Download as pdf or txt
You might also like
- Shears Cysts of The Oral and Maxillofacial Regions, 5th Edition (Paul Speight)Document382 pagesShears Cysts of The Oral and Maxillofacial Regions, 5th Edition (Paul Speight)Miriam Tovar OgazonNo ratings yet
- Data Interpretation For Medical StudentDocument18 pagesData Interpretation For Medical StudentWee K WeiNo ratings yet
- The Radial Appliance and Wet Cell BatteryDocument160 pagesThe Radial Appliance and Wet Cell Batteryvanderwalt.paul2286No ratings yet
- PLT Indices Normal ValuesDocument6 pagesPLT Indices Normal ValueskireetiNo ratings yet
- Platelet To Lymphocyte Ratio and Neutrophil To Lymphocyte Ratio As Risk Factors For Venous ThrombosisDocument7 pagesPlatelet To Lymphocyte Ratio and Neutrophil To Lymphocyte Ratio As Risk Factors For Venous ThrombosisEvan Nanda AdilistyaNo ratings yet
- Plateletcrit, Mean Platelet Volume, Platelet Distribution Width: Its Expected Values and Correlation With Parallel Red Blood Cell ParametersDocument4 pagesPlateletcrit, Mean Platelet Volume, Platelet Distribution Width: Its Expected Values and Correlation With Parallel Red Blood Cell ParametersSoumik SahaNo ratings yet
- Clinical Features and Outcomes of Thrombotic Thrombocytopenic Purpura With Severe ADAMTS13 Deficiency at Maharat Nakhon Ratchasima HospitalDocument6 pagesClinical Features and Outcomes of Thrombotic Thrombocytopenic Purpura With Severe ADAMTS13 Deficiency at Maharat Nakhon Ratchasima HospitalChalothorn WannaphutNo ratings yet
- An Etiological Reappraisal of Pancytopenia - LargestDocument9 pagesAn Etiological Reappraisal of Pancytopenia - LargestKaye Antonette AntioquiaNo ratings yet
- Pages 4 7Document4 pagesPages 4 7andreas_251650No ratings yet
- Artilce - 1 - Preeclampsia Are Platelet Count and Indices Useful For Its Prognostic - Page 362Document6 pagesArtilce - 1 - Preeclampsia Are Platelet Count and Indices Useful For Its Prognostic - Page 362shilpi sumanNo ratings yet
- Accurasi Perhitungan PlateletDocument68 pagesAccurasi Perhitungan PlateletMaria Yosefina HeraNo ratings yet
- Diferenciacion de Hematogonias y LinfoblastosDocument6 pagesDiferenciacion de Hematogonias y LinfoblastosSusan RamosNo ratings yet
- Matter 2017Document6 pagesMatter 2017AzkiaNo ratings yet
- Ipf Pada ItpDocument5 pagesIpf Pada ItpMunawwar AweNo ratings yet
- Misra 2012Document7 pagesMisra 2012Carlos RiquelmeNo ratings yet
- 5 - Reticulated Platelets - Clinical Application and Future PerspectivesDocument13 pages5 - Reticulated Platelets - Clinical Application and Future PerspectivesnivmastNo ratings yet
- Immature Platelet Fraction Measured On The Sysmex XNeDocument7 pagesImmature Platelet Fraction Measured On The Sysmex XNetuanbu164No ratings yet
- Flow Cytometric Characterization of CerebrospinalDocument12 pagesFlow Cytometric Characterization of CerebrospinalHedo HidayatNo ratings yet
- Platelet IndicesDocument17 pagesPlatelet IndicesNarendra Bhattarai0% (1)
- 02 Platelet To Lymphocyte and Neutrophil To Lymphocyte Ratios Are Useful in Differentiation of Thyroid Conditions With Normal and Increased UptakeDocument6 pages02 Platelet To Lymphocyte and Neutrophil To Lymphocyte Ratios Are Useful in Differentiation of Thyroid Conditions With Normal and Increased UptakeBridia BogarNo ratings yet
- Abuzeid 2019Document7 pagesAbuzeid 2019diegomedicinainternaNo ratings yet
- Roth 2012Document10 pagesRoth 2012ekanovicaNo ratings yet
