
Statistics
Statistics
You might also like
- Sparks Taylors Nursing Diagnosis Pocket Guide 3rd Edition Ebook PDFDocument61 pagesSparks Taylors Nursing Diagnosis Pocket Guide 3rd Edition Ebook PDFzelma.bennett128100% (48)
- Review of A Little Book For New TheologiansDocument3 pagesReview of A Little Book For New Theologianscreative2009No ratings yet
- Bodart Et Al. - 2000 - Identifying Information Needs and IndicatorsDocument24 pagesBodart Et Al. - 2000 - Identifying Information Needs and IndicatorsEvan Baros IrawanNo ratings yet
- Learning Guide #55: Nursing Level IiiDocument8 pagesLearning Guide #55: Nursing Level IiiSamuel MergaNo ratings yet
- Analyze & Interprete Pro - Data-EditedDocument32 pagesAnalyze & Interprete Pro - Data-EditedFelekePhiliphosNo ratings yet
- Group 5 (FE64) - Descriptive StatisticsDocument10 pagesGroup 5 (FE64) - Descriptive StatisticsVũ GiangNo ratings yet
- Data Analysis and Use Training GuidelinesDocument23 pagesData Analysis and Use Training GuidelinesFadhil ChiwangaNo ratings yet
- Biostat Chapter 1-7Document85 pagesBiostat Chapter 1-7Kassa GebreyesusNo ratings yet
- Anjali f9Document29 pagesAnjali f9NEERNo ratings yet
- Analyze and Interpret Production DataDocument16 pagesAnalyze and Interpret Production DataFelekePhiliphosNo ratings yet
- Health Data FirstDocument30 pagesHealth Data FirstSamuel MergaNo ratings yet
- Week 1011 Guidelines Protocols Tools in Documentation Related To Client CareDocument59 pagesWeek 1011 Guidelines Protocols Tools in Documentation Related To Client CareobnimagashelinaNo ratings yet
- Tugas Sistem Informasi KesehatanDocument37 pagesTugas Sistem Informasi Kesehatandewi shintaNo ratings yet
- Executive Briefer ILCDocument2 pagesExecutive Briefer ILCjohnllenalcantaraNo ratings yet
- Comp. StatsDocument9 pagesComp. Statsjaneldelosreyes321No ratings yet
- Nicu DoccumentationDocument17 pagesNicu Doccumentationchaarvi100% (1)
- 7.health Management Information SystemDocument18 pages7.health Management Information SystemBENDOR MOSESNo ratings yet
- Session 1Document19 pagesSession 1josephat mgimbaNo ratings yet
- Unit 2 Collection, Classification, and Presentation of Data: StructureDocument20 pagesUnit 2 Collection, Classification, and Presentation of Data: Structurejazz440No ratings yet
- Lecture 2, SamplingDocument29 pagesLecture 2, SamplingSheikh sNo ratings yet
- Chapter One: Statistics: Mathematical and Nonmathematical AspectsDocument9 pagesChapter One: Statistics: Mathematical and Nonmathematical AspectsSaif Hasan JyotiNo ratings yet
- Documenting and ReportingDocument3 pagesDocumenting and ReportingGLADYS GARCIANo ratings yet
- Phase 2 LEARN OverviewDocument9 pagesPhase 2 LEARN OverviewJenny AbdullahNo ratings yet
- HESM 375 Mid Term Study NotesDocument4 pagesHESM 375 Mid Term Study NotesJenny PriorNo ratings yet
- Big Data Technologies in Health and BiomedicalDocument7 pagesBig Data Technologies in Health and BiomedicalAJER JOURNALNo ratings yet
- National Immunization Program: Manual of Procedures Booklet 7Document32 pagesNational Immunization Program: Manual of Procedures Booklet 7Blue PielagoNo ratings yet
- Introduction To StatisticsDocument7 pagesIntroduction To StatisticsKingsley RNo ratings yet
- Unity 5 HmisDocument38 pagesUnity 5 HmisJoseph MuzabulaNo ratings yet
- Advanced Statistics Las Q1Document75 pagesAdvanced Statistics Las Q1Mark Joseph BaromaNo ratings yet
- Documentation & Reporting in Nursing: PurposesDocument5 pagesDocumentation & Reporting in Nursing: PurposesMeike ElfkyuminMvp's BanabestfriendmelodyNo ratings yet
