Download as pdf or txt
You might also like
- Lenovo ThinkPad T480 01YR328 NM B501Document104 pagesLenovo ThinkPad T480 01YR328 NM B501rishi vaghelaNo ratings yet
- (03241750 - Acta Medica Bulgarica) Minimally Invasive Radiofrequency Ablation For Large Thyroid Toxic AdenomaDocument3 pages(03241750 - Acta Medica Bulgarica) Minimally Invasive Radiofrequency Ablation For Large Thyroid Toxic AdenomaTeodorNo ratings yet
- Pediatric Nasopharyngeal Carcinoma Treated With Proton Beam Therapy Two Case ReportsDocument5 pagesPediatric Nasopharyngeal Carcinoma Treated With Proton Beam Therapy Two Case ReportsJesse Helmut Hansen-BartelNo ratings yet
- Se Hacía Biopsia A Los Tres Meses. Estudio Pequeño ADocument5 pagesSe Hacía Biopsia A Los Tres Meses. Estudio Pequeño Aouf81No ratings yet
- Fulltext Ajo v2 Id1026Document3 pagesFulltext Ajo v2 Id1026Lavenia Ellein MokiwangNo ratings yet
- Small Lung CarcinomaDocument4 pagesSmall Lung CarcinomaFawzia Haznah Nurul ImaniNo ratings yet
- SC 201543Document7 pagesSC 201543esinsubozatliNo ratings yet
- Concurrent Radiotherapy and Weekly Paclitaxel For Locally Advanced Squmous Cell Carcinoma of Uterine Cervix-Treated Patients at Rural Centre in IndiaDocument5 pagesConcurrent Radiotherapy and Weekly Paclitaxel For Locally Advanced Squmous Cell Carcinoma of Uterine Cervix-Treated Patients at Rural Centre in IndiaIjsrnet EditorialNo ratings yet
- Case Report A Rare Case of Metastatic Primary Peritoneal Ependymoma: A Case Report and Literature ReviewDocument8 pagesCase Report A Rare Case of Metastatic Primary Peritoneal Ependymoma: A Case Report and Literature Reviewnurul auliaNo ratings yet
- Gil 2013Document1 pageGil 2013Ananth BalakrishnanNo ratings yet
- Tanum1991 (Biopsia A Todos)Document5 pagesTanum1991 (Biopsia A Todos)ouf81No ratings yet
- Artigo Carcinoma NUTDocument6 pagesArtigo Carcinoma NUTlorranatayna202201No ratings yet
- Ann Oncol 2012 Chan Vii83 5Document3 pagesAnn Oncol 2012 Chan Vii83 5Fibrianti SeputriNo ratings yet
- Inoperable Pancoast Tumors Treated With Hyperthermia-Inclusive Multimodality TherapiesDocument4 pagesInoperable Pancoast Tumors Treated With Hyperthermia-Inclusive Multimodality TherapiesFerina Mega SilviaNo ratings yet
- 3781 FullDocument6 pages3781 FullSukhvinder Singh RanaNo ratings yet
- 2867 FullDocument5 pages2867 FullAhmad FauzanNo ratings yet
- International Journal of Radiation Oncology Biology PhysicsDocument1 pageInternational Journal of Radiation Oncology Biology PhysicsAstie NomleniNo ratings yet
- Topic 5Document4 pagesTopic 5Rabia BagewadiNo ratings yet
- Slater Case Presentation Issue 1 Article For WebsiteDocument2 pagesSlater Case Presentation Issue 1 Article For Websiteapi-400507461No ratings yet
- Percutaneous Laser Ablation: A New Contribution To Unresectable High-Risk Metastatic Retroperitoneal Lesions?Document10 pagesPercutaneous Laser Ablation: A New Contribution To Unresectable High-Risk Metastatic Retroperitoneal Lesions?Luke DengNo ratings yet