- To Study The Hematological Profile in Patients With Alcoholic Liver Cirrhosis in A Tertiary Care Hospital in ManipurDocument9 pagesTo Study The Hematological Profile in Patients With Alcoholic Liver Cirrhosis in A Tertiary Care Hospital in ManipurIJAR JOURNALNo ratings yet
- Basophil-Biomarker-Fibrosis - PMF 2018Document8 pagesBasophil-Biomarker-Fibrosis - PMF 2018Banchob SripaNo ratings yet
- Guidelines On Aplastic AnaemiaDocument9 pagesGuidelines On Aplastic AnaemiadskhanNo ratings yet
- Therapeutic Plasma Exchange in Thrombotic Thrombocytopenic PurpuraDocument9 pagesTherapeutic Plasma Exchange in Thrombotic Thrombocytopenic Purpurasugi9namliNo ratings yet
- Study of Correlation Between Imatinib Mesylate Plasma-LinkDocument7 pagesStudy of Correlation Between Imatinib Mesylate Plasma-LinkIvonne Mercedes Gutierrez AtapaucarNo ratings yet
- Nihms 396194Document15 pagesNihms 396194miR 125bNo ratings yet
- HR 11 1 7732Document5 pagesHR 11 1 7732ResidenPatKlin Juli2022No ratings yet
- Yagmur Et Al 2013 Platelet Hyperaggregability Is Highly Prevalent in Patients With Chronic Kidney Disease AnDocument7 pagesYagmur Et Al 2013 Platelet Hyperaggregability Is Highly Prevalent in Patients With Chronic Kidney Disease AnMister FannaniNo ratings yet
- Full Blood Count Apr04, DR Eva RaikDocument7 pagesFull Blood Count Apr04, DR Eva RaikDanielcc LeeNo ratings yet
- Mcdonnell2017 2Document6 pagesMcdonnell2017 2sitiaisyahdNo ratings yet
- JR 2 AnasDocument7 pagesJR 2 AnasCitra DewiNo ratings yet
- Reticulated Platelets - Clinical Application and FDocument13 pagesReticulated Platelets - Clinical Application and Ftufis02No ratings yet
- JCM 08 01175 v2 PDFDocument28 pagesJCM 08 01175 v2 PDFAs'har AnwarNo ratings yet
- Advances in Platelet CountingDocument8 pagesAdvances in Platelet CountingKamran DawoodNo ratings yet
- Bone Marrow Evaluation of Patients Having Pancytopenia at Tertiary Care Center, M. Y. Hospital, Indore, India: One-Year StudyDocument4 pagesBone Marrow Evaluation of Patients Having Pancytopenia at Tertiary Care Center, M. Y. Hospital, Indore, India: One-Year StudyivanNo ratings yet
- Pediatric Non-Hodgkin Lymphoma Workup - Approach Considerations, Laboratory Studies, Imaging StudiesDocument5 pagesPediatric Non-Hodgkin Lymphoma Workup - Approach Considerations, Laboratory Studies, Imaging StudiestopNo ratings yet
- Alm 35 630Document5 pagesAlm 35 630Ryan AndrianNo ratings yet
- Child Turcotte Pugh: Correlation Between Neutrophil To Lymphocyte Ratio With in Liver Cirrhosis PatientsDocument8 pagesChild Turcotte Pugh: Correlation Between Neutrophil To Lymphocyte Ratio With in Liver Cirrhosis PatientsainunnadzNo ratings yet
- Citometria 2005Document8 pagesCitometria 2005Leslie AraujoNo ratings yet
- CBCDocument15 pagesCBCUlicer CruzNo ratings yet
- International Consensus Report On The Investigation and Management of Primary Immune ThrombocytopeniaDocument19 pagesInternational Consensus Report On The Investigation and Management of Primary Immune ThrombocytopeniaJose EspinoNo ratings yet
- Effect of Pneumatic Tubing System Transport On Platelet Apheresis UnitsDocument13 pagesEffect of Pneumatic Tubing System Transport On Platelet Apheresis Unitsrizka widyanaNo ratings yet
- Buttarello-2016-International Journal of Laboratory HematologyDocument10 pagesButtarello-2016-International Journal of Laboratory HematologyLaurentiusJohanNo ratings yet
- Model For End-Stage Liver Disease (MELD) and Allocation of Donor LiversDocument6 pagesModel For End-Stage Liver Disease (MELD) and Allocation of Donor LiversIna MartianaNo ratings yet
