: Current Treatment ConceptsW.E. AlbertiNo ratings yet
- Empowerment Module 1Document7 pagesEmpowerment Module 1Rostum Raton100% (1)
- Defect Detection in PCB Using Image ProcessingDocument7 pagesDefect Detection in PCB Using Image ProcessingMathiprakasamNo ratings yet
- Getinge BCP Workshop - Preparation - Antalya - 25 - 26oct - 2022Document10 pagesGetinge BCP Workshop - Preparation - Antalya - 25 - 26oct - 2022cenkutNo ratings yet
- f1 NC CNC DNCDocument57 pagesf1 NC CNC DNCarunNo ratings yet
- Identified Social ProblemDocument10 pagesIdentified Social Problema kNo ratings yet
- Lab Instructions: HTML + CSS: Tags. A Tag Is A String Enclosed Within " ", For Example "Document9 pagesLab Instructions: HTML + CSS: Tags. A Tag Is A String Enclosed Within " ", For Example "Kỳ TrầnNo ratings yet
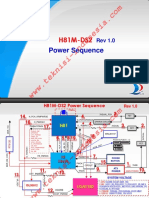
- H81M-DS2: Power SequenceDocument2 pagesH81M-DS2: Power SequenceHilario Serrano Flores100% (3)
- Technology Partner Program GuideDocument7 pagesTechnology Partner Program GuideSerge KuzminNo ratings yet
- Capstone Project Journal-3rd Trimester - Group ID - 191-02 Fall 2019Document17 pagesCapstone Project Journal-3rd Trimester - Group ID - 191-02 Fall 2019Ashley MartinezNo ratings yet
- Log 1Document22 pagesLog 1AkankAfidzNo ratings yet
- Scribd: HistoryDocument2 pagesScribd: HistoryoliviaoliviaoliviaoliviaNo ratings yet
- ps4 Vs Xbox OneDocument4 pagesps4 Vs Xbox OneGurbani SukhNo ratings yet
- Release Notes Generation M: New FeaturesDocument3 pagesRelease Notes Generation M: New FeaturesVictor Uriona BelloNo ratings yet
- lastUIException 63806137181Document7 pageslastUIException 63806137181AgaathaaNo ratings yet
- ADB 45016 001 - Do3NNZcDocument2 pagesADB 45016 001 - Do3NNZcVic MelendezNo ratings yet
- Igcse All Paper 3s MarksDocument134 pagesIgcse All Paper 3s Marksmaya.a.shaker.1No ratings yet
- Maths For MLDocument156 pagesMaths For MLvitomirjNo ratings yet
- Fitbit Charge 3 ManualDocument72 pagesFitbit Charge 3 ManualDawud Quaddur Yusuff BurhanNo ratings yet
- Mod Menu Crash 2023 11 19-09 41 10Document2 pagesMod Menu Crash 2023 11 19-09 41 10РАВАНNo ratings yet
- One Punch Man Chapter 125Document31 pagesOne Punch Man Chapter 125Ryan BarrilNo ratings yet
- Instakit WorkflowDocument10 pagesInstakit WorkflowsawadkarsanjayNo ratings yet
- Data Warehousing and ManagementDocument37 pagesData Warehousing and ManagementMike AntolinoNo ratings yet
- V25 GB PDFDocument143 pagesV25 GB PDFStefan CiobotariuNo ratings yet
- Heart Disease Classification ML Assignment - Jupyter NotebookDocument7 pagesHeart Disease Classification ML Assignment - Jupyter Notebookfurole sammyceNo ratings yet
- Towards Civil Engineering 4.0 (Digital Twins)Document15 pagesTowards Civil Engineering 4.0 (Digital Twins)Daniel Vargas ToroNo ratings yet
- ITB Notes (OU BBA 3rd Sem)Document82 pagesITB Notes (OU BBA 3rd Sem)Saba TaherNo ratings yet
- Scylla HideDocument30 pagesScylla Hidealpaga51No ratings yet
- Hive Properties:-: Hive - Metastore.warehouse - Dir Path You Want To Store Your Table and Database Directory and ItsDocument2 pagesHive Properties:-: Hive - Metastore.warehouse - Dir Path You Want To Store Your Table and Database Directory and ItsSaurabh KothariNo ratings yet