
DM Critical-Care-Medicine
DM Critical-Care-Medicine
You might also like
- WHO Scoring of Ayurveda SymptomsDocument116 pagesWHO Scoring of Ayurveda SymptomsNaresh KhanderayNo ratings yet
- AETCOM QuestionairDocument3 pagesAETCOM Questionairlatest techs&tips100% (1)
- IMM Surgery (2019)Document47 pagesIMM Surgery (2019)Umar Farooque100% (2)
- DM - Cardiac-AnaesthesiaDocument19 pagesDM - Cardiac-AnaesthesiaKajori ChakrabortyNo ratings yet
- Statutes DPTDocument27 pagesStatutes DPTzeeshanNo ratings yet
- CLUSTERS LIST - (CHNCS) GO-209Document45 pagesCLUSTERS LIST - (CHNCS) GO-209Gadde Srinivasarao67% (3)
- Thyroid NodulesDocument34 pagesThyroid NodulesEphobiaNo ratings yet
- Presc Audit ReportDocument85 pagesPresc Audit ReportAnuj KaushalNo ratings yet
- PiOS Sample (CH 2)Document39 pagesPiOS Sample (CH 2)Ramyasree BadeNo ratings yet
- 5Document232 pages5Raghunath Ravirala100% (2)
- Research ObjectivesDocument57 pagesResearch ObjectivesCathay Gallego MachanNo ratings yet
- Venous Leg UlcersDocument28 pagesVenous Leg UlcersamurachNo ratings yet
- DRNB Neuro Anaesthesia Paper3Document4 pagesDRNB Neuro Anaesthesia Paper3lakshminivas Pingali100% (1)
- 2022 Accreditation Standards For Medical InstitutesDocument93 pages2022 Accreditation Standards For Medical InstitutesAhsan MalikNo ratings yet
- Descriptive Study DesignsDocument6 pagesDescriptive Study DesignsstNo ratings yet
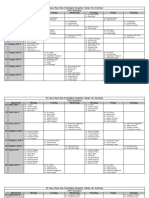
- Sri Guru Ram Das Charitable Hospital, Vallah, Sri Amritsar OPD ScheduleDocument3 pagesSri Guru Ram Das Charitable Hospital, Vallah, Sri Amritsar OPD ScheduleTarlochan SinghNo ratings yet
- DRNB CRITICAL CARE MEDICINE Paper3Document4 pagesDRNB CRITICAL CARE MEDICINE Paper3aparnapingali0100% (1)
- Clinical Medical Pathways in PakistanDocument2 pagesClinical Medical Pathways in PakistanMuhammad TalhahNo ratings yet
- Measuring Pulse OximeterDocument94 pagesMeasuring Pulse OximeterMuhammed HammadNo ratings yet
- Appendix 10 - Warfarin Counselling ChecklistDocument3 pagesAppendix 10 - Warfarin Counselling ChecklistMuhammad TahirNo ratings yet
- ETT SUCTION DEWASA ACI14 - Suction - 2-2 PDFDocument46 pagesETT SUCTION DEWASA ACI14 - Suction - 2-2 PDFAde Rahmah YuliaNo ratings yet
- EU IM Curriculum 2016Document72 pagesEU IM Curriculum 2016Ana Raquel Realista Coelho Dos Santos PedrosaNo ratings yet
- To Study Perinatal Outcome in Thyroid Disorder in PregnancyDocument34 pagesTo Study Perinatal Outcome in Thyroid Disorder in PregnancyAnkit AgarwalNo ratings yet
- Anticancer Effects of Chinese Herbal Medicine, Science or Myth?Document9 pagesAnticancer Effects of Chinese Herbal Medicine, Science or Myth?marcussiNo ratings yet
- Karnofsky/Lansky Performance StatusDocument0 pagesKarnofsky/Lansky Performance StatusHanayuki VizureiNo ratings yet
- Roles and Responsibilities in Clinical Trail PDFDocument3 pagesRoles and Responsibilities in Clinical Trail PDFyasahswi91No ratings yet
- DNB Emergency Medicine Paper4Document5 pagesDNB Emergency Medicine Paper4Vaishnavi Agrawal100% (1)
- Airway ACLSDocument29 pagesAirway ACLSJoshua KosowskyNo ratings yet
- EthicsDocument65 pagesEthicsUmesh KawalkarNo ratings yet
- Scoping and Rapid ReviewsDocument19 pagesScoping and Rapid ReviewsTam TNo ratings yet