- Establishing A Surveillance System1Document4 pagesEstablishing A Surveillance System1Moff NyabutoNo ratings yet
- Documenting and ReportingDocument5 pagesDocumenting and ReportingElla LobenariaNo ratings yet
- Introduction To Health AssessmentDocument3 pagesIntroduction To Health AssessmentAngela SaavedraNo ratings yet
- Tuberculosis Programme Review (Joint Monitoring Mission)Document48 pagesTuberculosis Programme Review (Joint Monitoring Mission)Jake TolentinoNo ratings yet
- Chapter ObjectivesDocument7 pagesChapter ObjectivesLakshay PawarNo ratings yet
- Documenting and ReportingDocument17 pagesDocumenting and ReportingalelichengNo ratings yet
- And The Experimental Method. The First Is A Carefully Planned andDocument15 pagesAnd The Experimental Method. The First Is A Carefully Planned andSharadananda MondalNo ratings yet
- The Nursing ProcessDocument94 pagesThe Nursing Processmutlabans100% (1)
- P4-S1-Surveilan Epid-Manajemen Sistem Surveilan Dan Kendali Mutu Data Surveilan (Autosaved)Document26 pagesP4-S1-Surveilan Epid-Manajemen Sistem Surveilan Dan Kendali Mutu Data Surveilan (Autosaved)ambar fahanikaNo ratings yet
- Sta 111 - NDS, DCS, Dce, DFST, DSGDocument39 pagesSta 111 - NDS, DCS, Dce, DFST, DSGsalihumusazabo215No ratings yet
- Documentation & Reporting in Nursing - EFNDocument4 pagesDocumentation & Reporting in Nursing - EFNadellia onyNo ratings yet
- Chapter Two To Five EditedDocument23 pagesChapter Two To Five EditedAbdullahi AwwalNo ratings yet
- Documenting and Reporting: CommunicationDocument5 pagesDocumenting and Reporting: CommunicationDanielle Cachero100% (1)
- LO4. Monitor Family Planning ServicesDocument20 pagesLO4. Monitor Family Planning ServicesMehalu Fentaw BerihunNo ratings yet
- Annotated Example of An M&E Matrix: AnnexDocument12 pagesAnnotated Example of An M&E Matrix: AnnexbqdianzNo ratings yet
- Meaningful Use Risks - Internal Audit Assessment and ResponseDocument32 pagesMeaningful Use Risks - Internal Audit Assessment and ResponseSpit FireNo ratings yet
- Learning Guide#2Document26 pagesLearning Guide#2berhanezemichaelNo ratings yet
- Perform Nursing AssessmentDocument81 pagesPerform Nursing AssessmentAhmanur SuleNo ratings yet
- L6 HMIS Monitoring and EvaluationDocument5 pagesL6 HMIS Monitoring and EvaluationVera June RañesesNo ratings yet
- Midterms - HA LabDocument17 pagesMidterms - HA LabMa. Daniela De la CernaNo ratings yet
- Module Develop and Manage Information SystemDocument10 pagesModule Develop and Manage Information Systemwehabrebi awelNo ratings yet
- Mathematics 7: Quarter 4 - Week 1 Introduction To Statistics CompetencyDocument4 pagesMathematics 7: Quarter 4 - Week 1 Introduction To Statistics CompetencyRolando LeyvaNo ratings yet
- Illustration 2: Tentative Theme of The Project: Invisible Work Force in Your AreaDocument15 pagesIllustration 2: Tentative Theme of The Project: Invisible Work Force in Your AreaSharadananda MondalNo ratings yet
- CHN Midterm Partt1Document54 pagesCHN Midterm Partt1Mica PerezNo ratings yet
- Fundamental Concepts of StatisticsDocument24 pagesFundamental Concepts of StatisticsZeroNo ratings yet
- Principles of Health Management: Mokhlis Al Adham Pharmacist, MPHDocument43 pagesPrinciples of Health Management: Mokhlis Al Adham Pharmacist, MPHsupremeerrorNo ratings yet
- Proper-Documentation HandoutDocument2 pagesProper-Documentation HandoutKate LagundiNo ratings yet
- The Nature of Secondary Sources of InformationDocument6 pagesThe Nature of Secondary Sources of InformationSingh ViratNo ratings yet
