Download as pdf or txt
You might also like
- Oculofacial Plastic and Reconstructive SurgeryDocument562 pagesOculofacial Plastic and Reconstructive SurgeryGimena Dapena100% (5)
- Gender-Responsive Lgu (Gerl) Assessment ToolDocument42 pagesGender-Responsive Lgu (Gerl) Assessment ToolDyanne Kristine Almirante Sideño100% (8)
- The Bidirectional Movement of The Frontalis Muscle: Introducing The Line of Convergence and Its Potential Clinical RelevanceDocument8 pagesThe Bidirectional Movement of The Frontalis Muscle: Introducing The Line of Convergence and Its Potential Clinical RelevanceBruna RochaNo ratings yet
- Gliding Brow LiftDocument11 pagesGliding Brow LiftThiago BuenoNo ratings yet
- Project Feasibility Study KolDocument86 pagesProject Feasibility Study KolPrasenjit Biswas100% (2)
- Herva Karwur Jurbal Tahun 2021 - CompressedDocument10 pagesHerva Karwur Jurbal Tahun 2021 - CompressedDavid LewanNo ratings yet
- Asian Upper BlepharoplastyDocument11 pagesAsian Upper BlepharoplastyJake ParkNo ratings yet
- (Paper) - Eyelid Surgical AnatomyDocument19 pages(Paper) - Eyelid Surgical AnatomycommandityNo ratings yet
- Articol 2 PDFDocument13 pagesArticol 2 PDFIoanna Bianca HNo ratings yet
- Simultaneous Double Eyelid Blepharoplasty and Ptosis Correction With A Single-Knot, Continuous, Nonincisional Technique: A Five-Year ReviewDocument7 pagesSimultaneous Double Eyelid Blepharoplasty and Ptosis Correction With A Single-Knot, Continuous, Nonincisional Technique: A Five-Year ReviewTruong NguyenNo ratings yet
- Endoscopic Forehead and Brow Lift: Gregory S. Keller, M.D., F.A.C.S., and Grigoriy Mashkevich, M.DDocument12 pagesEndoscopic Forehead and Brow Lift: Gregory S. Keller, M.D., F.A.C.S., and Grigoriy Mashkevich, M.DVivekanand ChandrashekarNo ratings yet
- Asian Upper Eyelied Ptosis Correction The Levator Musculoaponeurotic Juntion FormulaDocument10 pagesAsian Upper Eyelied Ptosis Correction The Levator Musculoaponeurotic Juntion FormulaRaul FonsecaNo ratings yet
- A Novel Strategy To Achieve Stable and Lasting Double Eyelids in Upper BlepharoplastyDocument4 pagesA Novel Strategy To Achieve Stable and Lasting Double Eyelids in Upper BlepharoplastyRaul FonsecaNo ratings yet
- Advanced Endo Facial RejuDocument10 pagesAdvanced Endo Facial Rejudrkorn.ophNo ratings yet
- Blefaroplastia en AsiaticosDocument11 pagesBlefaroplastia en AsiaticosLiliana Cepeda GarcíaNo ratings yet
- Blepharoplasty: Indications and Surgical TechniquesDocument10 pagesBlepharoplasty: Indications and Surgical TechniquesIJAR JOURNALNo ratings yet
- The Effect of "Single" Vs "Double" Eyelids On The Perceived Attractiveness of Chinese WomenDocument9 pagesThe Effect of "Single" Vs "Double" Eyelids On The Perceived Attractiveness of Chinese WomenNICOLETA DEACONESCUNo ratings yet
- Revisional Asian Blepharoplasty of The High Eyelid Fold - Tarsus-Orbicularis Fixation Combined With Orbital Fat Repositioning TechniqueDocument5 pagesRevisional Asian Blepharoplasty of The High Eyelid Fold - Tarsus-Orbicularis Fixation Combined With Orbital Fat Repositioning TechniqueRaul FonsecaNo ratings yet
- Simultaneous Double Eyelid Blepharoplasty and Ptosis CorrectionDocument8 pagesSimultaneous Double Eyelid Blepharoplasty and Ptosis CorrectionshininghmNo ratings yet