- Integrated Analysis of Ultra-Deep ProteomesDocument20 pagesIntegrated Analysis of Ultra-Deep ProteomesMAURICIO FLORESNo ratings yet
- Nej Me 1204395Document2 pagesNej Me 1204395Ferdy SetiawanNo ratings yet
- Immune ThrombocytopeniaDocument19 pagesImmune ThrombocytopeniaAhmad MardiniNo ratings yet
- Cytometry Part B Clinical - 2017 - Dezern - ICCS ESCCA Consensus Guidelines To Detect GPI Deficient Cells in ParoxysmalDocument8 pagesCytometry Part B Clinical - 2017 - Dezern - ICCS ESCCA Consensus Guidelines To Detect GPI Deficient Cells in ParoxysmalzafeersmaNo ratings yet
- Qi 2022Document12 pagesQi 2022Jonathan Billy ChristianNo ratings yet
- Pancytopenia: A Clinico Hematological Study: Gayathri B N, Kadam Satyanarayan RaoDocument6 pagesPancytopenia: A Clinico Hematological Study: Gayathri B N, Kadam Satyanarayan RaoYeni PuspitasariNo ratings yet
- Evaluation of Neutrophiltolymphocyte Ratio NLR and Itscorrelation With Severity of Liver Cirrhosis Based On Childturcott PDFDocument6 pagesEvaluation of Neutrophiltolymphocyte Ratio NLR and Itscorrelation With Severity of Liver Cirrhosis Based On Childturcott PDFSilent StalkerNo ratings yet
- Management and Outcomes For Patients With TTP: Analysis of 100 Cases at A Single InstitutionDocument6 pagesManagement and Outcomes For Patients With TTP: Analysis of 100 Cases at A Single InstitutionBilly Shan LastKagerooboroNo ratings yet
- How To Diagnose AML and MDS by Flow CytometryDocument25 pagesHow To Diagnose AML and MDS by Flow CytometryheinekenredsculptureNo ratings yet
- Pancytopenia A Clinico Hematological StudyDocument6 pagesPancytopenia A Clinico Hematological StudyUci Rahmadhani MNo ratings yet
- Plex 2012Document6 pagesPlex 2012Sundar RamanathanNo ratings yet
- 236 297Document8 pages236 297Andrea KamóNo ratings yet
- Original Article: Study of RBC Histogram in Various AnemiasDocument14 pagesOriginal Article: Study of RBC Histogram in Various AnemiasSirishaNo ratings yet
- Primary and Secondary Thrombocytosis in ChildhoodDocument13 pagesPrimary and Secondary Thrombocytosis in ChildhoodSofia RuanoNo ratings yet
- Diagnosis of Blood and Bone Marrow DisordersFrom EverandDiagnosis of Blood and Bone Marrow DisordersSa A. WangNo ratings yet
- Kara's Poster-1Document1 pageKara's Poster-1Marcellia AngelinaNo ratings yet
- Magnesium CobasDocument5 pagesMagnesium CobasMarcellia AngelinaNo ratings yet
- ImplicationsofHemostasisDisordersinPatientswith CriticalLimbIschemia-AnIn-DepthComparisonof SelectedFactorsDocument9 pagesImplicationsofHemostasisDisordersinPatientswith CriticalLimbIschemia-AnIn-DepthComparisonof SelectedFactorsMarcellia AngelinaNo ratings yet
- 147-Article Text-494-1-10-20211209Document14 pages147-Article Text-494-1-10-20211209Marcellia AngelinaNo ratings yet
- Medicine: Correlation Study Between Serum Neuro-Speci Fic Enolase and Gastric and Colorectal CancersDocument8 pagesMedicine: Correlation Study Between Serum Neuro-Speci Fic Enolase and Gastric and Colorectal CancersMarcellia AngelinaNo ratings yet
- False-Positive Elevations in Carcinoembryonic AntiDocument7 pagesFalse-Positive Elevations in Carcinoembryonic AntiMarcellia AngelinaNo ratings yet
- Ehaa 703Document12 pagesEhaa 703Marcellia AngelinaNo ratings yet
- Yamamoto Et Al 2019 Clinical and Laboratory Predictors For Plaque Erosion in Patients With Acute Coronary SyndromesDocument18 pagesYamamoto Et Al 2019 Clinical and Laboratory Predictors For Plaque Erosion in Patients With Acute Coronary SyndromesMarcellia AngelinaNo ratings yet