- Data Gathering Methods: Method Description TipsDocument12 pagesData Gathering Methods: Method Description TipsJason HuffNo ratings yet
- Documentation in Psychiatric Mental Health Nursing Practice: Course Unit 13Document15 pagesDocumentation in Psychiatric Mental Health Nursing Practice: Course Unit 13MARIA STEPHANY DELA CRUZNo ratings yet
- Media Studies Coursework Evaluation ExampleDocument7 pagesMedia Studies Coursework Evaluation Examplefvntkabdf100% (2)
- Lab 13 Marshall Mix DesignDocument32 pagesLab 13 Marshall Mix DesignOtomen Yan Yan100% (9)
- 141 Islam Resighted Bruce B Lawrence.15204909 Review Shahab AhmedDocument9 pages141 Islam Resighted Bruce B Lawrence.15204909 Review Shahab AhmedKevin MoggNo ratings yet
- GAVC 1200 Functional Description - 1518165531 - 687c34ad PDFDocument21 pagesGAVC 1200 Functional Description - 1518165531 - 687c34ad PDFAhsan SiddiquiNo ratings yet
- Jesus Asks, What Are You Doing To Promote Devotion To My MotherDocument5 pagesJesus Asks, What Are You Doing To Promote Devotion To My MotherThe Fatima CenterNo ratings yet
- RULE 69 Partition CasesDocument43 pagesRULE 69 Partition CasesSamantha ReyesNo ratings yet
- Introduction To Engineering MechanicsDocument20 pagesIntroduction To Engineering MechanicsMAHVISH SADAFNo ratings yet
- Nova ProfilesDocument2 pagesNova ProfilesManish ManandharNo ratings yet
- Judicial Activism Draft1Document15 pagesJudicial Activism Draft1vijay sathyaNo ratings yet
- 9.executive SummaryDocument4 pages9.executive SummaryJhay Dee XhiaoNo ratings yet
- 1.5 Necklace Part 1 2023 EnglishDocument3 pages1.5 Necklace Part 1 2023 EnglishPari GuptaNo ratings yet
- template-SHS COURSE OUTLINE NewDocument6 pagestemplate-SHS COURSE OUTLINE NewAkosiSimon SolivaNo ratings yet
- Worksheet - 1: Diversity in Living OrganismsDocument6 pagesWorksheet - 1: Diversity in Living OrganismsDharmendra SinghNo ratings yet
- Lord's SupperDocument1 pageLord's SupperJesus LivesNo ratings yet
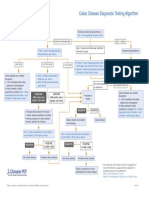
- Celiac Disease Diagnostic Testing AlgorithmDocument1 pageCeliac Disease Diagnostic Testing AlgorithmtarogiosdrakNo ratings yet
- HEC HMS Manual Costa CountyDocument56 pagesHEC HMS Manual Costa CountyHéctor M. PauthNo ratings yet
- Sharp Writeview EL-W535 ManualDocument2 pagesSharp Writeview EL-W535 ManualJkPhoenixNo ratings yet
- Datuin and Zarco Ecoframe Landslides Sept2019Document49 pagesDatuin and Zarco Ecoframe Landslides Sept2019Isaiah Emmanuel SuguitanNo ratings yet
- The Class - A Film To Teach and InspireDocument4 pagesThe Class - A Film To Teach and InspireJuhiduhNo ratings yet
- RococoDocument1 pageRococoSongJaerimNo ratings yet
- Pidilite Internship Report - SalesDocument28 pagesPidilite Internship Report - SalesAnuragNo ratings yet
- Gas Turbine Control System1 - NemaDocument50 pagesGas Turbine Control System1 - Nemaveerclaire100% (1)
- Gonzales Vs COMELECDocument3 pagesGonzales Vs COMELECNICHOL URIEL MUÑOZNo ratings yet
- CBS Grand Conversations PDFDocument8 pagesCBS Grand Conversations PDFShin Jeon HyeNo ratings yet
- Triptico PDFDocument2 pagesTriptico PDFana idalia yzaguirre vegaNo ratings yet
- Book ListDocument53 pagesBook ListfilologicNo ratings yet
- Plantillas Odoo Leah Beauty & Boutique (Productos y Usuarios)Document85 pagesPlantillas Odoo Leah Beauty & Boutique (Productos y Usuarios)Policarpio LazalaNo ratings yet
- Full SubtractorDocument6 pagesFull SubtractorPrerna Sharma100% (1)
- Man A Trinity (Spirit, Soul, Body) - BibleDocument5 pagesMan A Trinity (Spirit, Soul, Body) - BibleErol Mazhar AksoyNo ratings yet























































