- Asian Blepharoplasty PDFDocument9 pagesAsian Blepharoplasty PDFariskaNo ratings yet
- Nose Tip Elongation and Elevation: A Novel Filler Injection TechniqueDocument17 pagesNose Tip Elongation and Elevation: A Novel Filler Injection TechniqueJuan AvonNo ratings yet
- Sjac 126Document18 pagesSjac 126dukedevils27No ratings yet
- Frontalis + OOM FlapDocument7 pagesFrontalis + OOM Flapdrkorn.ophNo ratings yet
- Asianmaleblepharoplasty Andrhinoplasty: John W. Frederick,, Jae Kim,, Donald B. YooDocument13 pagesAsianmaleblepharoplasty Andrhinoplasty: John W. Frederick,, Jae Kim,, Donald B. YooCarlos Hernan Castañeda RuizNo ratings yet
- CANTOPLASTIADocument11 pagesCANTOPLASTIAvarelarmNo ratings yet
- 10 1111@jocd 13491Document28 pages10 1111@jocd 13491Emrys1987No ratings yet
- An Algorithm For Thepreoperative DiagnosisDocument16 pagesAn Algorithm For Thepreoperative DiagnosismedellincolombiaNo ratings yet
- Capítulo 8Document11 pagesCapítulo 8Erik BrooksNo ratings yet
- Blefaroplastia Superior Associada A Remoção de Pele Abaixo Do Supercílio em Pacientes de Origem AsiaticaDocument4 pagesBlefaroplastia Superior Associada A Remoção de Pele Abaixo Do Supercílio em Pacientes de Origem AsiaticaIvoNo ratings yet
- Upper Eyelid Blepharoplasty Improved The Overall Periorbital Aesthetics Ratio by Enhancing Harmony Between The Eyes and EyebrowsDocument10 pagesUpper Eyelid Blepharoplasty Improved The Overall Periorbital Aesthetics Ratio by Enhancing Harmony Between The Eyes and Eyebrowstephy1394No ratings yet
- The Five-Step Lower Blepharoplasty: Blending The Eyelid-Cheek JunctionDocument9 pagesThe Five-Step Lower Blepharoplasty: Blending The Eyelid-Cheek JunctionFelyana GunawanNo ratings yet
- J of Cosmetic Dermatology - 2021 - Chuang - Cephalometric Analysis Following Combined Sub SMAS Hyaluronic Acid InjectionDocument8 pagesJ of Cosmetic Dermatology - 2021 - Chuang - Cephalometric Analysis Following Combined Sub SMAS Hyaluronic Acid Injectionjoann15marrieNo ratings yet
- Wang 2019Document10 pagesWang 2019Hải Dương MinhNo ratings yet
- DoubleEyelids by William P Chen MDDocument36 pagesDoubleEyelids by William P Chen MDAnonymous 8hVpaQdCtrNo ratings yet
- Quantification of The Aesthetically Desirable Female Midface Position.Document10 pagesQuantification of The Aesthetically Desirable Female Midface Position.Tseng WadeNo ratings yet
- Massry - Management of Postblepharoplasty Lower Eyelid RetractionDocument10 pagesMassry - Management of Postblepharoplasty Lower Eyelid RetractionLuiggi Fayad100% (1)
- DR Lakshmi Saleem 7thPSAAP Conference - Cosmetic Surgery Clinic HyderabadDocument32 pagesDR Lakshmi Saleem 7thPSAAP Conference - Cosmetic Surgery Clinic Hyderabadcosmeticsurgeryclinic_in9534No ratings yet
- Aesthetic 20 Surgery 20 Journal 20201120 Jacono 20 ParikhDocument18 pagesAesthetic 20 Surgery 20 Journal 20201120 Jacono 20 ParikhPaulo VianaNo ratings yet
- Blepharoplasty An Overview 2Document6 pagesBlepharoplasty An Overview 2Sandro GouveiaNo ratings yet
- Cheek FlapDocument4 pagesCheek FlapDae AhmadNo ratings yet
- Academy ExpressDocument5 pagesAcademy ExpressbalakunjeNo ratings yet
- Vectorial Facial Sculpting 2020Document21 pagesVectorial Facial Sculpting 2020maat1No ratings yet