- Proceedings of The Director of Public Health and Preventive MEDICINE, CHENNAI - 600 006. Present: Dr.K.Kolandaswamy, MBBS, Mae, DPH, Dih, Dbe.Document8 pagesProceedings of The Director of Public Health and Preventive MEDICINE, CHENNAI - 600 006. Present: Dr.K.Kolandaswamy, MBBS, Mae, DPH, Dih, Dbe.Dr.Bruno RajuNo ratings yet
- Case MalariaDocument2 pagesCase MalariaRaju NiraulaNo ratings yet
- DNB Emergency Medicine Paper1Document4 pagesDNB Emergency Medicine Paper1Vaishnavi Agrawal100% (1)
- MD Emergency MedicineDocument34 pagesMD Emergency MedicineSaurav KumarNo ratings yet
- Prospectus - 2022 Admission: M. Phil Course in Clinical Epidemiology (Part-Time) CourseDocument5 pagesProspectus - 2022 Admission: M. Phil Course in Clinical Epidemiology (Part-Time) CourseDr.Minu C MathewsNo ratings yet
- Guidlines July 2017Document14 pagesGuidlines July 2017Ghulam JillaniNo ratings yet
- MD (H) Prospectus - 2019-20 - 17 - 09Document20 pagesMD (H) Prospectus - 2019-20 - 17 - 09brunda maneepuriNo ratings yet
- Final PH D Ordinance 2019Document19 pagesFinal PH D Ordinance 2019BKNo ratings yet
- SR Manual 2013 14Document315 pagesSR Manual 2013 14Zebram ZeeNo ratings yet
- Mscnregulations 2010 Ver 2Document187 pagesMscnregulations 2010 Ver 2John SamuelNo ratings yet
- Brochure PGSSET 2014 RguhsDocument13 pagesBrochure PGSSET 2014 RguhsRaja TalwarNo ratings yet
- Master of PhysiotherapyDocument98 pagesMaster of Physiotherapyakhilesh jhariyaNo ratings yet
- MD DermatologyDocument65 pagesMD DermatologyamanabduwahabNo ratings yet
- OASIS-E Guidance Manual - 5.16.22Document46 pagesOASIS-E Guidance Manual - 5.16.22mosaNo ratings yet
- M.ch. UrologyDocument81 pagesM.ch. UrologyajaypeoplesenseNo ratings yet
- Naturopathy Revised2014-15 01102015 PDFDocument103 pagesNaturopathy Revised2014-15 01102015 PDFRajesh KumarNo ratings yet
- MPH Brochure 2023Document8 pagesMPH Brochure 2023Shraddha PatadiyaNo ratings yet
- MPT Syllabus-1 PDFDocument53 pagesMPT Syllabus-1 PDFYadav NishaNo ratings yet
- Information Bulletin For National Eligibility Cum Entrance Test (Post Graduate)Document88 pagesInformation Bulletin For National Eligibility Cum Entrance Test (Post Graduate)Rajat789No ratings yet
- NEET PG 2013 Information Booklet FINALDocument88 pagesNEET PG 2013 Information Booklet FINALManish Chandra PrabhakarNo ratings yet
- Post Basic Nursing SyllabusDocument112 pagesPost Basic Nursing SyllabusSathish Kumar67% (3)
- Notification & IMM SGR (2019)Document49 pagesNotification & IMM SGR (2019)QandeelNo ratings yet
- The Tamil Nadu Dr. M.G.R. Medical UniversityDocument7 pagesThe Tamil Nadu Dr. M.G.R. Medical UniversityDrgopal VenkatNo ratings yet
- Syllabus MPT 1 YrDocument38 pagesSyllabus MPT 1 YrShubham ChopadeNo ratings yet
- Final PGMER DraftDocument36 pagesFinal PGMER Draftprashant singhNo ratings yet
- BSC N Regulations 2010 Ver 2Document183 pagesBSC N Regulations 2010 Ver 2Susan HepziNo ratings yet
- Bachelor of PhysiotherapyDocument79 pagesBachelor of Physiotherapyguptaalok998877No ratings yet
- Teachers Eligibility QualificationsDocument23 pagesTeachers Eligibility QualificationsdrpklalNo ratings yet
- Postgraduate Medical Education Regulations 2021Document23 pagesPostgraduate Medical Education Regulations 2021Dhwani DesaiNo ratings yet
- Oct 2022 PH.D Broucher & Area of ResearchDocument7 pagesOct 2022 PH.D Broucher & Area of ResearchbiopharmacyNo ratings yet

























