Download as pdf or txt
You might also like
- Sparks Taylors Nursing Diagnosis Pocket Guide 3rd Edition Ebook PDFDocument61 pagesSparks Taylors Nursing Diagnosis Pocket Guide 3rd Edition Ebook PDFzelma.bennett128100% (48)
- Review of A Little Book For New TheologiansDocument3 pagesReview of A Little Book For New Theologianscreative2009No ratings yet
- Bodart Et Al. - 2000 - Identifying Information Needs and IndicatorsDocument24 pagesBodart Et Al. - 2000 - Identifying Information Needs and IndicatorsEvan Baros IrawanNo ratings yet
- Learning Guide #55: Nursing Level IiiDocument8 pagesLearning Guide #55: Nursing Level IiiSamuel MergaNo ratings yet
- Analyze & Interprete Pro - Data-EditedDocument32 pagesAnalyze & Interprete Pro - Data-EditedFelekePhiliphosNo ratings yet
- Group 5 (FE64) - Descriptive StatisticsDocument10 pagesGroup 5 (FE64) - Descriptive StatisticsVũ GiangNo ratings yet
- Data Analysis and Use Training GuidelinesDocument23 pagesData Analysis and Use Training GuidelinesFadhil ChiwangaNo ratings yet
- Biostat Chapter 1-7Document85 pagesBiostat Chapter 1-7Kassa GebreyesusNo ratings yet
- Anjali f9Document29 pagesAnjali f9NEERNo ratings yet
- Analyze and Interpret Production DataDocument16 pagesAnalyze and Interpret Production DataFelekePhiliphosNo ratings yet
- Health Data FirstDocument30 pagesHealth Data FirstSamuel MergaNo ratings yet
- Week 1011 Guidelines Protocols Tools in Documentation Related To Client CareDocument59 pagesWeek 1011 Guidelines Protocols Tools in Documentation Related To Client CareobnimagashelinaNo ratings yet
- Tugas Sistem Informasi KesehatanDocument37 pagesTugas Sistem Informasi Kesehatandewi shintaNo ratings yet
- Executive Briefer ILCDocument2 pagesExecutive Briefer ILCjohnllenalcantaraNo ratings yet
- Comp. StatsDocument9 pagesComp. Statsjaneldelosreyes321No ratings yet
- Nicu DoccumentationDocument17 pagesNicu Doccumentationchaarvi100% (1)
- 7.health Management Information SystemDocument18 pages7.health Management Information SystemBENDOR MOSESNo ratings yet
- Session 1Document19 pagesSession 1josephat mgimbaNo ratings yet
- Unit 2 Collection, Classification, and Presentation of Data: StructureDocument20 pagesUnit 2 Collection, Classification, and Presentation of Data: Structurejazz440No ratings yet
- Lecture 2, SamplingDocument29 pagesLecture 2, SamplingSheikh sNo ratings yet
- Chapter One: Statistics: Mathematical and Nonmathematical AspectsDocument9 pagesChapter One: Statistics: Mathematical and Nonmathematical AspectsSaif Hasan JyotiNo ratings yet
- Documenting and ReportingDocument3 pagesDocumenting and ReportingGLADYS GARCIANo ratings yet
- Phase 2 LEARN OverviewDocument9 pagesPhase 2 LEARN OverviewJenny AbdullahNo ratings yet
- HESM 375 Mid Term Study NotesDocument4 pagesHESM 375 Mid Term Study NotesJenny PriorNo ratings yet
- Big Data Technologies in Health and BiomedicalDocument7 pagesBig Data Technologies in Health and BiomedicalAJER JOURNALNo ratings yet
- National Immunization Program: Manual of Procedures Booklet 7Document32 pagesNational Immunization Program: Manual of Procedures Booklet 7Blue PielagoNo ratings yet
- Introduction To StatisticsDocument7 pagesIntroduction To StatisticsKingsley RNo ratings yet
- Unity 5 HmisDocument38 pagesUnity 5 HmisJoseph MuzabulaNo ratings yet
- Advanced Statistics Las Q1Document75 pagesAdvanced Statistics Las Q1Mark Joseph BaromaNo ratings yet
- Documentation & Reporting in Nursing: PurposesDocument5 pagesDocumentation & Reporting in Nursing: PurposesMeike ElfkyuminMvp's BanabestfriendmelodyNo ratings yet