- Sjaa066 (01 03)Document3 pagesSjaa066 (01 03)mariaana300552No ratings yet
- Scalp Reconstruction An Algorithmic Approach and Systematic ReviewDocument11 pagesScalp Reconstruction An Algorithmic Approach and Systematic Reviewahmed atefNo ratings yet
- 1 s2.0 S2173579422000755 MainDocument11 pages1 s2.0 S2173579422000755 MainAndrea ChanNo ratings yet
- 2022+vitaly+ +Skin+Contour+Sutures+in+RhinoplastyDocument11 pages2022+vitaly+ +Skin+Contour+Sutures+in+RhinoplastyJackeline Lizbeth Anicama mendozaNo ratings yet
- Niechajev 2020Document9 pagesNiechajev 2020Schwan AbdulkareemNo ratings yet
- Subbrow Blepharoplasty For Upper Eyelid Rejuvenation in AsiansDocument5 pagesSubbrow Blepharoplasty For Upper Eyelid Rejuvenation in AsiansdoctorbanNo ratings yet
- Editorial: The Management of Retinal Detachment: Techniques and PerspectivesDocument3 pagesEditorial: The Management of Retinal Detachment: Techniques and PerspectivesSarahNo ratings yet
- Anatomical Map of The Facial Artery For Facial 2019Document12 pagesAnatomical Map of The Facial Artery For Facial 2019letty3gapeNo ratings yet
- Transpalpebral Eyebrow Lift: The Mini Eyebrow Lift: Plastic and Aesthetic ResearchDocument9 pagesTranspalpebral Eyebrow Lift: The Mini Eyebrow Lift: Plastic and Aesthetic ResearchMaxi AbalosNo ratings yet
- Algorithm For The Management of Ectropion Through Medial and Lateral CanthopexyDocument9 pagesAlgorithm For The Management of Ectropion Through Medial and Lateral CanthopexyRania ENo ratings yet
- Research Assignment IsmDocument4 pagesResearch Assignment Ismapi-426395895No ratings yet
- 2019 Three Simple Steps For Refining Transcutaneous Lower Blepharoplasty For Aging EyelidsDocument15 pages2019 Three Simple Steps For Refining Transcutaneous Lower Blepharoplasty For Aging EyelidsDimitris RodriguezNo ratings yet
- 266 2023 Article 3444Document7 pages266 2023 Article 3444Ingook SongNo ratings yet
- OphthalmologyConference 2017 TPDocument9 pagesOphthalmologyConference 2017 TPsarika jamesNo ratings yet
- Sjab 116Document8 pagesSjab 116Poramate PITAK-ARNNOPNo ratings yet
- Aesthetic Surgery of The Orbits and EyelidsDocument31 pagesAesthetic Surgery of The Orbits and EyelidsdoctorbanNo ratings yet
- The Open Brow LiftDocument8 pagesThe Open Brow LiftdoctorbanNo ratings yet
- Jurnal MataDocument7 pagesJurnal MatafaniaapriskaNo ratings yet
- A Modified Procedure For Blepharoplasty - Physiological Structure Reconstruction of Upper EyelidsDocument4 pagesA Modified Procedure For Blepharoplasty - Physiological Structure Reconstruction of Upper EyelidsRaul FonsecaNo ratings yet
- Evolution in Techniques For Endsocopic Brow Lift With Deep Temporal Fixation Only and Lower Blepharoplasty-Transconjunctival Fat RepositioningDocument16 pagesEvolution in Techniques For Endsocopic Brow Lift With Deep Temporal Fixation Only and Lower Blepharoplasty-Transconjunctival Fat RepositioningBFF BotoxNo ratings yet
- Filler Complications: Filler-Induced Hypersensitivity Reactions, Granuloma, Necrosis, and BlindnessFrom EverandFiller Complications: Filler-Induced Hypersensitivity Reactions, Granuloma, Necrosis, and BlindnessNo ratings yet
- Pre Int 3 Listeningscripts 7Document10 pagesPre Int 3 Listeningscripts 7Burak SelçukNo ratings yet