Download as pdf or txt
You might also like
- WHO Scoring of Ayurveda SymptomsDocument116 pagesWHO Scoring of Ayurveda SymptomsNaresh KhanderayNo ratings yet
- AETCOM QuestionairDocument3 pagesAETCOM Questionairlatest techs&tips100% (1)
- IMM Surgery (2019)Document47 pagesIMM Surgery (2019)Umar Farooque100% (2)
- DM - Cardiac-AnaesthesiaDocument19 pagesDM - Cardiac-AnaesthesiaKajori ChakrabortyNo ratings yet
- Statutes DPTDocument27 pagesStatutes DPTzeeshanNo ratings yet
- CLUSTERS LIST - (CHNCS) GO-209Document45 pagesCLUSTERS LIST - (CHNCS) GO-209Gadde Srinivasarao67% (3)
- Thyroid NodulesDocument34 pagesThyroid NodulesEphobiaNo ratings yet
- Presc Audit ReportDocument85 pagesPresc Audit ReportAnuj KaushalNo ratings yet
- PiOS Sample (CH 2)Document39 pagesPiOS Sample (CH 2)Ramyasree BadeNo ratings yet
- 5Document232 pages5Raghunath Ravirala100% (2)
- Research ObjectivesDocument57 pagesResearch ObjectivesCathay Gallego MachanNo ratings yet
- Venous Leg UlcersDocument28 pagesVenous Leg UlcersamurachNo ratings yet
- DRNB Neuro Anaesthesia Paper3Document4 pagesDRNB Neuro Anaesthesia Paper3lakshminivas Pingali100% (1)
- 2022 Accreditation Standards For Medical InstitutesDocument93 pages2022 Accreditation Standards For Medical InstitutesAhsan MalikNo ratings yet
- Descriptive Study DesignsDocument6 pagesDescriptive Study DesignsstNo ratings yet
- Sri Guru Ram Das Charitable Hospital, Vallah, Sri Amritsar OPD ScheduleDocument3 pagesSri Guru Ram Das Charitable Hospital, Vallah, Sri Amritsar OPD ScheduleTarlochan SinghNo ratings yet
- DRNB CRITICAL CARE MEDICINE Paper3Document4 pagesDRNB CRITICAL CARE MEDICINE Paper3aparnapingali0100% (1)
- Clinical Medical Pathways in PakistanDocument2 pagesClinical Medical Pathways in PakistanMuhammad TalhahNo ratings yet
- Measuring Pulse OximeterDocument94 pagesMeasuring Pulse OximeterMuhammed HammadNo ratings yet
- Appendix 10 - Warfarin Counselling ChecklistDocument3 pagesAppendix 10 - Warfarin Counselling ChecklistMuhammad TahirNo ratings yet
- ETT SUCTION DEWASA ACI14 - Suction - 2-2 PDFDocument46 pagesETT SUCTION DEWASA ACI14 - Suction - 2-2 PDFAde Rahmah YuliaNo ratings yet
- EU IM Curriculum 2016Document72 pagesEU IM Curriculum 2016Ana Raquel Realista Coelho Dos Santos PedrosaNo ratings yet
- To Study Perinatal Outcome in Thyroid Disorder in PregnancyDocument34 pagesTo Study Perinatal Outcome in Thyroid Disorder in PregnancyAnkit AgarwalNo ratings yet
- Anticancer Effects of Chinese Herbal Medicine, Science or Myth?Document9 pagesAnticancer Effects of Chinese Herbal Medicine, Science or Myth?marcussiNo ratings yet
- Karnofsky/Lansky Performance StatusDocument0 pagesKarnofsky/Lansky Performance StatusHanayuki VizureiNo ratings yet
- Roles and Responsibilities in Clinical Trail PDFDocument3 pagesRoles and Responsibilities in Clinical Trail PDFyasahswi91No ratings yet
- DNB Emergency Medicine Paper4Document5 pagesDNB Emergency Medicine Paper4Vaishnavi Agrawal100% (1)
- Airway ACLSDocument29 pagesAirway ACLSJoshua KosowskyNo ratings yet
- EthicsDocument65 pagesEthicsUmesh KawalkarNo ratings yet
- Scoping and Rapid ReviewsDocument19 pagesScoping and Rapid ReviewsTam TNo ratings yet