- Successful MethotrexateDocument6 pagesSuccessful MethotrexateWinda HaeriyokoNo ratings yet
- Medical Treatment Versus Radiofrequency Ablation For Patients With Trigeminal Neuralgia: A Prospective Clinical StudyDocument5 pagesMedical Treatment Versus Radiofrequency Ablation For Patients With Trigeminal Neuralgia: A Prospective Clinical StudyasclepiuspdfsNo ratings yet
- Prognostic Model For Survival of Local Recurrent Nasopharyngeal Carcinoma With Intensity-Modulated RadiotherapyDocument7 pagesPrognostic Model For Survival of Local Recurrent Nasopharyngeal Carcinoma With Intensity-Modulated Radiotherapypp kabsemarangNo ratings yet
- Cisplatin-Based Chemoradiation Plus Cetuximab in Head and Neck Cancer Ann Oncol-2010-Merlano-annonc - mdq412Document6 pagesCisplatin-Based Chemoradiation Plus Cetuximab in Head and Neck Cancer Ann Oncol-2010-Merlano-annonc - mdq412ZuriNo ratings yet
- Wagner1994 (No Hace Biopsia)Document7 pagesWagner1994 (No Hace Biopsia)ouf81No ratings yet
- Acg Poster PD1 Final 2021Document1 pageAcg Poster PD1 Final 2021prithwish ghoshNo ratings yet
- Histologically-Diagnosed Psoriasiform Dermatitis Induced by Nivolumab Successfully Controlled by Etanercept - A Case ReportDocument2 pagesHistologically-Diagnosed Psoriasiform Dermatitis Induced by Nivolumab Successfully Controlled by Etanercept - A Case ReportM CostantinoNo ratings yet
- Dysphagia: Impact On Quality of Life After Radio (Chemo) Therapy of Head and Neck CancerDocument7 pagesDysphagia: Impact On Quality of Life After Radio (Chemo) Therapy of Head and Neck CancerNurul Afika LubisNo ratings yet
- 4451 FullDocument4 pages4451 FullSukhvinder Singh RanaNo ratings yet
- Dosimetry of Yttrium-Labelled Radiopharmaceuticals For Internal Therapy: Yor Y Imaging?Document12 pagesDosimetry of Yttrium-Labelled Radiopharmaceuticals For Internal Therapy: Yor Y Imaging?sayed hossein hashemiNo ratings yet
- TB Se Defiende BiopsiaDocument7 pagesTB Se Defiende Biopsiaouf81No ratings yet
- Assignment On Radiation TherapyDocument16 pagesAssignment On Radiation TherapyAxsa AlexNo ratings yet
- Technique ChemotherapyDocument62 pagesTechnique Chemotherapyyunia chairunnisaNo ratings yet
- Chassot 2012Document9 pagesChassot 2012docadax848No ratings yet
- Paper Nuclear PhysicsDocument6 pagesPaper Nuclear PhysicsPurbandiniNo ratings yet
- Lai 2009 Septation and PTBDocument5 pagesLai 2009 Septation and PTBmarvic gabitanNo ratings yet
- 660ijrobp2011y90 Model-Based Radiation Dose Correction For Yttrium-90 Microsphere Treatment of Liver Tumors With Central Necrosis - CsliuDocument9 pages660ijrobp2011y90 Model-Based Radiation Dose Correction For Yttrium-90 Microsphere Treatment of Liver Tumors With Central Necrosis - Csliu劉晉昇No ratings yet
- 10.1055@s 0032 1313634Document8 pages10.1055@s 0032 1313634lucasnegromonte0001No ratings yet
- J Radonc 2012 08 013Document8 pagesJ Radonc 2012 08 013AnharNo ratings yet