- Module 2 Community Organizing - 2140354780 PDFDocument10 pagesModule 2 Community Organizing - 2140354780 PDFAlyssa marieNo ratings yet
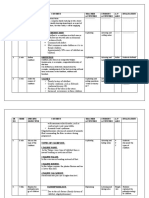
- SR NO Time Specific Objective Content Teacher Activities Student Activities A.V Aids EvaluationDocument16 pagesSR NO Time Specific Objective Content Teacher Activities Student Activities A.V Aids EvaluationJuhi Johnson JadhavNo ratings yet
- Nursing Exam Questions 2023 Part 2Document5 pagesNursing Exam Questions 2023 Part 2Lejo SunnyNo ratings yet
- Trends in Recreation and LeisureDocument30 pagesTrends in Recreation and LeisureShindelle De KeyserNo ratings yet
- Stress Management Quiz: True FalseDocument2 pagesStress Management Quiz: True FalseLady Ann HondoNo ratings yet
- NURS-FPX4030 - MuaClaude - Assessment 2 - 1Document6 pagesNURS-FPX4030 - MuaClaude - Assessment 2 - 1marvinNo ratings yet
- Health.&.Nutrition May.2017 P2PDocument116 pagesHealth.&.Nutrition May.2017 P2PAbel BejanNo ratings yet
- 2017 - PSYC1100 - Chapter 2 - Research MethodsDocument16 pages2017 - PSYC1100 - Chapter 2 - Research MethodsKevin HuangNo ratings yet
- Body Fat Percentage PDFDocument23 pagesBody Fat Percentage PDFmcvelli40No ratings yet
- Health Insurance Premium CalculatorDocument15 pagesHealth Insurance Premium CalculatorqwertyNo ratings yet
- 10 Animal Welfare Overview JIT PPT FINALDocument19 pages10 Animal Welfare Overview JIT PPT FINALYOUSAFNo ratings yet
- Microbiology (HBM 531)Document5 pagesMicrobiology (HBM 531)panther795No ratings yet
- Unit 5.1 Student JLBDocument26 pagesUnit 5.1 Student JLBkendrabooboooNo ratings yet
- Spanish For Medical ProfessionalsDocument372 pagesSpanish For Medical ProfessionalsJean MallipudiNo ratings yet
- 2019年6月英语四级考试真题试卷 (完整版 第1套)Document12 pages2019年6月英语四级考试真题试卷 (完整版 第1套)jiaxuNo ratings yet
- BioPIN Sternheimer-Malbin-Concentrate - Bioanalytic (En)Document2 pagesBioPIN Sternheimer-Malbin-Concentrate - Bioanalytic (En)Yan PetrovNo ratings yet
- Hans India Hyderabad - 25-04-20 PDFDocument10 pagesHans India Hyderabad - 25-04-20 PDFShubham NathNo ratings yet
- A Study of Snail Behavior: Directions For StudentsDocument28 pagesA Study of Snail Behavior: Directions For StudentsHyacinth Jade SantosNo ratings yet
- TR - Driving NC IiDocument61 pagesTR - Driving NC IiMark Kevin DaitolNo ratings yet
- HS-Series Instruction Manual 4HS / 6HS: Reciprocating CompressorDocument151 pagesHS-Series Instruction Manual 4HS / 6HS: Reciprocating CompressornavNo ratings yet
- 18 Affidavit of Experience (Form A)Document2 pages18 Affidavit of Experience (Form A)playbowensNo ratings yet
- Lesson Plan in Tle SubjectDocument11 pagesLesson Plan in Tle SubjectJonaiza PangandianNo ratings yet
- Nurses' Understanding of Patient-Centred Care in Bhutan: Rinchen Pelzang, Beverley Wood, Simon BlackDocument8 pagesNurses' Understanding of Patient-Centred Care in Bhutan: Rinchen Pelzang, Beverley Wood, Simon BlackKinley DorjiNo ratings yet
- Braouonline MSC Psychology Assignments Psychology I Year 2019-20Document8 pagesBraouonline MSC Psychology Assignments Psychology I Year 2019-20Telika RamuNo ratings yet
- GNHCPDocument210 pagesGNHCPSuryavenkat RaghavanNo ratings yet
- Stolen Generations PDFDocument4 pagesStolen Generations PDFIndiana JonesNo ratings yet