- Proceedings of The Director of Public Health and Preventive MEDICINE, CHENNAI - 600 006. Present: Dr.K.Kolandaswamy, MBBS, Mae, DPH, Dih, Dbe.Document8 pagesProceedings of The Director of Public Health and Preventive MEDICINE, CHENNAI - 600 006. Present: Dr.K.Kolandaswamy, MBBS, Mae, DPH, Dih, Dbe.Dr.Bruno RajuNo ratings yet
- Case MalariaDocument2 pagesCase MalariaRaju NiraulaNo ratings yet
- DNB Emergency Medicine Paper1Document4 pagesDNB Emergency Medicine Paper1Vaishnavi Agrawal100% (1)
- MD Emergency MedicineDocument34 pagesMD Emergency MedicineSaurav KumarNo ratings yet
- Prospectus - 2022 Admission: M. Phil Course in Clinical Epidemiology (Part-Time) CourseDocument5 pagesProspectus - 2022 Admission: M. Phil Course in Clinical Epidemiology (Part-Time) CourseDr.Minu C MathewsNo ratings yet
- Guidlines July 2017Document14 pagesGuidlines July 2017Ghulam JillaniNo ratings yet
- MD (H) Prospectus - 2019-20 - 17 - 09Document20 pagesMD (H) Prospectus - 2019-20 - 17 - 09brunda maneepuriNo ratings yet
- Final PH D Ordinance 2019Document19 pagesFinal PH D Ordinance 2019BKNo ratings yet
- SR Manual 2013 14Document315 pagesSR Manual 2013 14Zebram ZeeNo ratings yet
- Mscnregulations 2010 Ver 2Document187 pagesMscnregulations 2010 Ver 2John SamuelNo ratings yet
- Brochure PGSSET 2014 RguhsDocument13 pagesBrochure PGSSET 2014 RguhsRaja TalwarNo ratings yet
- Master of PhysiotherapyDocument98 pagesMaster of Physiotherapyakhilesh jhariyaNo ratings yet
- MD DermatologyDocument65 pagesMD DermatologyamanabduwahabNo ratings yet
- OASIS-E Guidance Manual - 5.16.22Document46 pagesOASIS-E Guidance Manual - 5.16.22mosaNo ratings yet
- M.ch. UrologyDocument81 pagesM.ch. UrologyajaypeoplesenseNo ratings yet
- Naturopathy Revised2014-15 01102015 PDFDocument103 pagesNaturopathy Revised2014-15 01102015 PDFRajesh KumarNo ratings yet
- MPH Brochure 2023Document8 pagesMPH Brochure 2023Shraddha PatadiyaNo ratings yet
- MPT Syllabus-1 PDFDocument53 pagesMPT Syllabus-1 PDFYadav NishaNo ratings yet
- Information Bulletin For National Eligibility Cum Entrance Test (Post Graduate)Document88 pagesInformation Bulletin For National Eligibility Cum Entrance Test (Post Graduate)Rajat789No ratings yet
- NEET PG 2013 Information Booklet FINALDocument88 pagesNEET PG 2013 Information Booklet FINALManish Chandra PrabhakarNo ratings yet
- Post Basic Nursing SyllabusDocument112 pagesPost Basic Nursing SyllabusSathish Kumar67% (3)
- Notification & IMM SGR (2019)Document49 pagesNotification & IMM SGR (2019)QandeelNo ratings yet
- The Tamil Nadu Dr. M.G.R. Medical UniversityDocument7 pagesThe Tamil Nadu Dr. M.G.R. Medical UniversityDrgopal VenkatNo ratings yet
- Syllabus MPT 1 YrDocument38 pagesSyllabus MPT 1 YrShubham ChopadeNo ratings yet
- Final PGMER DraftDocument36 pagesFinal PGMER Draftprashant singhNo ratings yet
- BSC N Regulations 2010 Ver 2Document183 pagesBSC N Regulations 2010 Ver 2Susan HepziNo ratings yet
- Bachelor of PhysiotherapyDocument79 pagesBachelor of Physiotherapyguptaalok998877No ratings yet
- Teachers Eligibility QualificationsDocument23 pagesTeachers Eligibility QualificationsdrpklalNo ratings yet
- Postgraduate Medical Education Regulations 2021Document23 pagesPostgraduate Medical Education Regulations 2021Dhwani DesaiNo ratings yet
- Oct 2022 PH.D Broucher & Area of ResearchDocument7 pagesOct 2022 PH.D Broucher & Area of ResearchbiopharmacyNo ratings yet