- Establishing A Surveillance System1Document4 pagesEstablishing A Surveillance System1Moff NyabutoNo ratings yet
- Documenting and ReportingDocument5 pagesDocumenting and ReportingElla LobenariaNo ratings yet
- Introduction To Health AssessmentDocument3 pagesIntroduction To Health AssessmentAngela SaavedraNo ratings yet
- Tuberculosis Programme Review (Joint Monitoring Mission)Document48 pagesTuberculosis Programme Review (Joint Monitoring Mission)Jake TolentinoNo ratings yet
- Chapter ObjectivesDocument7 pagesChapter ObjectivesLakshay PawarNo ratings yet
- Documenting and ReportingDocument17 pagesDocumenting and ReportingalelichengNo ratings yet
- And The Experimental Method. The First Is A Carefully Planned andDocument15 pagesAnd The Experimental Method. The First Is A Carefully Planned andSharadananda MondalNo ratings yet
- The Nursing ProcessDocument94 pagesThe Nursing Processmutlabans100% (1)
- P4-S1-Surveilan Epid-Manajemen Sistem Surveilan Dan Kendali Mutu Data Surveilan (Autosaved)Document26 pagesP4-S1-Surveilan Epid-Manajemen Sistem Surveilan Dan Kendali Mutu Data Surveilan (Autosaved)ambar fahanikaNo ratings yet
- Sta 111 - NDS, DCS, Dce, DFST, DSGDocument39 pagesSta 111 - NDS, DCS, Dce, DFST, DSGsalihumusazabo215No ratings yet
- Documentation & Reporting in Nursing - EFNDocument4 pagesDocumentation & Reporting in Nursing - EFNadellia onyNo ratings yet
- Chapter Two To Five EditedDocument23 pagesChapter Two To Five EditedAbdullahi AwwalNo ratings yet
- Documenting and Reporting: CommunicationDocument5 pagesDocumenting and Reporting: CommunicationDanielle Cachero100% (1)
- LO4. Monitor Family Planning ServicesDocument20 pagesLO4. Monitor Family Planning ServicesMehalu Fentaw BerihunNo ratings yet
- Annotated Example of An M&E Matrix: AnnexDocument12 pagesAnnotated Example of An M&E Matrix: AnnexbqdianzNo ratings yet
- Meaningful Use Risks - Internal Audit Assessment and ResponseDocument32 pagesMeaningful Use Risks - Internal Audit Assessment and ResponseSpit FireNo ratings yet
- Learning Guide#2Document26 pagesLearning Guide#2berhanezemichaelNo ratings yet
- Perform Nursing AssessmentDocument81 pagesPerform Nursing AssessmentAhmanur SuleNo ratings yet
- L6 HMIS Monitoring and EvaluationDocument5 pagesL6 HMIS Monitoring and EvaluationVera June RañesesNo ratings yet
- Midterms - HA LabDocument17 pagesMidterms - HA LabMa. Daniela De la CernaNo ratings yet
- Module Develop and Manage Information SystemDocument10 pagesModule Develop and Manage Information Systemwehabrebi awelNo ratings yet
- Mathematics 7: Quarter 4 - Week 1 Introduction To Statistics CompetencyDocument4 pagesMathematics 7: Quarter 4 - Week 1 Introduction To Statistics CompetencyRolando LeyvaNo ratings yet
- Illustration 2: Tentative Theme of The Project: Invisible Work Force in Your AreaDocument15 pagesIllustration 2: Tentative Theme of The Project: Invisible Work Force in Your AreaSharadananda MondalNo ratings yet
- CHN Midterm Partt1Document54 pagesCHN Midterm Partt1Mica PerezNo ratings yet
- Fundamental Concepts of StatisticsDocument24 pagesFundamental Concepts of StatisticsZeroNo ratings yet
- Principles of Health Management: Mokhlis Al Adham Pharmacist, MPHDocument43 pagesPrinciples of Health Management: Mokhlis Al Adham Pharmacist, MPHsupremeerrorNo ratings yet
- Proper-Documentation HandoutDocument2 pagesProper-Documentation HandoutKate LagundiNo ratings yet
- The Nature of Secondary Sources of InformationDocument6 pagesThe Nature of Secondary Sources of InformationSingh ViratNo ratings yet