- A Comparative Study of Platelet Indices in Acute Coronary SyndromeDocument4 pagesA Comparative Study of Platelet Indices in Acute Coronary SyndromeMarcellia AngelinaNo ratings yet
- Biomarkers of Necrosis and Myocardial Remodeling: August 2015Document25 pagesBiomarkers of Necrosis and Myocardial Remodeling: August 2015Marcellia AngelinaNo ratings yet
- XN Result InterpretationDocument63 pagesXN Result InterpretationMarcellia Angelina100% (1)
- Clases 09 Avian EncephalomyelitisDocument31 pagesClases 09 Avian EncephalomyelitisMijael ChoqueNo ratings yet
- Ijpo 5 3 429 434Document7 pagesIjpo 5 3 429 434Shahid HussainNo ratings yet
- (Derek C. Allen, R. Iain Cameron) Histopathology S (BookFi)Document544 pages(Derek C. Allen, R. Iain Cameron) Histopathology S (BookFi)EduardoArellanoFrancoNo ratings yet
- Klasifikasi Tumor Paru Secara Histologis Menurut WHO Tahun 2015Document3 pagesKlasifikasi Tumor Paru Secara Histologis Menurut WHO Tahun 2015lindaNo ratings yet
- Olson J. R01 HD082554-01A1. The Impact of Early Medical Treatment in Transgender YouthDocument198 pagesOlson J. R01 HD082554-01A1. The Impact of Early Medical Treatment in Transgender YouthMLNo ratings yet
- SyllabusDocument44 pagesSyllabusom vermaNo ratings yet
- 1.radiographic PathologyDocument50 pages1.radiographic PathologyMUHAMMAD SAFWAN SUILENo ratings yet
- FC Path (SA) Chem Blueprints 7-7-2014Document2 pagesFC Path (SA) Chem Blueprints 7-7-2014matentenNo ratings yet
- Literature Study: GRADING OF HOSPITALS - As Per The Number of BedsDocument5 pagesLiterature Study: GRADING OF HOSPITALS - As Per The Number of BedsAmanDhimanNo ratings yet
- Blood Type Test ExperimentDocument8 pagesBlood Type Test ExperimentUpz PhaNo ratings yet
- JobDocument5 pagesJobLalaluluNo ratings yet
- Dokumen - Tips - The Ore ExamDocument17 pagesDokumen - Tips - The Ore ExamHema KamatNo ratings yet
- Textbook Aquaculture Virology 1St Edition Godoy Ebook All Chapter PDFDocument53 pagesTextbook Aquaculture Virology 1St Edition Godoy Ebook All Chapter PDFmaria.talbot893100% (21)
- Silverberg Grading SystemDocument7 pagesSilverberg Grading SystemFlaviu Ionuț FaurNo ratings yet
- 2014 KGSP University Information-English (2020)Document270 pages2014 KGSP University Information-English (2020)hungnv91No ratings yet
- LumnereDocument232 pagesLumnereAlkaNo ratings yet
- BDS PDFDocument16 pagesBDS PDFSimran KathuriaNo ratings yet
- Department of Hematology: Blood C/E (Complete, CBC)Document1 pageDepartment of Hematology: Blood C/E (Complete, CBC)Ilyas FaizNo ratings yet
- Clinical LaboratoriesDocument24 pagesClinical Laboratoriespdamodar200788% (8)
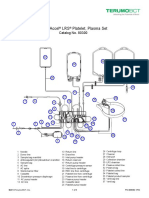
- Trima Accel LRS Platelet, Plasma Set: Catalog No. 80300Document10 pagesTrima Accel LRS Platelet, Plasma Set: Catalog No. 80300Suneo HonekawaNo ratings yet
- MadhavDocument1 pageMadhavmadhav maheshwariNo ratings yet
- Guidelines SuralnervebiopsyDocument7 pagesGuidelines SuralnervebiopsySonam JoshiNo ratings yet
- The Complete Blood Count Is The Calculation of The Cellular (Formed Elements) of BloodDocument26 pagesThe Complete Blood Count Is The Calculation of The Cellular (Formed Elements) of BloodNabard MhammadNo ratings yet
- Book Reviews: Kar5ner'sDocument3 pagesBook Reviews: Kar5ner'sAhmed MawardiNo ratings yet
- Venkatraman K PDFDocument3 pagesVenkatraman K PDFRana Zara AthayaNo ratings yet
- Chen 2011 PDFDocument15 pagesChen 2011 PDFanthony tiensunNo ratings yet
- Anatomy Log BookwbDocument27 pagesAnatomy Log BookwbDr ZubairNo ratings yet
- Lista CzasopismDocument544 pagesLista CzasopismJohn RotfliczekNo ratings yet