- 2011 Sun Myint Anal CAncer Follow-UpDocument5 pages2011 Sun Myint Anal CAncer Follow-UpgammasharkNo ratings yet
- Brandsma 2001Document4 pagesBrandsma 2001VoltajeNo ratings yet
- (2006) GOKDEMIR, G. Et Al. Narrowband UVB Phototherapy For Early-Stage MycosisDocument6 pages(2006) GOKDEMIR, G. Et Al. Narrowband UVB Phototherapy For Early-Stage MycosisCassandra VérasNo ratings yet
- Fundamentals of Radiation Oncol-Ogy For Neurologic ImagingDocument32 pagesFundamentals of Radiation Oncol-Ogy For Neurologic ImagingMaria Ximena SilvaNo ratings yet
- 1273 FullDocument6 pages1273 FullPrima YogiNo ratings yet
- Intensity-Modulated Radiation Therapy (Imrt) in The Treatment of Anal Cancer - Toxicity and Clinical OutcomeDocument8 pagesIntensity-Modulated Radiation Therapy (Imrt) in The Treatment of Anal Cancer - Toxicity and Clinical OutcomejunfangokuNo ratings yet
- Carrara 2012Document2 pagesCarrara 2012Samuel PernaleteNo ratings yet
- FotoDocument5 pagesFotodhaniNo ratings yet
- 6 Forastiere2003Document8 pages6 Forastiere2003RivssNo ratings yet
- BJC 2013230Document6 pagesBJC 2013230Abraham OsunaNo ratings yet
- 2011 Guias ClinicasDocument5 pages2011 Guias ClinicasJavier VegaNo ratings yet
- Kasus ADocument3 pagesKasus AHalizah DamayNo ratings yet
- EBRT in DTCDocument7 pagesEBRT in DTCElena FlorentinaNo ratings yet
- Lung Carcinoma: Radiotherapy PlanningDocument9 pagesLung Carcinoma: Radiotherapy PlanningTowhidulIslamNo ratings yet
- Esophageal 1Document5 pagesEsophageal 1Prashanth KumarNo ratings yet
- v4n4 NeoadjuvantDocument3 pagesv4n4 NeoadjuvantfaidgustisyarifNo ratings yet
- PIIS0923753419405668Document3 pagesPIIS0923753419405668Novi OktaviantiNo ratings yet
- Immunomodulatory Effect of Gaas Laser Irradiation On Tumo!' Bearing MiceDocument2 pagesImmunomodulatory Effect of Gaas Laser Irradiation On Tumo!' Bearing MiceNeven ZarkovicNo ratings yet
- Concurrent QTRXT For T3 LarynxDocument4 pagesConcurrent QTRXT For T3 LarynxporsanimedNo ratings yet
- Pinealoblastoma With Shunt Metastasis: A Case Report: e Ea e yDocument4 pagesPinealoblastoma With Shunt Metastasis: A Case Report: e Ea e yMuhammad Azhary LazuardyNo ratings yet
- Radiation TherapyDocument218 pagesRadiation Therapyjerax116No ratings yet
- Total Marrow Irradiation: A Comprehensive ReviewFrom EverandTotal Marrow Irradiation: A Comprehensive ReviewJeffrey Y. C. WongNo ratings yet
- Revelation I Excerpt PDFDocument10 pagesRevelation I Excerpt PDFMikhael ChangNo ratings yet
- PersonificationDocument33 pagesPersonificationShane Pineda100% (2)
- Iso 11124-1 2018Document14 pagesIso 11124-1 2018anon_433139120No ratings yet
- TAS Product Catalog 2020 01Document210 pagesTAS Product Catalog 2020 01ct0720054858No ratings yet
- Design and Implementation of A Distributed IOT System in AquacultureDocument7 pagesDesign and Implementation of A Distributed IOT System in AquacultureAnun YuserboNo ratings yet
- 143 Modele CV Etats Unis ResumeDocument2 pages143 Modele CV Etats Unis ResumeGaoussou SangareNo ratings yet