- Data Gathering Methods: Method Description TipsDocument12 pagesData Gathering Methods: Method Description TipsJason HuffNo ratings yet
- Documentation in Psychiatric Mental Health Nursing Practice: Course Unit 13Document15 pagesDocumentation in Psychiatric Mental Health Nursing Practice: Course Unit 13MARIA STEPHANY DELA CRUZNo ratings yet
- Media Studies Coursework Evaluation ExampleDocument7 pagesMedia Studies Coursework Evaluation Examplefvntkabdf100% (2)
- Lab 13 Marshall Mix DesignDocument32 pagesLab 13 Marshall Mix DesignOtomen Yan Yan100% (9)
- 141 Islam Resighted Bruce B Lawrence.15204909 Review Shahab AhmedDocument9 pages141 Islam Resighted Bruce B Lawrence.15204909 Review Shahab AhmedKevin MoggNo ratings yet
- GAVC 1200 Functional Description - 1518165531 - 687c34ad PDFDocument21 pagesGAVC 1200 Functional Description - 1518165531 - 687c34ad PDFAhsan SiddiquiNo ratings yet
- Jesus Asks, What Are You Doing To Promote Devotion To My MotherDocument5 pagesJesus Asks, What Are You Doing To Promote Devotion To My MotherThe Fatima CenterNo ratings yet
- RULE 69 Partition CasesDocument43 pagesRULE 69 Partition CasesSamantha ReyesNo ratings yet
- Introduction To Engineering MechanicsDocument20 pagesIntroduction To Engineering MechanicsMAHVISH SADAFNo ratings yet
- Nova ProfilesDocument2 pagesNova ProfilesManish ManandharNo ratings yet
- Judicial Activism Draft1Document15 pagesJudicial Activism Draft1vijay sathyaNo ratings yet
- 9.executive SummaryDocument4 pages9.executive SummaryJhay Dee XhiaoNo ratings yet
- 1.5 Necklace Part 1 2023 EnglishDocument3 pages1.5 Necklace Part 1 2023 EnglishPari GuptaNo ratings yet
- template-SHS COURSE OUTLINE NewDocument6 pagestemplate-SHS COURSE OUTLINE NewAkosiSimon SolivaNo ratings yet
- Worksheet - 1: Diversity in Living OrganismsDocument6 pagesWorksheet - 1: Diversity in Living OrganismsDharmendra SinghNo ratings yet
- Lord's SupperDocument1 pageLord's SupperJesus LivesNo ratings yet
- Celiac Disease Diagnostic Testing AlgorithmDocument1 pageCeliac Disease Diagnostic Testing AlgorithmtarogiosdrakNo ratings yet
- HEC HMS Manual Costa CountyDocument56 pagesHEC HMS Manual Costa CountyHéctor M. PauthNo ratings yet
- Sharp Writeview EL-W535 ManualDocument2 pagesSharp Writeview EL-W535 ManualJkPhoenixNo ratings yet
- Datuin and Zarco Ecoframe Landslides Sept2019Document49 pagesDatuin and Zarco Ecoframe Landslides Sept2019Isaiah Emmanuel SuguitanNo ratings yet
- The Class - A Film To Teach and InspireDocument4 pagesThe Class - A Film To Teach and InspireJuhiduhNo ratings yet
- RococoDocument1 pageRococoSongJaerimNo ratings yet
- Pidilite Internship Report - SalesDocument28 pagesPidilite Internship Report - SalesAnuragNo ratings yet
- Gas Turbine Control System1 - NemaDocument50 pagesGas Turbine Control System1 - Nemaveerclaire100% (1)
- Gonzales Vs COMELECDocument3 pagesGonzales Vs COMELECNICHOL URIEL MUÑOZNo ratings yet
- CBS Grand Conversations PDFDocument8 pagesCBS Grand Conversations PDFShin Jeon HyeNo ratings yet
- Triptico PDFDocument2 pagesTriptico PDFana idalia yzaguirre vegaNo ratings yet
- Book ListDocument53 pagesBook ListfilologicNo ratings yet
- Plantillas Odoo Leah Beauty & Boutique (Productos y Usuarios)Document85 pagesPlantillas Odoo Leah Beauty & Boutique (Productos y Usuarios)Policarpio LazalaNo ratings yet
- Full SubtractorDocument6 pagesFull SubtractorPrerna Sharma100% (1)
- Man A Trinity (Spirit, Soul, Body) - BibleDocument5 pagesMan A Trinity (Spirit, Soul, Body) - BibleErol Mazhar AksoyNo ratings yet