- Lung Sounds Auscultation - 1Document3 pagesLung Sounds Auscultation - 1George BarajazNo ratings yet
- STAAD - Pro Plates and Solid Elements (FAQ) - RAM - STAAD Wiki - RAM - STAAD - Bentley CommunitiesDocument15 pagesSTAAD - Pro Plates and Solid Elements (FAQ) - RAM - STAAD Wiki - RAM - STAAD - Bentley CommunitiesKamal RaoNo ratings yet
- Percussion Laser DrillingDocument1 pagePercussion Laser DrillingBefzzNo ratings yet
- The Secrets of Ancient Rome's Buildings - History - Smithsonian Magazine PDFDocument2 pagesThe Secrets of Ancient Rome's Buildings - History - Smithsonian Magazine PDFMarlui Faith MaglambayanNo ratings yet
- SPAP05A Sevaka - EngDocument7 pagesSPAP05A Sevaka - EngNava NarasimhaNo ratings yet
- Effects of Maize-Legume Intercrops On Termite Damage To Maize, Activityof Predatoryants and Maize Yields in UgandaDocument7 pagesEffects of Maize-Legume Intercrops On Termite Damage To Maize, Activityof Predatoryants and Maize Yields in UgandasedianpoNo ratings yet
- Pneumatic Rotary Actuators & Airmotors Radial Piston Air Motors - P1V-PDocument33 pagesPneumatic Rotary Actuators & Airmotors Radial Piston Air Motors - P1V-Ptiensy buiNo ratings yet
- Audi s6 2007 5.2l ManualDocument374 pagesAudi s6 2007 5.2l ManualMisael EspañaNo ratings yet
- Grammar Exam Pre Int PDFDocument2 pagesGrammar Exam Pre Int PDFSandra Lazovska100% (1)
- DP - X510 BrochureDocument2 pagesDP - X510 BrochureRommel SegismundoNo ratings yet
- 6-Büşra BahatDocument4 pages6-Büşra BahatAYŞE NURNo ratings yet
- Polyurea EbookDocument39 pagesPolyurea EbookJesus De la Rosa100% (1)
- Bio 2022 PreparationDocument21 pagesBio 2022 PreparationAGENT SAYONNo ratings yet
- Yangon Thanlyin Bridge 4Document50 pagesYangon Thanlyin Bridge 4ကိုနေဝင်း100% (4)
- Pia Calabarzon 7 Prs (April 12,15, 2013), Dispatch For April 15, 2013 (Monday)Document34 pagesPia Calabarzon 7 Prs (April 12,15, 2013), Dispatch For April 15, 2013 (Monday)Pia QuezonNo ratings yet
- Product Range: Trelleborg Se Aling SolutionsDocument39 pagesProduct Range: Trelleborg Se Aling SolutionssandeepNo ratings yet
- Circut Diagram For GlucometerDocument22 pagesCircut Diagram For GlucometerSaranyaNo ratings yet
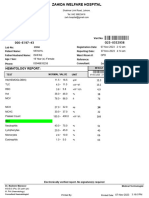
- Hematology Report:: MRN: Visit NoDocument1 pageHematology Report:: MRN: Visit Nojuniadsheikh6No ratings yet
- Logic Pro X Cheat Sheet (Atajos)Document14 pagesLogic Pro X Cheat Sheet (Atajos)Nazareno AltamiranoNo ratings yet
- Ecs2602 Tests Bank-1Document97 pagesEcs2602 Tests Bank-1corlia100% (2)
- Atlas FiltriDocument18 pagesAtlas FiltriCristi CicireanNo ratings yet
- FINAL Ulster Combined Report From STONE 12-15Document104 pagesFINAL Ulster Combined Report From STONE 12-15Watershed PostNo ratings yet
- Introduction To Privatisation and Liberalisation in India: by Anmol SharmaDocument10 pagesIntroduction To Privatisation and Liberalisation in India: by Anmol SharmaAnmol SharmaNo ratings yet